

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
As industry and economy progress, the nocturnal exposure to bright light increases. The night is no longer dark, particularly in densely populated areas. The amount of light emitted and entering into bedrooms during nocturnal sleep from nearby buildings, electric billboards, and streetlamps is increasing as well. If this unnecessary nocturnal light causes human or ecosystem harm, it is considered light pollution. Light pollution can affect human physiology and disturb the circadian rhythm, which influences mood, vitality, and basal temperature by regulating hormones.12 Reportedly, circadian rhythm disruption affects the neuroendocrine system and induces obesity, diabetes, depression, and cancer.
The light intensity affecting circadian rhythm is perceived by photosensitive retinal ganglion cells (PRGC), while the shape and movement of objects are recognized with retinal photoreceptor cells.3 The eye is the first sensory organ to perceive the light-dark environment, but the influence of retinal nocturnal light exposure is not thoroughly understood. Nocturnal light exposure induced refractive errors in animal studies4; whether ambient light at night also induces refractive error in humans is controversial.56 Bright light at night could disturb normal sleep and subsequently induce systemic and ocular fatigue. However, the effect of dim nocturnal light on ocular fatigue is not well established.
Ocular fatigue decreases reading performance.7 It also decreases the accuracy of eye movement and saccadic speed.8 If ambient nocturnal light exposure deteriorates visual function or induces ocular fatigue, then it may cause discomfort and decrease daily work efficiency. The tolerable level of nocturnal light for avoiding ocular fatigue and maintaining visual function is similarly unknown. The present study investigates the influence of nocturnal ambient light at 5 and 10 lux illumination on visual function and ocular fatigue.
Go to : 
METHODS
Sixty healthy subjects (30 males and 30 females) aged 19 through 29 years with no history of ocular disease were recruited. Prior to enrollment, best-corrected visual acuity with Snellen chart, and intraocular pressure with non-contact tonometry (CT-80A, Topcon Co., Tokyo, Japan) were measured on the participants. An alternate cover test at far and near distances, slit lamp examination, and fundus examination with fundus photography (TRC-NW8, Topcon Co., Tokyo, Japan) were performed. Subjects with a best-corrected visual acuity less than 20/20, corneal opacity, cataract, ocular hypertension, strabismus, and any fundus photographic abnormality were excluded.
Subjects spent 3 consecutive nights in the sleep laboratory of Korea University Hospital. During the day, subjects were educated to behave normally, taking care to avoid strenuous exercise, napping, excessive caffeine intake, alcohol consumption, and other behaviors potentially affecting sleep quality. During the first and second nights, subjects were not exposed to ambient light during sleep, but during the third night, they were. The light intensity was measured at the subjects' eyes, and the subjects were randomly allocated to one of two groups (30 subjects each), receiving 5 or 10 lux of light during sleep at night. Visual function and ocular fatigue were evaluated at 7 a.m. on the 3rd and 4th mornings. Sleep structure can become distorted in a laboratory setting during the first night of sleep (first-night effect),9 therefore the visual function and ocular fatigue examinations were not performed after the 1st night (2nd morning). The visual function was evaluated using the best-corrected visual acuity, and refractive error. Refractive error was measured using an autorefractor (RK-F1, Canon, Tokyo, Japan). The objective ocular fatigue tests included the tear break-up time (TBUT), maximal blinking interval, ocular surface temperature, and conjunctival hyperemia. A questionnaire was administered to subjects for subjective assessment of fatigue. For the TBUT measurement, the tear film was stained with a fluorescein paper, and development of the tear film break was observed using the slit lamp; the elapsed time was measured 3 times and averaged to calculate the TBUT. Maximal blinking interval was obtained by measuring the maximal time that the subject was capable of keeping the eye open without blinking. The central corneal temperature was measured at the ocular surface using the Thermal imaging system (FLIR E50, FLIR Systems, Inc., Wilsonville, OR, USA). Conjunctival hyperemia was determined on a 100-point scale previously described by Schulze et al.10 All measurements were performed on the right eye. The ocular fatigue questionnaire comprised 10 items that are the most frequently reported symptoms of ocular fatigue.11 Each item was answered using a 7-point scale (0–6). A score of 0 corresponded to no symptom, and a score 6 corresponded to an extremely severe symptom. This questionnaire had been reported previously to assess subjective ocular fatigue.12
Statistical analysis
Statistical analysis was performed using SPSS 20.0 (SPSS Inc., Chicago, IL, USA). Visual function and ocular fatigue parameter differences between the 3rd and 4th mornings were compared using the Wilcoxon signed-rank test. The magnitude of change in visual function and ocular fatigue between subjects exposed to 5 lux and 10 lux during 3rd nocturnal sleep period were compared using the Mann-Whitney U test. A P value of < 0.05 was considered statistically significant.
Ethics statement
Informed consent was obtained from all study participants after explanation of the nature and consequences of the study, and the study protocol was reviewed and approved by the Institutional Review Board of Korea University Anam Hospital (approval No. ED12261) and adhered to the tenets of the Declaration of Helsinki.
Go to :
RESULTS
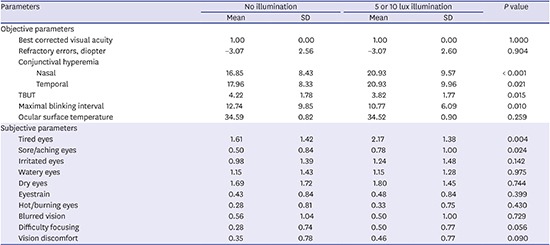
Six subjects failed to complete the 3-night protocol. Among these 6 subjects, 4 was allocated to receive 5 lux exposure and the other 2 to receive 10 lux exposure. Excluding those subjects, the data of 54 subjects were analyzed. Table 1 summarizes the post-sleep visual function and ocular fatigue without illumination and at 5 or 10 lux of illumination. The best-corrected visual acuity and refractive error did not change. Nasal and temporal conjunctival hyperemia increased significantly (P < 0.001; 0.021 respectively), and TBUT and maximal blinking interval decreased significantly (P = 0.015; 0.010, respectively). Among the subjective parameters, eye tiredness and soreness were increased significantly (P = 0.004; 0.024, respectively). Difficulty in focusing also increased with marginal significance (P = 0.056).
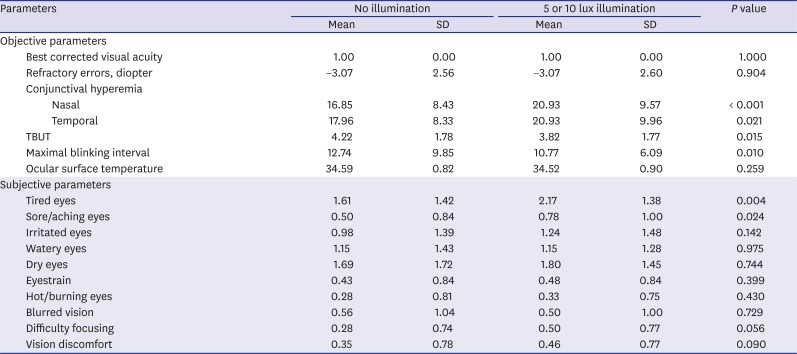
Table 1
The post-sleep visual function and ocular fatigue without illumination and at 5 or 10 lux of illumination
![]()
Visual function and ocular fatigue changes of subjects exposed to 5 lux illumination during the 3rd night are summarized in Table 2. Nasal conjunctival hyperemia increased significantly (P = 0.008). But no other subjective and objective parameters changed.
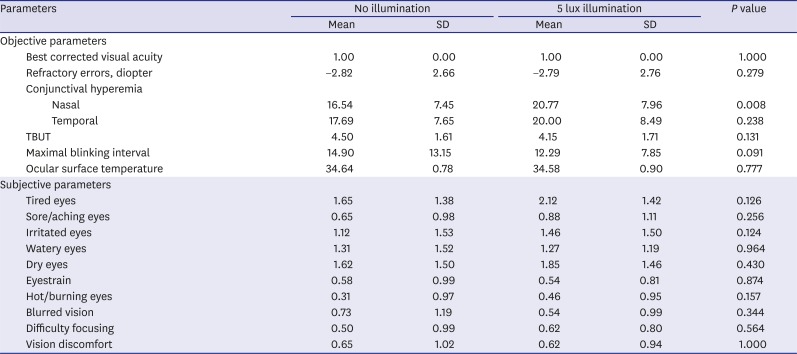
Table 2
Visual function and ocular fatigue of subjects exposed to 5 lux illumination during the 3rd night
![]()
Table 3 summarizes the visual function and ocular fatigue after sleep without light exposure and under 10 lux illumination. Both nasal and temporal conjunctival hyperemia increased significantly (P = 0.016; 0.041, respectively). TUBT decreased with marginal significance (P = 0.061). Based on the questionnaire, eye tiredness, soreness, difficulty in focusing and vision discomfort increased significantly (P < 0.05). The amounts of change in visual function and ocular fatigue after sleep under 5 and 10 lux exposure were compared in Table 4. There was no statistically significant difference between 5 and 10 lux illumination.
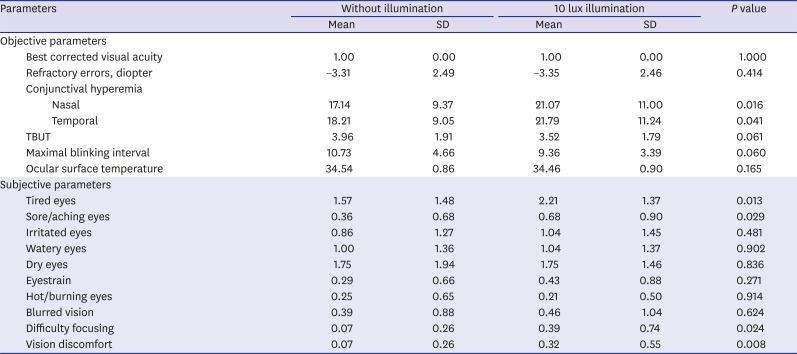
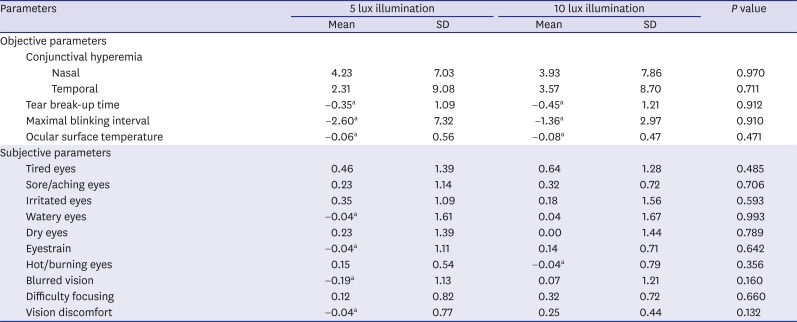
Table 3
Visual function and ocular fatigue of subjects exposed to 10 lux illumination during the 3rd night
![]()
Table 4
Comparison of the amount of changes in visual function and ocular fatigue between 5 and 10 lux light exposure at night
SD = standard deviation, TBUT = tear break-up time.
aDecrease after sleep under ambient light exposure.
![]()
Go to :
DISCUSSION
Light information during diurnal and nocturnal periods is transmitted to the suprachiasmatic nuclei (SCN) through the PRGC.13 The SCN is thought to contain the human circadian clock and control the daily pattern of most physiologic processes.1415 It regulates hormones including cortisol, serotonin, and melatonin, and it controls the sleep-wake cycle, which is essential for systemic health.16 When the eye is exposed to light nocturnally, melatonin secretion is suppressed by the SCN.1617 Melatonin is considered one of the most potent antioxidants, and it has known neuroprotective, anti-aging, immunomodulative, and oncostatic properties.3 For example, an elevated breast cancer prevalence in night shift-work nurses is linked to disrupted melatonin secretion.181920 Symptoms frequently reported by shift-workers such as insomnia, depression, cardiovascular disease, and premature mortality are also thought to be related to melatonin secretion disruption, which is caused by nocturnal light exposure.21
The human eye is also influenced by circadian rhythm. Numerous studies report diurnal variation in ocular structures and intraocular pressure. Intraocular pressure in a normal population is reported to vary 4–5 mm Hg diurnally, and the variation is greater in patients diagnosed with glaucoma.2223 Diurnal variation in choroidal thickness and axial length is also reported.2425 The circadian structural alterations are thought to control ocular growth, influence emmetropization, and affect refractive error development.2627 When the eye is exposed to nocturnal light, the diurnal ocular variation may be altered either by response to the light itself or indirectly through the disrupted circadian rhythm. In animal experiments, disruption of normal diurnal light rhythm changes refractive development in chickens.428 Quinn et al.5 noted that children exposed to nocturnal ambient light have a higher prevalence of myopia, which suggests that nocturnal light exposure during sleep may be a precipitating factor in myopia development. Reports contradict on the relationship between nocturnal light exposure and myopia development6 and are inconclusive because of the absence of prospective case-controlled studies, but a potential correlation between nocturnal ambient light and ocular growth cannot be excluded.
This study found that 5 lux or greater light exposure during sleep at night increased ocular fatigue. In most studies, ocular fatigue is evaluated only subjectively using a symptom questionnaire, and an objective measurement of ocular fatigue has not been established. In our previous study,12 we measured ocular fatigue after 1 hour of computer work both subjectively and objectively, which revealed that TBUT, maximal blinking interval, conjunctival hyperemia, and ocular surface temperature correlated with ocular fatigue. Therefore, we used identical objective and subjective methodology in this study.
The questionnaire revealed that eye tiredness, soreness, focusing difficulty and vision discomfort increased in the group with 10 lux light exposure at night. Conjunctival hyperemia also increased, and TBUT and maximal blinking interval decreased. In most previous studies, ocular fatigue was evaluated after visual tasks,293031 and, these studies revealed that the blinking rate decreased, the ocular surface was more exposed to air during visual tasks, and the resulting dry eye caused ocular fatigue symptoms.29323334 However, the subjects in our study did not perform any visual tasks; instead, the eyes were closed during sleep. Thus, an explanation other than decreased blinking rate is necessary. There are several potential mechanisms of ocular fatigue induced by nocturnal ambient light. Light may partially enter the eyes through the eyelid, which would induce the light reflex, prolong pupillary constriction, and cause ocular fatigue. In addition, disruption of the circadian rhythm may be a factor in resulting ocular fatigue. The nocturnal light exposure may disrupt the circadian clock and disturb the diurnal variation of ocular structures including choroidal blood flow, resulting in ocular fatigue. Alternatively, the ambient light may deteriorate sleep quality and cause shallow sleep.3536 This sleep disturbance can induce systemic fatigue37 and subsequently ocular fatigue. Sleep disturbance has been also documented to induce dry eye syndrome. Lee et al.38 reported that sleep deprivation reduced tear secretion, impaired tear film and decreased TBUT. They hypothesized that the alteration in autonomic nervous tone and imbalance of hormone levels induced by sleep deprivation affected tear secretion and tear film stability. Decreased TBUT after nocturnal ambient light exposure in our study could be explained in this aspect. We cannot determine the mechanism of ocular fatigue in the current study, but we surmise that these mechanisms may induce ocular fatigue in varying degrees. Further research of the mechanisms is necessary.
There are several limitations in this study. The number of subjects was small. Although ocular fatigue was induced after light exposure despite the small number of subjects, we think that future study using a larger sample size would reveal additional and more reliable differences associated with nocturnal ambient light. In addition, daytime activity of the subjects was not controlled. We instructed subjects to avoid activities that may influence ocular fatigue or sleep quality, including vigorous exercise, napping, excessive caffeine intake, and alcohol consumption, and the subjects reporting these activities were excluded. However, daytime activity could not be monitored; therefore, we cannot assume that those activities were perfectly controlled. Further study that systematically controls daytime activity on a larger number of subjects is necessary.
In conclusion, nocturnal light exposure increases ocular fatigue. Ambient light during nocturnal sleep should be prevented to avoid ocular fatigue.
Go to :
 XML Download
XML Download