

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Varicella-zoster virus (VZV), a double-stranded DNA virus belonging to the family Herpesviridae, causes one of the most communicable diseases in humans.12 There are two distinct clinical diseases caused by VZV: varicella (or chickenpox) which is caused by the primary VZV infection as well as herpes zoster (or shingles), caused by the endogenous reactivation of the latent infection.234 Although VZV infection is generally a benign, self-limited illness in immunocompetent children, serious and life-threatening complications occur more commonly in certain groups of patients, particularly neonates, pregnant women, adults, and immunocompromised persons.56789101112 For these reasons, infection control of VZV is important in hospital settings where patients are at higher risk of severe morbidity and mortality. In addition to patients, healthcare workers (HCWs) have the potential of exposure to VZV from infected patients. Furthermore, VZV can be transmitted to and from HCWs and other susceptible patients in the hospitals. To prevent the transmission of VZV infection in the hospital settings, the development and implementation of hospital policies for appropriate infection control is warranted. This article focuses on the healthcare-associated transmission of VZV, the infection control measures in the hospital settings, and summarizes the key points of the recommendations on the management of patients and HCWs exposed to VZV.
EPIDEMIOLOGY AND CLINICAL MANIFESTATIONS
Primary VZV infection causes varicella (also known as chickenpox), which typically occurs during childhood.3 After the primary infection, VZV characteristically establishes lifelong latency in the dorsal root or cranial nerve ganglia. Reactivation of the latent virus can occur years or decades later, resulting in herpes zoster, commonly called shingles.1314
Varicella
Varicella is endemic worldwide, occurring mainly in children, and affects persons of both sexes and all races equally.15 Although the disease occurs throughout the year in temperate climates, it has a seasonal variation, with peak incidence during late winter and early spring.10 The epidemiology of varicella has changed dramatically with the implementation of the childhood varicella vaccination program. In many countries including the United States of America (USA), Germany, Australia, Greece, and Saudi Arabia, the incidence of varicella has declined following the National Immunization Program (NIP) implementation for varicella vaccine; and vaccinated persons presents with milder disease.161718192021 In Korea, a live attenuated varicella vaccine was first introduced in 1988 and the NIP recommended a universal one-dose varicella vaccination for children aged 12 to 15 months since 2005.2223 Seroprevalence, in subjects aged 1 to 79 years, determined via enzyme-linked immunosorbent assay, is about 90% in Korea.24 However, seroprevalence increased with age from 67% in those aged 1 to 4 years to > 98% in subjects aged over 20 years.24 However, the decline in incidence of varicella reported in other countries has not yet been shown by the National Notifiable Disease Surveillance System in Korea; rather, it seems to have been increasing over time.25 In the Korea Centers for Diseases Control and Prevention Infectious Diseases Surveillance Report, varicella has continued to increase from 22 cases per 100,000 population in 2006 to 155 cases per 100,000 population in 2017.25 This increase could have resulted from a number of factors including a change in the disease reporting rate due to improvement in diagnostics and surveillance, vaccine effectiveness, and waning of immunity after the only one-dose vaccination; thus, further investigation is warranted to elucidate these factors.
Varicella is characterized by a generalized pruritic rash that begins to appear on the face and trunk, then, rapidly spread to the extremities and other areas of the body. A prodrome of low-grade fever, headache, malaise, and flu-like symptoms may occur 1 to 2 days before the onset of exanthem. The skin lesions, the hallmark of varicella, are usually pruritic, and evolve from maculopapules to vesicles, pustules, and eventually scabs, over hours to days. As a result, the lesions, at all stages of evolution are found early in the disease. Most blisters would have fully crusted within one week of the onset of infection.
The severity of disease varies in certain population groups. Approximately 15%–20% of one-dose vaccinated persons may develop varicella if exposed to VZV.26 When varicella develops in vaccinated persons, the symptoms are often mild, with little or no fever. The skin lesions are fewer in number and atypical in nature, predominantly maculopapular rather than vesicular in this population. In contrast, immunocompromised patients have more numerous skin lesions, often with hemorrhagic base, and take nearly three times longer to heal. Complications occur more commonly in the following high-risk groups: neonates, adolescents, adults, pregnant women, and immunocompromised persons (including transplant recipients, patients with human immunodeficiency virus [HIV] or cancer, and patients on anti-cancer chemotherapy, immunosuppressive medications, or long-term use of steroids).592728293031 Consequently, varicella in these patients causes significant morbidity and mortality. Varicella during pregnancy affects both the mother and the fetus or newborn.112732 Maternal varicella is associated with increased risk of varicella pneumonia, which can be life threatening.11122733 If a pregnant woman has varicella during the early gestational period, the fetus is at risk of congenital varicella syndrome. Newborns who have varicella within 2 weeks of delivery from peripartum exposure or from acquisition in healthcare facilities have the highest risk of neonatal varicella.32 The mortality rate of neonatal varicella is up to 30%.632
Herpes zoster
Herpes zoster is a sporadic disease that occurs in persons who are seropositive for VZV. The mechanisms of latency and reactivation of VZV are not well known. A decline in the level of T-cell immunity to VZV presumably correlates with the reactivation of latent VZV, resulting in herpes zoster. The most important risk factor for herpes zoster is increasing age. Herpes zoster afflicts about 20% or more of the population overall, but the incidence rates progressively increase with age, particularly after 50 years of age.152434353637 Patients with medical conditions or medications that suppress the immune system also have an increased risk of herpes zoster, including patients with HIV, cancer, or autoimmune disease, transplant recipients, and patients on anti-cancer chemotherapy, immunosuppressive medications, or steroids.38394041424344 Some studies found that herpes zoster occurred more in women than in men and less in Blacks than Whites.45 Recurrence of disease is uncommon, but immunocompromised patients can experience a second and even third episode of herpes zoster.4647 The incidence rates of herpes zoster have shown a gradual increase over a long period of time in the United States.48 This trend is similarly observed in Korea. The annual number of clinical visits due to herpes zoster in Korea was reported to have increased from 7.93 cases per 1,000 population in 2003 to 12.54 cases per 1,000 population in 2007.49 The reason for this increase remains unknown. Some experts are concerned that mandatory childhood varicella vaccination could have led to the increase in herpes zoster incidence.5051 However, there are currently no data available to support this. The disease burden of herpes zoster in Korea is considerably higher than that reported for other countries.354952 The reason for this difference is not clear and further studies are needed. There are two types of vaccines licensed for the prevention of herpes zoster in the USA: Zoster Vaccine Live (live attenuated vaccine containing the Oka VZV strain with at least 14 times the potency of varicella vaccine) and Recombinant Zoster Vaccine (adjuvanted, recombinant subunit vaccine containing VZV glycoprotein E).53 In Korea, only Zoster Vaccine Live has been available since 2013. Zoster Vaccine Live is contraindicated in immunocompromised patients especially in transplant recipients because of the potential risk of disseminated VZV infection.5354
The typical clinical manifestation of herpes zoster includes painful and unilateral vesicular eruption, with a dermatomal distribution. Generally, pain precedes the erythematous maculopapular rash by 48 to 72 hours, then, the skin lesions rapidly evolve into vesicles or bullae. Although the lesions crust within 7 to 10 days in immunocompetent patients, it could take longer to heal in immunocompromised patients. Postherpetic neuralgia, the most common complications of herpes zoster, may occur in up to 50% of patients older than 50 years and can persist for more than 1 month after the skin lesions resolves.55 Occasionally, herpes zoster can become disseminated, with > 20 skin lesions beyond the primary and adjacent dermatomes or with visceral involvements.2856 Like varicella, herpes zoster in immunocompromised patients is more severe, and the risk of complications and developing disseminated zoster is higher.30435758
TRANSMISSION IN HEALTHCARE SETTINGS
VZV is highly contagious and the disease is more severe in immunocompromised patients. That is why transmission of VZV in hospitals, where potentially susceptible immunocompromised patients are housed, is a serious problem. The risk of transmission is highest in pediatric patients, and seronegative adult patients and HCWs are also at high risk for acquisition.5960 Transmission of VZV to previously vaccinated persons (breakthrough varicella) can occur.6162 A patient with either varicella or herpes zoster can be a source of transmission in healthcare settings.63646566676869 The incubation period of VZV is generally 14 to 16 days, with a range of 10 to 21 days after exposure to the characteristic rash.3 Secondary attack rates of varicella among susceptible persons within a household are between 70% and 90%.1570 There are no available data concerning the attack rate of varicella in hospital settings. Although herpes zoster is less contagious than varicella, it may however be a more frequent cause of healthcare-associated infection.6768
Transmission of VZV in hospital settings can occur via airborne route or through contact with contaminated environment or hands of HCWs. Healthcare-associated transmission from an index case with either varicella or disseminated zoster to susceptible patients or HCWs appears to be primarily through the airborne route. The virus spreads by droplets and aerosols from the nasopharynx 1 to 2 days before the onset of rash and from vesicular lesions containing large amount of virus particles. Patients with either varicella or disseminated zoster are regarded as being infectious, 48 hours before the onset of rash until all vesicles are crusted. Susceptible hosts may also acquire the virus by direct or indirect contacts with skin lesions of patients with either varicella or herpes zoster. Although rare, there have been reports of airborne transmission of VZV in hospital settings from patients with herpes zoster.697172 Some studies reported that aerosolized VZV DNA is rapidly and widely spread to the environment even from patients with herpes zoster.6973
PREVENTION AND CONTROL OF HEALTHCARE-ASSOCIATED EXPOSURES
In healthcare facilities, both HCWs and patients should be evaluated to determine the appropriate management approach for prevention and infection control of VZV infections. The major measures of infection control include isolation, varicella vaccine, varicella-zoster immune globulin (VZIG) or intravenous immune globulin (IVIG), and antiviral agents.1174757677 Definitions of key terms are summarized in Table 1.
Table 1
Definitions of key terms

HCW = healthcare worker, VZV = varicella-zoster virus.
aThe contact should be non-transient. Experts differ in the opinion about the duration of contact; some suggest 5 minutes and others up to 1 hour.28
![]()
Pre-exposure management of HCWs
HCWs with incubating or clinical varicella are significant sources of exposure to primary VZV infection in healthcare facilities. On the other hand, HCWs are at risk of acquisition of VZV infection from patients who have varicella or herpes zoster. Therefore, the first step in the prevention of healthcare-associated transmission of VZV is to minimize the number of susceptible HCWs.78 The history of prior varicella or vaccination should be determined at the time of initial employment in all HCWs. The seroprevalence of varicella among HCWs born in Korea before 1988 is reported as 96%.79 Serologic screening, such as VZV immunoglobulin G (IgG), before vaccination is indicated for persons with no or uncertain history of varicella.808182 All HCWs without evidence of immunity to VZV should receive two-doses of varicella vaccine, 4 to 8 weeks apart, unless they are contraindicated.23808183 Evidence of immunity for HCWs includes one of the followings: 1) written documentation with two-doses of vaccine, 2) laboratory evidence of immunity or laboratory confirmation of disease, 3) diagnosis or verification of history of varicella or herpes zoster by a healthcare provider.81 However, routine serologic testing after vaccination is not recommended.84 Table 2 shows the contraindications for varicella vaccination.788586
Table 2
Contraindications to varicella vaccination
![]()
Management of HCWs exposed to VZV
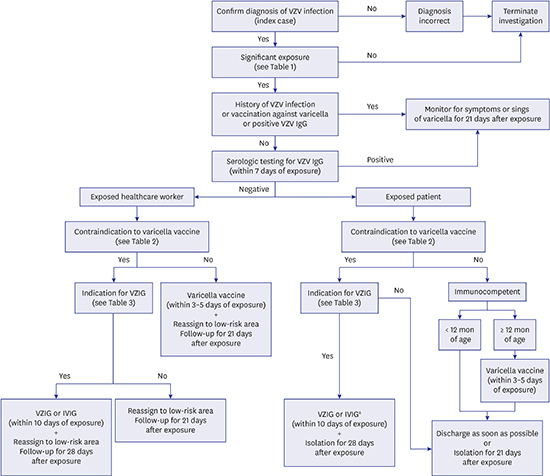
For all exposures, the potential of VZV acquisition should be assessed as soon as feasible. HCWs with evidence of immunity can be allowed to continue working and should be monitored daily for symptoms or signs of varicella, within 8 to 21 days of exposure.81 All susceptible HCWs exposed to VZV should be screened to assess their immunity to VZV. HCWs without evidence of immunity should receive two-doses of varicella vaccine within 3 to 5 days of exposure, if there are no contraindications to varicella vaccination.8187 If HCWs who have received only one dose of varicella vaccine are exposed to VZV, the second dose of vaccine is recommended within 3 to 5 days after exposure, at least 4 weeks after the first dose. Seronegative HCWs who are immunocompromised or pregnant should be considered for VZIG as soon as possible within 10 days of exposure (Table 3).81868889 Furthermore, seronegative HCWs should be considered for reassignment to low-risk areas or be placed on administrative leave from day 8 to day 21 of the exposure. VZIG may prolong the incubation period by one week, thus HCWs who receive VZIG should be excluded from work from day 8 to day 28 of the exposure. If VZV infection is suspected, the HCWs must be excluded from work immediately.6281 Suggested algorithm for the evaluation and management after exposure to VZV in healthcare settings is shown in Fig. 1.
Table 3
Indications for VZIG after an exposure to VZV

![]()
 | Fig. 1Suggested algorithm for the evaluation and management after exposure to VZV in healthcare settings.VZV = varicella-zoster virus, IVIG = intravenous immune globulin, VZIG = varicella-zoster immune globulin.
aFor immunocompromised patients, a 7-day course of acyclovir or valacyclovir may be considered if both VZIG and IVIG are not available.
|
Management of patients exposed to VZV
First, the immunologic status of all patients exposed to VZV should be assessed. Susceptible patients who are exposed to VZV should be placed on airborne and contact precautions from day 8 to day 21 of the exposure. If VZIG or IVIG is administered, these precautions should be maintained until day 28 of the exposure.90
Immunocompetent patients
The principle of management in immunocompetent patients is the same as in HCWs. In general, immunocompetent patients who have immunity to VZV need no further follow-up. All susceptible immunocompetent patients, who are 12 months of age or older, may be candidates for varicella vaccination. Varicella vaccine should be administered as soon as possible, preferably within 3 to 5 days after exposure.
Immunocompromised patients
Serologic testing should be performed in all immunocompromised patients as soon as possible. Patients without evidence of immunity to VZV and who are at high risk of complications should be administered with VZIG (Table 2).28838891 Some experts also recommend VZIG as postexposure prophylaxis for highly immunocompromised patients, such as hematopoietic stem cell transplant recipients, regardless of serologic test results. This is because the sensitivity and specificity of serologic tests are unavailable and VZV IgG may not be protective in these patients. Intramuscular administration of VZIG (1 vial [125 units] per 10 kg body weight; maximum of 5 vials) is recommended as soon as possible within 10 days.89 If VZIG is not available, IVIG (≥ 400 mg/kg) can be an alternative.2875 A 7-day course of acyclovir (800 mg 5 times daily) or valacyclovir (1 g 3 times daily), beginning 7 to 10 days after exposure may be considered as chemoprophylaxis for immunocompromised patients if both VZIG and IVIG are not available.28 However, there are no studies on postexposure chemoprophylaxis for immunocompromised patients. All susceptible patients should be placed in isolation until day 21 of exposure. In patients who receive VZIG, isolation should be continued until day 28 of exposure.
Pregnant women
Varicella vaccine is contraindicated in pregnant women and VZIG is recommended in all susceptible pregnant women exposed to VZV as soon as possible, within 10 days.111228888992 The use of VZIG could reduce both the severity of maternal disease and the risk of fetal infection. There are no studies on whether the use of acyclovir is effective in the prevention of varicella in pregnant women after exposure to VZV. Because maternal varicella infection complicated with pneumonia is a medical emergency, careful follow-up for signs of active disease despite passive immunization is needed. If maternal disease occurs despite VZIG, patients should be treated with antiviral agents. Susceptible pregnant women who do not develop varicella should receive varicella vaccine after delivery.1112
Neonates
Newborns may be infected with VZV by peripartum maternal infection or by postnatal exposure. Routine screening for maternal immunity to VZV is recommended during early pregnancy.1112 If the maternal immune status is not known, the mother should have a serologic testing for VZV as soon as possible. Because varicella vaccine has been approved for children aged 12 months through 12 years, VZIG is recommended to prevent varicella and ameliorate the disease course in neonates.88 Indications for VZIG in newborns with significant exposure to VZV are shown in Table 2.28888993 If VZIG is unavailable, IVIG or chemoprophylaxis with acyclovir could be considered.28
Infants whose mother has active varicella within 21 days prior to delivery should be isolated from other infants. If a mother has symptoms of varicella within 5 days before or 2 days after delivery, the infant should be isolated from the mother until she is no longer infectious.28
TREATMENT OF CONFIRMED OR SUSPECTED INFECTION
Work restriction and isolation precautions
All HCWs who develop varicella or disseminated zoster should be excluded from work until all lesions are crusted. Although immunocompetent hosts with dermatomal herpes zoster with covered lesions may continue to work, advice for reassignment to low-risk patients should be offered, until all lesions are crusted.59
Unvaccinated susceptible HCWs should avoid contact with patients who have confirmed or suspected varicella or herpes zoster. All patients with varicella or disseminated zoster should be placed on airborne and contact precautions until all lesions are crusted. For immunocompetent patients with dermatomal herpes zoster, standard precautions and complete covering of the skin lesions are recommended.
Antiviral therapy
HCWs and patients who develop clinical symptoms despite active or passive immunization should be appropriately treated with antiviral therapy. Antiviral therapy can shorten the duration of disease, reduce the total number of new lesions, accelerate cutaneous healing, and reduce acute neuritis.2 Acyclovir is approved for the treatment of both varicella and herpes zoster, and both oral (800 mg 5 times daily for 7 to 10 days) and intravenous (10 mg/kg every 8 hours for 7 to 10 days) forms are available. Oral valacyclovir (1 g 3 times daily for 7 to 10 days) and famciclovir (250 to 500 mg 3 times daily for 7 to 10 days), the prodrugs of acyclovir and penciclovir, have been licensed for the treatment of herpes zoster.
CONCLUSION
Despite implementation of routine childhood varicella vaccination NIP program in Korea, varicella and herpes zoster continue to occur. VZV is highly contagious and can cause serious complications in high-risk populations. Healthcare-associated transmission of VZV is also well documented from both varicella and herpes zoster. The prevention and control of VZV infection in hospital settings is important for both HCWs and in-hospital patients. All HCWs should be screened for immunity to VZV at the time of initial employment, then varicella vaccines are recommended to all seronegative HCWs, if there are no contraindications to vaccine use. Susceptible HCWs and patients exposed to VZV should be isolated from other members of staff or patients, appropriately. Active immunization should be performed when it is safe, and passive immunization can be considered, based on specific indications.
 XML Download
XML Download