

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Ambient air pollution is recognized as the major environmental health hazard in the Republic of Korea. Exposure to ambient fine particulate matter pollution (PM2.5) has been associated with increased morbidity and mortality. In 2012, the World Health Organization (WHO) announced that 1 in 8 individuals died from air pollution-related diseases, of which about 3.5 million deaths were caused by exposure to ambient air pollutants, worldwide.12 Globally, about 90% of people live in environments in which the air pollution levels do not meet the air quality guidelines of the WHO.3 Premature deaths due to air pollution occur most frequently in individuals living in Southeast Asia and the Western Pacific region, including Korea.1 The most recent global burden of disease (GBD) study ranked PM2.5 exposure as the ninth biggest risk factor affecting the total disease burden in Korea.4
PM consists of a complex mixture of metals, as well as solid and liquid particles of organic and inorganic substances suspended in the atmosphere. The components of PM that affect health are iron, nickel, and arsenic, and compounds such as elemental carbon, organic carbon, sulfate, and nitrate.56 The composition of these mixtures varies depending on the geographical location of each country, the emissions in major industrial facilities, and the amount of fossil fuels burnt for heating and transport.6789 Particles with smaller diameters penetrate more deeply into the lungs and affect health even at very low concentrations.10 Because of this, the health effects associated with ambient particles are more focused in the case of PM2.5 than in the case of PM10.
Data on PM2.5 exposure, disease mortality, and comparative risk assessments (CRAs) for each disease are required for the calculation of premature death caused by ambient air pollutants such as PM2.5.11 The CRAs for each disease caused by PM2.5 are mainly derived from long-term cohort studies, and these results are used to calculate the population attributable fraction (PAF) of PM2.5 for each disease.11 Because measurement of PM2.5 concentrations has not been long worldwide, assessment of long-term exposure in epidemiological studies related to PM2.5 exposure has been challenging.12 In the past, PM2.5 exposure has been measured in several cities using routine ground monitoring, and health effects due to long-term exposures have been estimated in cohort studies.1314 However, because the monitoring sites were mainly located in urban areas, the total area of the country could not be obtained. Hence, the level of exposure across the entire population could not be estimated. Over the last decade, models that estimate PM2.5 concentrations have been developed using satellite-based remote sensing such as aerosol optical depth (AOD), chemical transport modeling, and ground measurement data.151617 The development of methodology has enabled the estimation of long-term PM2.5 exposure in each region. In the health impact assessment, the results of several cohort studies have improved the outcome of CRA, and there has been a significant change in the methodology for estimating the number of premature deaths attributable to PM2.5 led by the Institute for Health Metrics and Evaluation (IHME) and WHO.118 In Korea, previous epidemiologic studies related to PM2.5 exposure were primarily focused on short-term exposure assessments in the metropolitan population. This study aimed to estimate the premature death attributable to long-term PM2.5 exposure in the Korean population.
METHODS
Data on exposure to ambient PM2.5
In order to assess the health effects of long-term PM2.5 exposure, it is necessary to estimate the concentration of PM2.5 in areas where no ground measurements. In Korea, data on PM2.5 were not available for the measurement of long-term exposure, as measurement of PM2.5 has been started from the 2010s, except for metropolitan areas. The only possible way to use the data was through the estimation by the modeling method. Therefore, in order to calculate PM2.5 concentrations in the past, it is required to use all available sources for estimation. The available data to estimate past PM2.5 concentrations with insufficient measurements include satellite estimated PM2.5 concentrations using AOD data, chemical transport modeling data based on emissions inventories, and data with proportionally estimated using PM10.1617 The GBD approach, which estimates the PM2.5 concentrations by making the greatest use of multiple sources of PM2.5 information in the most reasonable way possible, combined data from ground monitoring with satellite observations and chemical transport models.15 In the GBD study, satellite based estimates and chemical transport modelling results were calculated and calibrated to available ground measurements data. Estimated results were calculated as a grid of 0.1 degrees × 0.1 degrees, and then the population-weighted PM2.5 concentrations were applied reflecting the number of inhabitants.
In this study, the data on long-term PM2.5 exposure were obtained from the GBD 2013 study.15 The annual average PM2.5 exposure levels in 1990, 1995, 2000, 2005, 2010, 2011, 2012, and 2013 were derived from the combined data, and the data for the missing years were interpolated. The long-term ambient PM2.5 exposure levels were estimated using average annual population-weighted PM2.5 concentrations.
Exposure-risk relationship and PAF
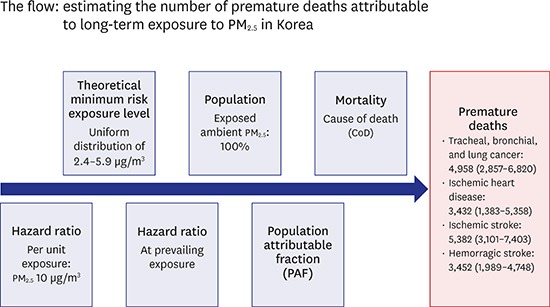
In this study, the theoretical minimum risk exposure level (TMREL) of ambient PM2.5, which can be hazardous to human health, was assumed to be the minimum exposure level achievable by modifying the environment at the current available technology level.4 The GBD 2015 study does not clearly define TMREL as a single value, rather a uniform distribution of 2.4–5.9 μg/m3.18 We applied a lower bound and upper bound of 2.4 μg/m3 and 5.9 μg/m3, respectively, as TMREL to reflect the presented distribution. Hazard ratios (HRs) per unit increment of PM2.5 were based on the exposure-response function presented in a recent large prospective cohort study (Table 1).19
Table 1
HR for each mortality due to exposure to ambient PM2.519

The PAF for mortality is the magnitude of the reduction in the number of deaths in the whole population that can be prevented when exposure to a particular hazardous environment is reduced to the counterfactual level.20 Premature death due to a particular disease is the sum of the consequences of various environmental, social, and behavioral risks. The sum of each PAF may often exceed 100%, which means that premature death could be potentially reduced or eliminated by various risk factors.20
The PAF for lung cancer, ischemic heart disease, hemorrhagic stroke, and ischemic stroke due to ambient PM2.5 were calculated using the following formula:

where Pi is the percentage of the population exposed to level i of ambient air exposure, HRi is the HR at exposure level i, and n is the total number of exposure levels.
The attributable burden (AB) was calculated by multiplying each health outcome (B) of interest and the PAF:
Mortality data
The total number of premature deaths due to long-term exposure to ambient PM2.5 by sex and age group was estimated. The number of cause-specific deaths in 2013 were estimated according to the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10). Mortality data pertaining to ischemic heart disease (I20, I21, I22, I23, I24, and I25), hemorrhagic stroke (I60, I61, I62, I690, I691, I692, and I694), ischemic stroke (I63, I65, I66, I670, I671, I672, I673, I675, I676, I677, I678, I679, and I693), and tracheal, bronchial, and lung cancer (C33 and C34) were obtained from the Statistics Korea, the national statistical office of Korea. It is important to accurately measure the cause-specific mortality to determine the number of premature deaths, using the death rate and cause of death (CoD). However, some errors can occur because data on the CoD are inaccurate. For example, CoDs such as senility or cardiac arrest may be considered as the final event in the course of death and not the root CoD; in these cases, the actual CoD is not reflected.21 Therefore, to estimate the accurate premature deaths, it is necessary to modify the CoD code in the case of the aforementioned vague CoDs. In a study on the CoD based on the 2012 Korean death registry data, about 5% were classified as having an inadequate CoD.21 The IHME used these invalid causes of deaths as “garbage codes.”22 The IHME reclassified them as valid disease codes to accurately estimate the burden of disease. However, the Korean Burden of Disease Study Group found that the IHME methodology developed for universal use does not accurately reflect the reality in each country such as Korea.21 Therefore, they devised a reclassification method to match the characteristics of the Korean population to estimate the burden of disease more accurately. In this study, we used the modified CoD data, which is computed by applying the garbage code redistribution algorithm devised by the Korean Burden of Disease Study Group.21
Uncertainty analyses
The uncertainties associated with TMREL when assessing the ambient PM2.5 exposure levels was reflected in this study. The uncertainty analysis reflected the uniform distribution of TMREL and the uncertainty pertaining to the relative risk derived from the exposure-risk function.18 The combined uncertainty intervals were calculated as 2.5th percentile and the 97.5th percentile of the results that were drawn from the premature death calculation formula and Monte Carlo simulation method.
RESULTS
Population-weighted exposure concentration
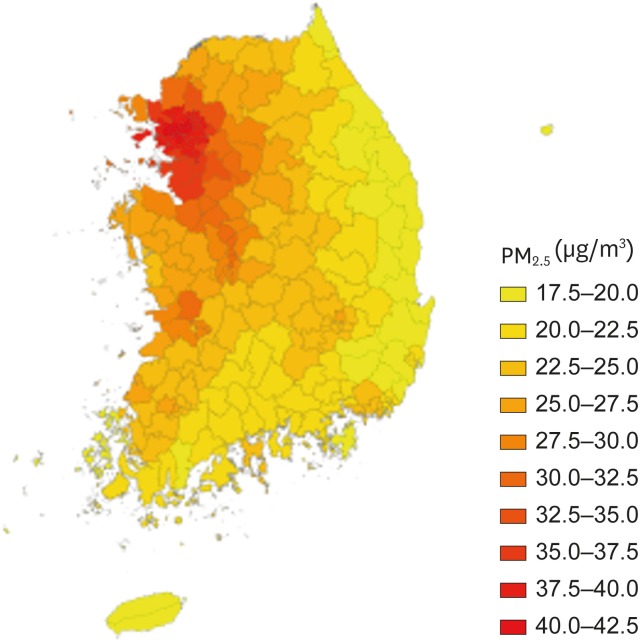
The average annual PM2.5 concentration per administrative district was estimated from 1990 to 2013. About 40% of the population in Korea are concentrated in the capital areas of Seoul, Incheon, and Gyeonggi-do. The concentration of PM2.5 is higher in capital areas compared with other regions. After calculating the population-weighted concentration of each year, the average PM2.5 exposure concentration for the whole period was estimated to be 30.2 μg/m3 (Fig. 1).
PAF
Using the estimated population-weighted PM2.5 exposure concentration and the HR function, we calculated the PAF of mortality for each CoD category. With regard to mortality, the PAF for tracheal, bronchial, and lung cancer was 0.269 (95% confidence interval [CI], 0.155–0.370); 0.139 (95% CI, 0.056–0.217) for ischemic heart disease; and 0.269 (95% CI, 0.155–0.370) for hemorrhagic stroke and ischemic stroke (Table 2).
Table 2
PAF of each disease based on the level of exposure to ambient PM2.5 in Korea (2013)

Reclassified CoD based on the mortality data
As a result of the garbage code reclassification, CoDs due to ischemic heart disease increased by 80.9%, that is, from 13,656 to 24,691 (Table 3). The CoD increased by 32.3% in ischemic stroke (from 15,128 to 20,009 deaths), 6.6% in tracheal, bronchial, and lung cancer (from 17,294 to 18,432 deaths), and 25.0% in hemorrhagic stroke (from 8,442 to 12,832 deaths). The rate of increase in the number of deaths after reclassification of garbage code was higher in females than in males.
Table 3
Garbage code reclassified mortality data in Korea (2013)

Premature deaths attributable to exposure to ambient PM2.5
The number of premature deaths due to exposure to ambient PM2.5 was estimated by applying the PAF to the total number of deaths of each related disease using the modified CoD by the garbage code redistribution algorithm. As of 2013, long-term PM2.5 exposure caused a total of 17,203 (95% CI, 11,056–22,772) premature deaths due to ischemic stroke; hemorrhagic stroke; tracheal, bronchial, and lung cancer; and ischemic heart disease. Ischemic stroke was the most common cause, which led to 5,382 (95% CI, 3,101–7,403) deaths, followed by tracheal, bronchial, and lung cancer, which led to 4,958 (95% CI, 2,857–6,820) deaths; hemorrhagic stroke, which led to 3,452 (95% CI, 1,989–4,748) deaths; and ischemic heart disease, which led to 3,432 (95% CI, 1,383–5,358) deaths (Table 4). Long-term PM2.5 exposure has led to a total of 17,224 deaths, which accounted for 6.4% of the total deaths in Korea in 2013.
Table 4
Premature deaths attributable to exposure to ambient PM2.5 in Korea (2013)

DISCUSSION
We estimated the premature deaths associated with long-term exposure to ambient PM2.5 in Korea. The population-weighted ambient PM2.5 exposure concentration from 1990 to 2013 in Korea was 30.2 μg/m3, resulting in a total annual premature death of 17,224.
As PM2.5 ground measurement data were not available in Korea before the year 2000, it was not possible to estimate the PM2.5 concentrations in the period before that. This study used exposure data of a spatial resolution of 0.1° × 0.1° coordinate, based on satellite measurement data and by applying the improved estimation algorithm provided by the GBD group.1516 In order for long-term high-resolution exposure data to be applied to the resident population, there should be little population movement. However, Korea has extreme population movements; about 15% of the total population moves in relation to new city development, change in housing and occupation, each year.23 Therefore, applying the exposure data to the resident population after calculating the long-term PM2.5 exposure concentration by region may result in biased outcomes. To resolve this issue, the population-weighted exposure concentration was calculated and applied to the whole population.
In previous GBD studies that focused on the health effects of ambient PM2.5 exposure, the TMREL reflected the smallest observable value in the area where the human residence on Earth. In the GBD 2010 study, the observable value was 5.8–8.8 μg/m3. In GBD 2015 study, however, the said value was lower (2.4–5.9 μg/m3).418 To reflect these changes, we estimated the number of premature deaths after applying a uniform distribution of 2.4–5.9 μg/m3 for TMREL.
Garbage codes occupy about 20% of the registration data pertaining to the CoD in Korea. In previous studies, the number of deaths after the garbage codes were redistributed increased by 6.5% in the case of lung cancer, 76.5% in ischemic heart disease, and 33.6% in ischemic stroke.21 The garbage code reclassification method applied in this study was the same with that applied by other Korean researchers in previous research; the reclassification of CoD showed a similar increase in our results.
Based on the results of the estimation conducted by the WHO in 2012, the number of premature deaths attributable to long-term ambient PM2.5 exposure in Korea was 11,523 (9,054–13,963).1 The number of premature deaths due to long-term ambient PM2.5 exposure, as estimated jointly by the Health Effects Institute and IHME, increased from 13,800 (11,600–16,300) in 2010 to 18,200 (15,100–21,400) in 2015.24 Although significant differences in the detailed methodology were noted during the calculation process, data on long-term exposure to ambient PM2.5 were estimated based on satellite measurements, and data on CoD were derived from the national death registry data.
In 2013, the total number of deaths in Korea was 266,000. In this study, the premature deaths due to long-term exposure to ambient PM2.5 accounted for 6.4% of the total deaths, which is much higher than the average of 4.9% in the European Union (EU) and 4.4% in the Organization for Economic Cooperation and Development (OECD) countries (Table 5).24 Premature deaths of a specific disease due to long-term exposure to ambient PM2.5 is affected by the concentration level of PM2.5 and the total number of deaths due to a specific disease. Increase in PM2.5 concentrations and increase in the total number of deaths caused by a specific disease in aging populations contribute to the increase in the number of premature deaths due to long-term exposure to ambient PM2.5. The proportion of the population aged 65 years and over in Korea, the EU, and OECD countries as of 2013 is 11.9%, 18.2%, and 15.9%, respectively.2526 The average long-term exposure concentrations of PM2.5 in Korea, EU, and OECD were 30.2 μg/m3, 15.5 μg/m3, and 15.0 μg/m3, respectively.27 Because the proportion of the population aged 65 years and over in Korea was lower than that in the EU or OECD countries, the number of premature deaths due to long-term exposure to ambient PM2.5 was caused by exposure to higher PM2.5 concentrations rather than by the higher number of deaths due to cardiovascular and respiratory diseases at older ages.
Table 5
Proportion of deaths due to long-term exposure to PM2.5 among total deaths in Korea, the EU, and OECD countries

Our study had some limitations. First, the PM2.5 exposure levels, produced by combining satellite measurements, chemical transport modeling data, and ground measurements, may have been overestimated or underestimated in relation to the actual ground measurements. However, since PM2.5 concentrations were not monitored in Korea before the year 2000, the use of satellite measurement data is the most practical solution to estimate past exposure levels and identify the health effects. Second, the combined model used to estimate the ambient PM2.5 exposure levels in this study does not reflect the exposure level according to the height from the ground.2829 According to the 2014 data, 49.6% of Koreans reside in apartments and the proportion of apartment residents in big cities is much higher than that in the rural areas.30 Therefore, when considering the housing type of Koreans, changes in PM2.5 concentrations based on height can be an important issue. Although PM2.5 concentrations differ depending on the height of the apartment, matching the estimated values at ground level can cause the overestimation of ambient PM2.5 exposures in epidemiological studies.12 Third, the exposure-risk function used in this study was obtained from the result of cohort studies conducted in North America. Therefore, the race, residential environments, and lifestyles of the target group would have been different from those of the group in Korea; in addition, emergency medical service systems and health insurance systems that can make a difference in the CoD also vary from country to country. Since, in Korea, there is no cohort study that can assess the health effects of long-term exposure to ambient PM2.5, this study applied the results of the North American study. Considering the impact of the above confounding factors, it is reasonable to apply the results of the Korean cohort studies in the future.
The Korean population entered the “aging society” category in 2000 and is on the verge of entering the “super-aged society” category. In a study conducted on the disease burden due to non-communicable diseases in Korea, the above diseases were ranked high in both sexes.31 The prevalence rates of ischemic heart disease, ischemic stroke, hemorrhagic stroke and tracheal, and bronchial and lung cancer, the major health effects of long-term PM2.5 exposure, increase with age. Considering these characteristics, damage to health caused by ambient PM2.5 exposure will further increase in the near future.32 According to a study that projected future air pollution levels, the OECD estimated that, in 2060, more than 1,000 people per 1 million population would die prematurely due to exposure to ambient PM2.5 in Korea and that this would be the highest number of cases reported across all OECD countries.33
This study used regional population data of the Korean national statistical office to estimate the population-weighted PM2.5 exposure. The garbage codes were redistributed to classify the CoD more precisely. Therefore, our reclassification method is more realistic than the global evaluation method because it reflects the regional population structure in Korea and misclassification pattern.
Unlike lifestyle-related risk factors such as smoking and high-risk drinking, the health risk from exposure to ambient PM2.5 is difficult to avoid through individual efforts alone. Establishing government policies is important in reducing the health damage caused by exposure to ambient PM2.5. The results of this study can be used as a basis for the government to promote policies and secure budgets. They can also act as tools in predicting and evaluating the health effects of future policy implementation.
 XML Download
XML Download