

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The suicide rate in Korea has been the highest of those among the Organization for Economic Cooperation and Development countries since 2003, and in 2013, it was 1.53 times higher than that of Japan, the country with the second-highest suicide rate.1 Although the suicide rate in Korea has decreased since 2015, suicide was the fifth leading cause of death, with 26.5 deaths per 100,000 persons, in 2015. Furthermore, more than 13,000 people died by suicide in 2015, and the number of suicide-bereaved individuals — secondary victims of suicide — is estimated to exceed 80,000 annually.23 Suicide or suicide attempts can cause physical injury and psychological trauma, increase medical and social costs, and lead to loss of life and family breakups; therefore, government policies for suicide prevention are required.4
Suicide victims and survivors differ in terms of demographic and clinical factors as well as the factors related to suicide.23 According to the analysis on suicide statistics in 2015, hanging was the most common method of successful suicide, followed by gas inhalation and jumping from heights, whereas drug overdose was most common among suicide survivors, followed by cutting and hanging.3 In addition, suicide survivors can be classified into 2 types — those whose attempts are intentional and those who engage in non-suicidal self-harm.5 As demographic and clinical data, as well as a number of factors related to suicide, differ between the 2 groups, interventions aimed at those whose attempts are intentional must take a different approach from non-suicidal self-harm interventions.5 According to the model suggested by O'Connell et al.,6 suicide is a serial process encompassing ideation, planning, attempts, and completion. Attempted suicide is the stage immediately preceding death by suicide, and a history of attempted suicide is known to be the highest predictor of further suicide attempts or death by suicide.7 Therefore, we hypothesized that suicide attempters with higher suicidal intent have similar characteristics to those who have died by completing suicide; identifying these characteristics could provide important baseline data for developing interventions for suicide prevention.
In their examination of suicide attempters, several studies have focused on suicidal intent. Sisask et al.8 reported that age is an important factor in determining suicide risk, as the strength of suicidal intent increases with age. Niméus et al.9 reported that the strength of suicidal intent is an important predictor of suicide in elderly suicide attempters. However, while numerous studies have been conducted to examine other suicide-related topics in Korea, few have focused on suicidal intent in suicide attempters. Furthermore, these studies had limitations in that they studied people who had died by suicide,1011 or had a history of attempted suicide, as opposed to current suicide attempters,12 or that they reported only the demographic and suicide-related behavioral characteristics in suicide attempters.131415 Moreover, although the Korean government has provided wide-ranging suicide statistics, in-depth data regarding the characteristics of suicide attempters are lacking; therefore, studies examining suicidal intent in suicide attempters are needed to improve the effectiveness of suicide prevention strategies.
Accordingly, this study aimed to examine the differences in demographic, suicide-related, and clinical variables, including psychological and psychosocial characteristics, based on the strength of suicidal intent in suicide attempters who had been admitted to emergency departments.
METHODS
Subjects
In total, 358 suicide attempters who had been admitted to the emergency departments at 5 university hospitals in Daegu-Gyeongbuk province between June 2011 and May 2014 were recruited for this study. Data from 6 subjects, who provided incomplete responses to the questionnaire, were excluded, and data from another 24 subjects were excluded because the strength of suicidal intent was unclear; therefore, data from 328 subjects were included in the final analysis. Upon complete recovery from the critical condition, the subjects were interviewed by the trained psychiatric resident on duty. The evaluation was performed using a structured questionnaire that included items pertaining to demographic and suicide-related characteristics, suicidal intent, lethality of the method used, and injury severity. A psychiatric specialist at each hospital verified subjects' clinical diagnoses based on the reviews of their medical records. Psychiatric diagnoses were made with reference to the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, text revision.16
Classification of suicidal intent
Suicidal intent was evaluated using the Pierce Suicide Intent Scale (PSIS)17 and a clinician-rated scale that measured suicide authenticity. The PSIS is a self-report questionnaire consisting of 12 items divided between 3 subscales (circumstances, self-report, and medical risk). The total scores range from 0 to 25, and higher scores indicate stronger current suicidal intent. Suicidal intent was classified into 3 categories: low (scores of 0–3), intermediate (scores of 4–10), and high (scores of > 10) with reference to a previous study.17 As the PSIS is a self-report questionnaire, we also used a clinician-rated scale measuring suicide authenticity, which was completed by the psychiatric residents on duty, to increase the reliability of the evaluation. The psychiatric residents who interviewed the patients completed the clinician-rated scale based on the interview, and then excluded subjects whose PSIS scores implied low suicidal intent but whom the psychiatric residents judged as being likely to commit suicide. This was similarly applied in the case of high intention. The authors wanted to use these double checks to filter out those who had tried to understate or overstate their suicidal intent.
Subjects were assigned to the low, intermediate, or high-intent groups according to their degree of suicidal intent. If the results provided by the 2 scales were inconsistent, we excluded the subject's data from the analysis because of unclear suicidal intent. Five subjects from the low-intent group whose suicide attempts were evaluated to be of high authenticity and 19 subjects from the high-intent group whose suicide attempts were evaluated to be of low authenticity were included in this category. Of the 328 subjects whose data were included in the final analysis, 63, 199, and 66 were assigned to the low, intermediate, and high-intent groups, respectively.
Evaluation scale
The principal investigator visited the 5 participating university hospitals to train the emergency department psychiatric residents in administering the questionnaires and completing the evaluations, and to test their knowledge. If there was a change in psychiatric residents on duty during the study period, the new residents also received training to minimize errors.
Hamilton Depression Rating Scale (HDRS)
The 17-item HDRS18 was developed to assess the severity of depressive symptoms and is the most widely used observer-rated depression scale. We used the Korean version of the HDRS, which was adapted and validated by Yi et al.19 to measure the severity of subjects' depressive symptoms. The total scores range from 0 to 52, and higher scores indicate depressive symptoms of greater severity. Cronbach's α of the scale was 0.70.20
Barratt Impulsiveness Scale-11 (BIS-11)
The BIS-11 is a 30-item scale developed by Barratt.21 We used 23 items from the scale, which were standardized by Lee et al.22 to measure subjects' impulsiveness. The scale measures 3 subdomains: attentional impulsiveness, motor impulsiveness, and non-planning impulsiveness. Cronbach's α of the scale was 0.78.22
Statistical analysis
In the comparison of the demographic and clinical characteristics of the 3 groups, continuous variables were analyzed using t-tests, and categorical variables were analyzed using χ2 tests. The significance of linear associations between the categories in the categorical variables was analyzed using the Mantel-Haenszel test of linear association with weighted variables. We performed binary logistic regression, with the demographic, suicide attempt-related, and mental health-related variables that differed significantly between the 3 groups included as independent variables, and calculated the odds ratios (ORs) and statistical significance to identify the risk factors that predicted high suicidal intent. Furthermore, we conducted univariate logistic regression using clinical variables that showed significant differences in group comparison analysis. Finally, multivariate logistic regression was performed by selecting the variables that significantly affected suicidal intent in the univariate logistic regression. We applied the World Health Organization's new human age criteria (0–17 years old: underage, 18–65 years old: youth/young people, ≥ 66 years old: middle-aged, elderly/senior, long-lived elderly)23 for age classification in this study. All statistical analyses were performed using PASW ver. 18.0 for Windows (IBM Co., Armonk, NY, USA) and the level of significance was set at P < 0.05.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Boards of the participating hospitals and Kyungpook National University Hospital (Reg. No. KNUH 2011-04-014-003). All subjects and caregivers received written and oral explanations regarding the study and provided written informed consent.
RESULTS
Comparison of demographic characteristics
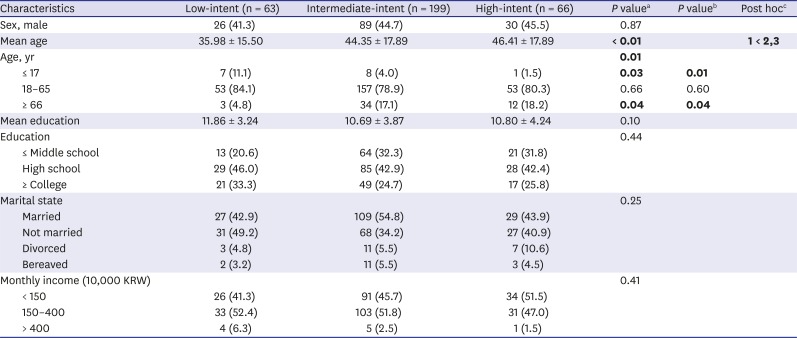
The subjects' demographic characteristics are shown in Table 1. Sex, educational levels, marital status, and income did not differ significantly between the 3 groups. The mean ages of subjects in the low, intermediate, and high-intent groups were 35.98 ± 15.50, 44.35 ± 17.89, and 46.41 ± 17.89 years, respectively, indicating a significant increase in suicidal intent with age (P < 0.01). Post hoc analysis confirmed that the subjects in the intermediate and high-intent groups were older relative to those in the low-intent group. Furthermore, the results showed a positive linear association between suicidal intent and age, as the proportion of subjects who were younger than 17 years increased as the strength of suicidal intent decreased (P = 0.01) and the proportion of subjects who were older than 66 years increased as the strength of suicidal intent increased (P = 0.04).
Table 1
Demographic data of suicide attempters by suicidal intent
Comparison of the characteristics of suicide attempts
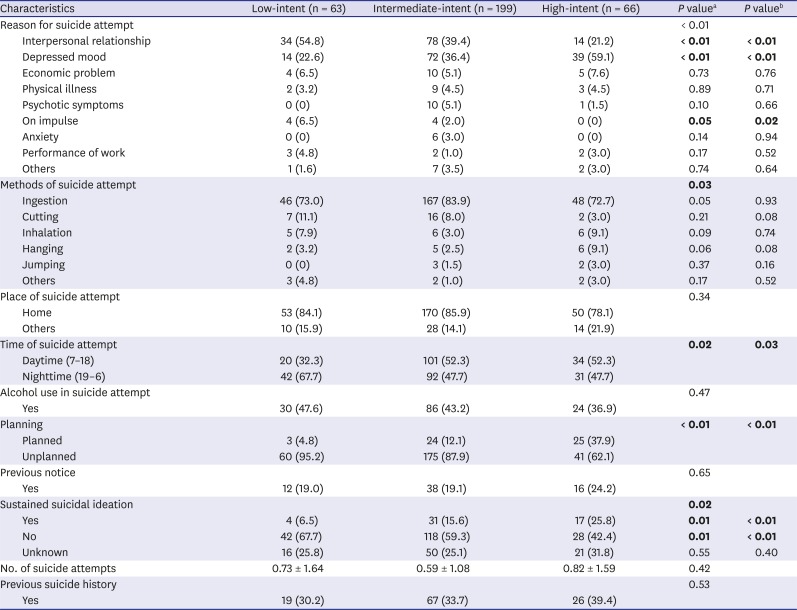
The characteristics of subjects' suicide attempts are shown in Table 2. Problems in interpersonal relationships were the most common reason for attempting suicide in the low (54.8%) and intermediate-intent (39.4%) groups, and psychiatric symptoms, such as depression, were the most common reason for attempting suicide in the high-intent group (59.1%). Problems in interpersonal relationships increased as the strength of their suicidal intent decreased, and the proportion of subjects who attempted suicide because of depression increased as the strength of their suicidal intent increased (P < 0.01). The results showed a negative linear association between the proportion of subjects who attempted suicide impulsively and the strength of suicidal intent (P = 0.02); the proportion of subjects who impulsively attempted suicide showed increasing linearity with decreasing suicidal intent. There was a significant difference in the timing of suicide attempts between the 3 groups. In the low-intent group, the proportion of subjects who attempted suicide at night (67.7%) was higher than that of subjects who attempted suicide during the day (32.3%). In the intermediate and high-intent groups, the proportion of subjects who attempted suicide during the day (52.3%) was higher than that of subjects who attempted suicide at night (47.7%). The proportion of subjects whose suicide attempts were premeditated was significantly higher in the high-intent group than in the other 2 groups (P < 0.01). The results showed linear associations between the proportion of responses indicating that the subjects intended to attempt suicide again and high suicidal intent (P < 0.01) and the proportion of responses indicating that subjects did not intend to attempt suicide again and low suicidal intent (P < 0.01).
Table 2
Characteristics of suicide attempt by suicidal intent
Comparison of mental health-related characteristics
Subjects' mental health-related characteristics are shown in Table 3. Although the proportion of subjects without a history of psychiatric treatment was the highest in all 3 groups, there were significant differences in linear trends between the groups. The results showed a linear association between the proportion of subjects without a history of psychiatric treatment and low suicidal intent (P = 0.02). Furthermore, HDRS scores differed significantly between the 3 groups, and total HDRS scores increased as the strength of suicidal intent increased (low-intent, 10.24 ± 6.20; intermediate-intent, 14.61 ± 6.17; high-intent, 19.59 ± 7.23; P < 0.01), which was confirmed in the post-hoc analysis. In contrast, there were no significant differences in the total or subscale scores on the BIS-11 between the 3 groups. The most frequently presumed diagnosis in all 3 groups was depressive disorder (low-intent, 66.2%; intermediate-intent, 73.4%; high-intent, 72.9%), followed by adjustment disorder (low-intent, 48.5%; intermediate-intent, 27.6%; high-intent, 23.5%). Furthermore, the results showed a positive linear association between the prevalence of depressive disorder and the strength of suicidal intent (P < 0.01) and a negative linear association between the prevalence of adjustment disorder and the strength of suicidal intent (P < 0.01). Psychosis, including schizophrenia, was diagnosed only in the intermediate and high-intent groups, and the results showed a positive linear association between the prevalence of psychosis and the strength of suicidal intent (P = 0.03).
Table 3
Clinical data of suicide attempters by suicidal intent
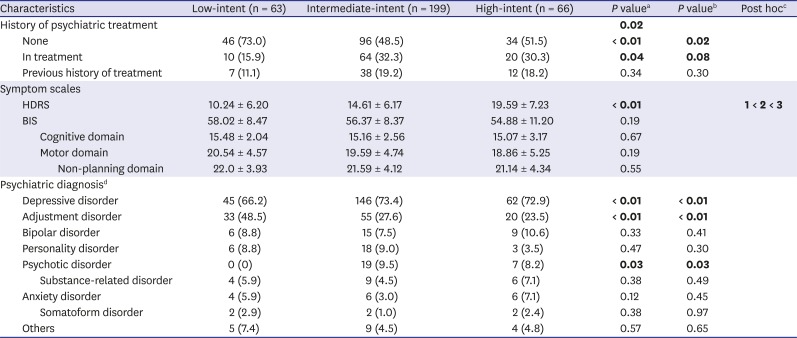
Values are presented as means ± standard deviation or number (%). Significant P values are shown in bold.
HDRS = Hamilton Depression Rating Scale, BIS = Barratt Impulsiveness Scale, CTQ = Childhood Trauma Questionnaire.
aP was calculated by a χ2 test; bP was calculated by the Mantel-Haenszel test of linear association; cAnalysis of variance and Bonferroni's post-hoc comparison were performed; dAllows multiple responses, considered up to 3 as provisional diagnosis.
Risk factors for high suicidal intent
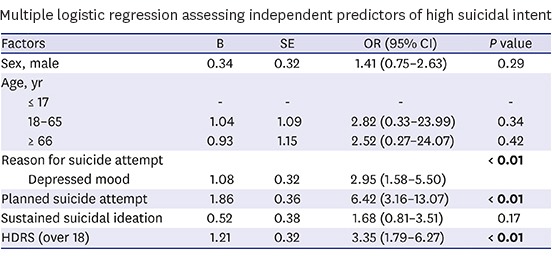
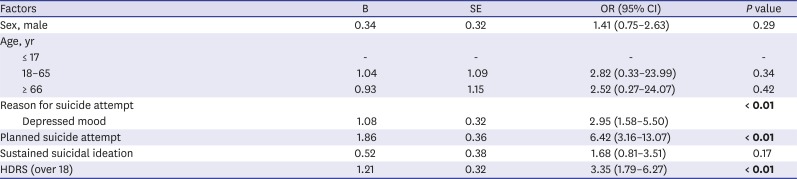
The results of the univariate logistic regression are presented in Table 4. Depressed mood as a reason for attempting suicide (OR, 2.73; P < 0.01), premeditation (OR, 5.31; P < 0.01), sustained suicidal ideation (OR, 2.24; P = 0.02) and HDRS scores of 18 or higher (OR, 3.80; P < 0.01) affected high suicidal intent. The results of the binary multivariate logistic regression analysis are shown in Table 5. Depressed mood being among the reasons for attempting suicide (OR, 2.95; P < 0.01), premeditation (OR, 6.42; P < 0.01), and HDRS scores of 18 or higher (OR, 3.35; P < 0.01) were identified as risk factors for high suicidal intent.
Table 4
Univariate logistic regression assessing independent predictors of high suicidal intent
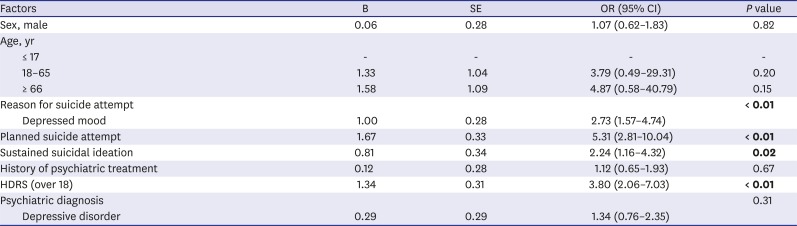
Table 5
Multiple logistic regression assessing independent predictors of high suicidal intent
DISCUSSION
This study analyzed the demographic, psychosocial, suicide-related, and clinical characteristics of 328 suicide attempters who were admitted to the emergency departments at one of the 5 university hospitals in Daegu-Gyeongbuk province. Our study used credible data based on various ratings by trained clinicians in the emergency department. The results regarding the characteristics of individuals who had attempted suicide and exhibited strong suicidal intent could serve as a theoretical foundation for the development of effective suicide prevention policies.
With regard to age, individuals who exhibited higher suicidal intent were older, on average, which is consistent with the findings of previous studies in which older people' scores on suicidal intent scales were higher than those observed in younger people.924 Similar to the existing reports, the results of the present study showed that the proportion of suicide attempters among adolescents and the elderly were high.1425 Furthermore, while the proportion of subjects who were younger than 17 years tended to increase as the strength of suicidal intent decreased, the proportion of subjects who were older than 66 years tended to increase as the strength of suicidal intent increased.
There were group differences in the main reasons for attempting suicide and the methods used in suicide attempts. Depression was reported as the reason for attempting suicide by most subjects in the high-intent group, while relationship problems were reported as the main reason for attempting suicide by subjects in the low-intent group. These results support those of previous studies in which depression was the highest risk factor for death by suicide.7262728 Some studies have reported that family relationship problems, including problems with spouses, parents, and children, were the main reason for attempted suicide.2930 However, these results could have been affected by suicidal intent. Our study suggests that relationship problems and external stress are considered the main reasons for attempted suicide, while depression is a key predictor of the severity of injury in attempted suicide. It is known that suicide methods used by people with stronger suicidal intent are more lethal relative to those used by people with weaker suicidal intent. However, in this study, there were no significant differences in suicidal methods between the 3 groups. This could be explained by the fact those with very high suicidal intent and those who had used very lethal methods generally did not agree to participate in the study. Meanwhile, there was a report31 that suicide methods are not significantly related to suicidal intent. With respect to the timing of suicide attempts, the proportion of subjects who attempted suicide at night was more than twice the proportion of subjects who attempted suicide during the day in the low-intent group. There is no consensus in the existing literature regarding the most common time of day at which suicide is attempted.3233 Considering the place where suicide attempts were most commonly made — home — the low-intent group in our study tended to attempt suicide at night, when they were more likely to be discovered or helped by caregivers.
The proportions of premeditation and subjects who expressed an intention to attempt suicide again were the highest in the high-intent group. Although the findings of some studies have indicated that suicidal intent scales are not useful for predicting suicide,3435 the findings of this study are consistent with those of studies in which people with high suicidal intent were more likely to attempt suicide repeatedly.9 Increasing numbers of suicide attempts have been revealed as a reliable predictor of future death by suicide.3637 Therefore, our findings imply that the use of active, objective evaluations of suicidal intent, as opposed to mere questioning during interviews of patients at risk of suicide, would be the most effective means of predicting future suicide risk.
With regard to the subjects' presumed diagnoses, the prevalence of depressive disorder was higher than that of other conditions in all 3 groups and increased with the strength of suicidal intent, which is consistent with the findings of previous studies wherein depression was identified as a major cause of suicide and a risk factor for death by suicide.713253134 The finding that approximately 30% of the subjects in the intermediate and high-intent groups were receiving psychiatric treatment when they attempted suicide, and none of the subjects in the low-intent group had received psychiatric treatment, suggests that a history of psychiatric treatment is a major risk factor for attempted suicide. However, rather than simply concluding that a history of psychiatric treatment per se is a risk factor, researchers and clinicians should be mindful of the fact that patients with severe depression, which can translate into high suicide risk, attend mental health clinics frequently, and that people in the early stages of the disorder who have yet to experience an improvement in their symptoms remain at risk of suicide, even if they are treated at a mental health clinic. Furthermore, it should be noted that a considerable proportion (70%) of subjects who exhibited moderate or strong suicidal intent had not attended a mental health clinic. Therefore, mental health services should be promoted more actively, and institutional measures should be implemented to facilitate access to these services as a means of suicide prevention. Furthermore, the prevalence of adjustment disorder, which was the second-most prevalent diagnosis, tended to increase as the strength of suicidal intent decreased, and adjustment disorder was the presumed diagnosis for most subjects in the low-intent group. Therefore, clinicians should carefully assess the people who have recently been exposed to stressors. Adjustment disorder generally develops within 3 months of the occurrence of a stressor, and the prognosis for patients with adjustment disorder is good with appropriate early psychiatric treatment, suggesting that this could prevent suicide attempts.
We performed a logistic regression and identified depressed mood being among the reasons for attempting suicide, premeditation, sustained suicidal ideation, and HDRS scores of 18 or higher as key predictors of high suicidal intent. Therefore, meticulous attention to and observation of individuals with high suicidal intent, who were found to be at high risk of suicide in the current study, and patients with depression and suicidal intent are essential for the prevention of suicide. Furthermore, in-depth interviews should be conducted with individuals who attempt suicide, to ascertain whether their attempts were premeditated and whether they continue to experience suicidal ideation. Sisask et al.8 and Niméus et al.9 reported that the strength of suicidal intent increases with age. In this study, the regression analysis showed that higher age is not a significant risk factor. Further consideration is needed in future studies by increasing the number of subjects.
This study has some limitations. First, it did not include suicide attempters who had died following emergency medical treatment or declined to provide consent to participate. Therefore, it is possible that a considerable number of the subjects' suicide attempts involved methods with lower levels of lethality and resulted in less severe injury relative to those of people who had died by suicide. Therefore, the findings might not be generalizable to all suicide attempters admitted to emergency departments. Second, although we provided periodic training for the evaluators and tested their knowledge, the evaluations were performed by different residents from several universities, which could have affected interrater reliability. Third, our sample size was rather small, and our retrospective data could be insufficient to confirm the variables of suicidal intent.
Despite these limitations, the study is meaningful in that it included interviews with suicide attempters admitted to emergency departments and conducted in-depth assessment according to the degree of one's intent, unlike previous studies wherein medical records were reviewed retrospectively. Suicidal thoughts, plans, and attempts are, in fact, different. It is hard to say that all the people who visit the emergency room because of a suicide attempt have high suicidal intent. In other words, many of those who visited emergency rooms were there because of non-suicidal self-harm. Such people are less likely to commit imminent suicide than high-intent attempters, which calls for different therapeutic interventions.5 Sometimes hospitalization is not necessary for them. Since previous suicide attempts are the most powerful risk factor for suicide, it is important to select a group of people who are in emergency rooms because they clearly intend to commit suicide and examine their characteristics. Kawanishi et al.38 performed a multicenter, randomized controlled trial to determine whether assertive case management is feasible in real-world clinical settings for suicidal patients with psychiatric disorders admitted to the emergency department. Although it was not effective in reducing the incidence of repetition of suicide attempts in the long term, the results of their ad-hoc analyses suggested that it was effective for up to 6 months. In Japan, since this study, the emergency-based suicide management program has been expanded with medical insurance support, which actually helped reduce the suicide rate.
This study aimed to identify the risk factors for high suicidal intent by comparing demographic and clinical characteristics between suicide attempters admitted to emergency departments. They were divided into low, intermediate, and high-intent groups according to the degree of suicidal intent. The high-intent group was older and displayed greater depressive symptoms. Also, the proportion of subjects who reported premeditated suicide attempts and continued to experience suicidal ideation was higher in the high-intent group, relative to those observed in the other 2 groups. In multivariate analysis, depressed mood, premeditation, and HDRS scores of 18 or higher were identified as risk factors for high suicidal intent. Therefore, measures that adequately reflect these risk factors would be useful in the prevention of suicide attempts in individuals with strong suicidal intent, which could ultimately reduce the suicide mortality rate.
 XML Download
XML Download