

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Rheumatoid arthritis (RA) is characterized by persistent synovitis, systemic inflammation and autoantibodies (rheumatoid factor [RF] and anti-cyclic citrullinated peptide antibody [anti-CCP Ab]). RA affects 0.5%–1% of adults in developed countries and is three times more frequent in women than men.1 It is characterized by inflammation of multiple joints and often progressively leads to joint destruction and disability. Indeed, most patients also suffer from chronic inflammation. Although arthritis is the major manifestation of RA, RA is often associated with extra-articular manifestation as well.2 Extra-articular manifestation is observed in 17.8%–40.9% of RA patients and is related to disease duration and treatment as well as comorbidities.34 Although neurological manifestations, which are extra-articular, are considered to be less common among patients with RA, recent studies have reported the prevalence of such impairment to account for up to 50% of patients with RA.56
Disturbed sleep is a major concern among patients with RA and may negatively affect quality of life as well as increase morbidity and mortality.7 Because disturbed sleep is a common symptom of RA, sleep is an important consideration in health-related quality of life (HRQoL) in patients with RA.8 Previous studies have suggested that disturbed sleep may be influenced by pain or fatigue.8910
Recent studies suggest that RA-related sleep disturbances correlate with cognitive impairment and cognitive dysfunction, and, collectively, these symptoms reduce the ability to perform activities of daily living and quality of life. Cognitive impairment may also be associated with clinical features including chronic pain and fatigue11 as well as with neurologic comorbidities including depression, disturbed sleep, and anxiety.1213
The aim of this study was to assess the characteristics of sleep quality, HRQoL, and cognitive function in Korean female patients with RA and to investigate the association between poor sleep quality and HRQoL. In addition, we examined whether sleep quality and disease activity were associated with cognitive function as measured by the Korean-Montreal Cognitive Assessment (MoCA-K).
METHODS
Study population
One hundred and twenty-three patients with RA were recruited from a rheumatology clinic in the Seoul St. Mary's Hospital, a tertiary care university hospital, between July 2016 and May 2017. Inclusion criteria of this study were as follows: 1) women aged 18 years old or older; 2) satisfied the 2010 American College of Rheumatology/European League against Rheumatism criteria for RA14; 3) currently treated with disease-modifying anti-rheumatic drugs (DMARDs) or biologics.
Patients that might not complete all questionnaires due to physical or mental problems were excluded. We recruited only female patients because RA is more common in women and we wanted to rule out the influences of gender differences. Seventy-six females were also recruited from a rheumatology clinic as a control group. Patients in the control group included mainly those who treated with osteoporosis or osteoarthritis without any history of autoimmune such as RA, systemic lupus erythematosus, ankylosing spondylitis.
Sample size
The desired sample size was calculated by G*Power software (version 3.1.9.2; University of Düsseldorf, Düsseldorf, Germany).15 We have based estimated the sample size to detect a minimum effect size of 0.2. Based on our study design, containing 14 observed variables and three variables from the questionnaires data, with a significance level of 5% and power of 80%, the sample size was calculated as 114 patients. By adding sample loss of 10%, subjects were raised to 125 patients. However, 2 people excluded due to failed to complete questionnaires by physical distress, 123 patients included finally.
Baseline characteristics and laboratory findings
Age, height, and weight were recorded for all participants, and body mass index (BMI) was calculated in kg/m2. Demographic information was recorded including income, marital status, education, alcohol consumption, and smoking. It was recorded whether subjects were previously diagnosed with depression or not. In the patients group, disease duration and the type of RA medication being used (e.g., biologics, DMARDs, nonsteroidal anti-inflammatory drugs [NSAIDs], steroid dose) were also recorded. The disease activity was measured using the disease activity score in 28 joints (DAS28) for 3 variables, which included the 28-joint tender joint count, swollen joint count, and Westergren erythrocyte sedimentation rate (ESR). Additionally, C-reactive protein (CRP), RF, and anti-CCP Ab results were obtained retrospectively.
Questionnaire for sleep quality
The patients completed the Korean version of Pittsburgh Sleep Quality Index (PSQI).16 The scale had 19 items and measured 7 components of sleep quality: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. The PSQI is a self-reported questionnaire to distinguish a “good sleeper” (PSQI global score ≤ 5) from a “poor sleeper” (PSQI > 5).
Questionnaire for HRQoL
All subjects answered a 36-item Short-Form Health Survey (SF-36) for assessing HRQoL. The SF-36 has been translated into Korean and the Korean version was validated.17 The SF-36 has 8 individual subscales divided across physical and psychological HRQoL domains: physical functioning (PF), role-physical (RP), bodily pain (BP), and general health (GH), vitality (V), social functioning (SF), role-emotional (RE), and mental health (MH). Scores on these domains can be grouped into 2 component summaries: the physical component summary (PCS) and the mental component summary (MCS). It was developed at RAND as part of the medical outcomes study.
Questionnaire for cognitive impairment
Cognitive function was measured using the MoCA-K.18 The Mini-Mental State Examination is most widely used for screening cognitive impairment; however, it is most appropriate to detect moderate and severe cognitive dysfunction rather than mild cognitive impairment. The MoCA-K was performed to screen patients with mild cognitive impairment. These items include short-term memory recall, visuospatial ability, executive function, attention-concentration-working memory, language, and orientation to time and place. Higher scores indicate better cognition and a score below 23 indicates cognitive impairment.
Statistical analysis
Continuous variables are expressed as the median (interquartile range [IQR]) as a normal distribution was not observed in most variables. Categorical variables are shown as absolute numbers with a percentage. The Mann-Whitney U test was used to compare continuous variables, and the χ2 or Fisher's exact test was used for categorical variables to compare RA patients with healthy controls, as well as between the groups of RA patients according to sleep quality, disease activity, and cognitive function. Spearman's correlation coefficient was used to examine the relationships between quality of sleep (PSQI), HRQoL (SF-36 score), disease activity (DAS28), and cognitive dysfunction (MoCA-K). Multivariate linear regression analysis was used to determine the effect of sleep quality on HRQoL or cognitive function with adjustment of the confounding factors. When P values were less than 0.05, results were considered statistically significant. All statistical analyses were performed using SPSS version 24.0 (IBM Co., Armonk, NY, USA).
RESULTS
Demographics and clinical characteristics of subjects
One hundred and twenty-three RA patients and 76 control subjects were included, and all participants were women. Baseline demographic and clinical characteristics are presented in Table 1. The median age was 56 years (IQR 47–61) and the median disease duration was 113 months (68–199). The median age of the control group was 54 years (45–61). RF was observed in 103 patients (83.7%) and anti-CCP Ab was observed in 97 patients (78.9%). The mean DAS28 was 2.69 and 26 patients (21.1%) showed a score greater than 3.2. In total, 117 patients (95.1%) were on DMARDs with 45 (36.6%) on at least two DMARDs.
Table 1
Baseline characteristics of study subjects

Values are presented as median (interquartile range) or number (%).
RA = rheumatoid arthritis, BMI = body mass index, RF = rheumatoid factor, anti-CCP Ab = anti-cyclic citrullinated peptide antibody, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, DAS28 = disease activity score in 28 joints, NSAIDs = nonsteroidal anti-inflammatory drugs, DMARDs = disease-modifying anti-rheumatic drugs.
aDMARDs: disease modifying antirheumatic drugs including methotrexate, hydroxychloroquine, sulfasalazine, leflunomide, tacrolimus; bBiologics: adalimumab, etanercept, infliximab, tocilizumab.
The RA patients had statistically higher PSQI scores with the exception of habitual sleep efficiency (P < 0.001) and lower scores in SF-36 (P < 0.05) (Table 2). This means that there was significantly poorer HRQoL in regard to PCS and MCS scores in RA patients (44.61 vs. 50.54, P < 0.001; 49.14 vs. 53.23, P = 0.011). There was also lower cognitive function in RA patients compared to the control group (26 vs. 27, P = 0.013).
Table 2
Comparison of questionnaire results of the study subjects
Values are presented as mediation (interquartile range).
PSQI = Pittsburgh Sleep Quality Index, MoCA-K = Korean-Montreal Cognitive Assessment, SF-36 = 36-item Short-Form Health Survey, PF = physical functioning, RP = role-physical, BP = bodily pain, GH = general health, PCS = physical component summary, V = vitality, SF = social functioning, MH = mental health, RE = role-emotional, MCS = mental component summary.
Differences in clinical variables and results of the questionnaire between RA patients with and without poor sleep quality
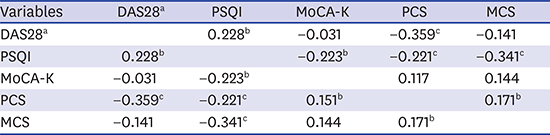
There were significant correlations between PSQI and PCS (r = −0.221; P < 0.003), PSQI and MCS (r = −0.341; P < 0.001), and HRQoL and MoCA-K (r = −0.223; P = 0.003) (Table 3). For RA patients, sleep quality was significantly correlated with disease activity (r = 0.228; P = 0.011). Therefore, we performed subgroup analysis according to sleep quality. Baseline demographic and clinical characteristics of RA patients with and without poor sleep quality are presented in Table 4. The patients with poor sleep quality showed higher BMI (21.09 vs. 22.19; P = 0.008) and a lower PCS on the SF-36 (46.95 vs. 42.74; P = 0.021). However, despite the correlation, disease activity and cognitive function did not exhibit significant differences between “good sleepers” and “poor sleepers.”
Table 3
Correlation coefficients of various variables

Table 4
Comparison of demographic and characteristics of RA patients subgroup according to sleep quality

Values are presented as mediation (interquartile range) or number (%).
PSQI = Pittsburgh Sleep Quality Index, BMI = body mass index, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, DAS28 = disease activity score in 28 joints, RF = rheumatoid factor, anti-CCP Ab = anti-cyclic citrullinated peptide antibody, MoCA-K = Korean-Montreal Cognitive Assessment, SF-36 = 36-item Short-Form Health Survey, PCS = physical component summary, MCS = mental component summary, DMARDs = disease-modifying anti-rheumatic drugs.
Sleep quality independently affects HRQoL and cognitive function
Multivariate linear regression was performed to determine whether sleep quality independently affects PCS, MCS, and cognitive function. PCS was affected by disease duration, disease activity, and sleep quality, and poor sleep quality was an independent risk factor for low PCS (Table 5). For MCS, only PSQI remained significant after adjustment for confounding factors. Cognitive function was mostly affected by age, but poor sleep quality was also a significant factor.
Table 5
General linear model testing relationship between sleep quality and health-related quality of life and cognitive function in RA patients
Values are presented as mediation (interquartile range). Age, BMI, disease duration, DAS28, PSQI were entered into the multivariate model.
RA = rheumatoid arthritis, SE = standard error, PCS = physical component summary, BMI = body mass index, DAS28 = disease activity score in 28 joints, PSQI = Pittsburgh Sleep Quality Index, MCS = mental component summary, MoCA-K = Korean-Montreal Cognitive Assessment.
DISCUSSION
In this study, we observed an increased prevalence of poor sleep quality in patients with RA compared with healthy controls. It was also shown that the frequency of poor sleep quality was higher in RA patients than in a healthy population in a previous study.19 The prevalence of poor sleep quality presented in this study is similar with previous studies that show that 50%–70% of patients with RA have poor sleep quality.20 In Korea, Son et al.21 showed that there is a higher incidence of poor quality of sleep in patients with RA than in the healthy population. High RA disease activity was also associated with poor sleep quality in a Korean population. Recently, Kim et al.22 revealed individuals with RA have a higher risk for sleep disturbances compared with individuals without RA.
In this study, there was no difference between patients with good vs. poor sleep quality in regard to age, disease duration, disease activity, serologic profile, and RA medication, whereas BMI was higher in “poor sleepers.” Peltzer et al.23 assessed an association between BMI and sleep quality, and they found a significant association between short sleep duration and increased BMI among women.
The present study showed a correlation between disease activity and quality of sleep as well as disease activity and the physical component of the SF-36. Also, there was a negative correlation between quality of sleep and cognitive function, meaning that the worse the sleep quality, the lower the cognitive function.
The PCS of the HRQoL showed an association with sleep quality. The physical components consisted of physical functioning, role-physical, bodily pain, and general health, and therefore sleep quality may be affected by physical pain or function. Another study showed that pain contributed to sleep disturbance24 and poor sleep could contribute to a lower pain threshold in patients with RA.9
The present study showed lower HRQoL in patients with RA than the healthy control group. Another study also showed that RA negatively impacts HRQoL, especially physical health, and that RA affects the mental health domain of HRQoL to a lesser degree.25 Our study also presents lower physical health than mental health, suggesting that RA has a greater impact on the physical health component of HRQoL than the mental health component. In the recommendations for treating patients with RA, the goal is to maximize long-term HRQoL through control of symptoms, prevention of structural damage, normalization of function, and social participation.26 Sanderson et al.27 also have described the importance of HRQoL and showed that HRQoL was one of the top priority outcomes to measure the efficacy of the treatment in RA patient perspective. Comparing two groups according to sleep quality (“good sleepers” vs. “poor sleepers”) in patients with RA, physical health was significantly better in “good sleepers” than “poor sleeper.” These findings suggest that sleep quality affects HRQoL in patients with RA, especially physical health.
Several methods are used for evaluating HRQoL in patients with RA. For example, Linde et al.28 showed that SF-36 is a reliable and valid tool for measuring HRQoL in RA. Although the Health Assessment Questionnaire and the RA quality of life scale also have reliability and validity, the SF-36 is available for healthy populations and other disease groups, providing a comparison of HRQoL to a healthy population.
Cognitive impairment was assessed with the MoCA-K, which was not validated for patients with RA. However, there is not yet a validated method for measuring cognitive function in patients with RA. A previous study analyzed characteristics of cognitive impairment with a meta-analysis and did not show consistent results across studies.29 With that said, RA seems to be influenced by age, education, and disease activity, but no significant differences were revealed between the RA and control groups. Recent study showed discrepancy between subjective and objective measures of cognitive impairment and sleep quality were significantly associated with subjective method in Korean RA patients.30 Our study only performed an objective cognitive function assessment, which may differ from subjective cognitive function. Further research should be conducted to identify the association between subjective cognitive impairment with sleep quality and HRQoL.
There are several limitations to our study. First, the sample size was not large and most patients had less severe disease activity. Second, MoCA-K is not a validated tool for the assessment of cognitive impairment for patients with RA. Third, sleep quality was not evaluated according to objective changes. Although polysomnography is recommended as the gold standard for primary sleep disorder evaluation, it is difficult to perform in an outpatient setting due to price and manpower problems. Despite these limitations, however, we believe that our study has important implications. This was the first study to evaluate the correlation between sleep quality and cognitive impairment in Korean female patients with RA. Further studies on the effects of disease activity, medication, and chronic diseases on cognitive function are needed to better describe the details of these relationships.
In conclusion, poor sleep quality was associated with high disease activity, low HRQoL, and lower cognitive dysfunction in patients with RA. Although causal relationships cannot be determined from correlation studies, our data suggest that good control of disease activity in patients with RA may be able to improve sleep quality and, thus, HRQoL and cognitive function. Therefore, physicians should consider disease activity, quality of sleep, and quality of life when treating patients with RA. Also, further studies are needed to understand the correlation between cognitive function and other factors.
 XML Download
XML Download