

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
Dupuytren's disease (DD) is a type of fibroproliferative disease which usually occurs in the palmar aspect of the hand and can lead to flexion contracture of fingers in severe cases. DD has a broad spectrum of symptoms from tiny nodules in the palm of the hand to flexion contracture of fingers for which hand surgeons can perform collagenase injection or fasciectomy according to the disease severity.12 Although its exact cause is unknown, researchers suspect that a genetic problem is related to DD because of its heredity and racial predominance.3
The racial predominance is supported by a higher prevalence of DD in Caucasians in northern Europe than in other races.4 However, the epidemiology of DD in Asia has been reported only in Japan in the past decades,56 and recently in Taiwan.7 Because of this relatively small number of Asian studies, the prevalence of DD in Caucasians appears more prominent.
In this regard, we conducted an epidemiological study of DD in Korea using the large dataset provided by the Health Insurance Review and Assessment Service (HIRA). Furthermore, diseases associated with DD and the therapeutic trends in DD were investigated.
METHODS
Dataset
Korea has been implementing a health insurance system for all citizens since 1989. Since the medical data of the whole population in Korea are managed at the HIRA, the HIRA's dataset makes it easy to retrieve and analyze data to understand the medical status of the whole country. HIRA provides some of the national data to support public policy formulation and research activities. The dataset used in our research was part of the HIRA dataset. The raw data provided by HIRA are captured in the form of specifications that occur when a medical institution makes a claim to the National Health Insurance Service (NHIS) after patients have been treated. We performed this study based on this set of raw data. We extracted the information using the Korea Informative Classification of Disease 7th revision (KOCID-7) code of M72.0 for DD for the survey period 2007 to 2014. According to the KOCID-7, M72.0 represents palmar fascial fibromatosis (Dupuytrens).
Epidemiological profiles
The annual prevalence was defined as the proportion of the population with DD in the year and includes people who already have DD at the beginning of the year as well as those who acquired it during the year. The annual prevalence was determined from the number of patients who had the M72.0 code and visited medical facilities more than once during the year. The annual incidence was determined by the number of patients who had been assigned the M72.0 code for the first time in that year and visited medical facilities more than once during the year. The data on the population of Korea, such as total population in the year, and population by age and sex group, which were required to estimate the prevalence and incidence, were provided by the Korean Statistical Information Service, a website-based service operated by Statistics Korea. We also analyzed the distribution of DD patients by age group and the difference in the prevalence/incidence according to sex. In addition, other diseases that accompanied DD were investigated. Annual frequencies of surgery for DD were determined to identify the treatment trend for DD. Since the surgical treatment codes for DD have not been unified as of yet, we investigated using all applicable surgical codes for DD (Table 1).

Statistical analysis
When comparing the prevalence of diseases such as DD between countries for a particular age group, the age composition of each country should be considered because the prevalence of DD may be relatively high in countries with a high proportion of middle-aged people. Therefore, age adjustment is needed to compare epidemiological profiles between countries. We adjusted the values using the direct method in this study. The total population of the Organization for Economic Co-operation and Development (OECD) countries in 2014 was assumed to be the standard population for the direct method. Poisson regression analysis was used to analyze the trends in annual incidence of DD, the number of annual surgeries for DD, and sex differences. P < 0.05 was interpreted as statistically significant.
RESULTS
Prevalence and incidence of DD
A total of 16,630 patients with DD were found in the HIRA dataset from 2007 to 2014. The mean prevalence (values in parentheses indicate the adjusted value) during the study period was 32.2 (35.2)/100,000 population, 41.8 (47.9)/100,000 for men and 22.5 (23.5)/100,000 for women. The number of male patients was about 1.85 (2.04) times the number of female patients (Fig. 1). The mean annual incidence was 1.09 (1.11)/100,000 population/year, which was 1.80 (1.89)/100,000/year for men and 0.38 (0.37)/100,000/year for women. The ratio of men to women was 4.67 (5.11):1 (Fig. 2). The mean age of patients with DD at the beginning of the study period was 53.2 years (54.0 years for men, 49.5 years for women). The sex-specific prevalence rate determined by Poisson regression analysis showed that female patients had a prevalence that was 0.539 times (95% confidence interval [CI], 0.533–0.545; P < 0.001) lower than that for male patients. Poisson regression analysis also showed that the change in annual prevalence was not statistically significant (P = 0.733). The incidence of DD calculated using the Poisson regression analysis was 0.214 times (95% CI, 0.197–0.233; P < 0.001) lower in female patients than that in male patients. The annual incidence decreased by 0.96 times (95% CI, 0.945–0.976; P < 0.001) per year (Table 2).


Table 2
Poisson regression analysis for epidemiologic profiles of Dupuytren's disease

Disease associated DD
Diseases associated with DD included hypertension in 5,076 (30.5%) patients, diabetes mellitus in 4,437 (26.7%) patients, hyperlipidemia in 3,396 (20.4%) patients, ischemic heart disease in 1,309 (7.9%) patients, cerebrovascular disease in 769 (4.6%) patients, and obstructive lung disease in 438 (2.6%) patients (Fig. 3).

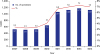
Surgery of DD
The prescribed codes for surgery for DD were N014, N023, N092 and N083. The mean number of surgeries performed for DD per year was 840.3 cases (range, 511–1,178), which was 5.24% (range, 3.24–7.30) of all DD patients. Poisson regression analysis showed a statistically significant increase of 1.147 times (95% CI, 1.134–1.159; P < 0.001) per year (Fig. 4 and Table 2).
DISCUSSION
According to studies of DD epidemiology in Europe, the prevalence of DD in Norway was 5,100 per 100,000 to 46,000 per 100,000,89 and in the Reykjavik region of Iceland it was reported to be 13,000 per 100,000.10 The prevalence of DD was reported to be 22,000 per 100,000 in the Netherlands11 and 31,000 per 100,000 in Bosnia and Herzegovina in southern Europe.12 In the United States, Saboeiro et al.13 reported on the prevalence of DD by race in a study of veteran patients. According to the report, the prevalence of DD in white patients was 734 per 100,000 population, 237 per 100,000 in Hispanic whites, 144 per 100,000 in Native Americans, 130 per 100,000 in blacks and 67 per 100,000 in Asians. The difference between the United States and Europe was believed to be due to patient heterogeneity and various research methods. In Asia, Egawa and colleagues5 reported that the prevalence of DD in Japan was 19%, and recently Taiwan researchers reported a prevalence of 4.52 per 100,000 population.7 McFarlane14 pointed out that the unusually high prevalence of DD in Japan reported by Egawa et al.5 might be related to their accurate diagnosis of minimal disease. Their patients were actually elderly residents of nursing homes and few had enough contracture to warrant surgery. In this study, the prevalence of DD in Korea was 32.3 per 100,000 population, which was much higher than that of Taiwan; however, it was significantly lower than that of Europe by 1/1,000–1/100. Among the previous studies, the prevalence was most similar to the prevalence of Asian-American veterans.13
Previous studies have reported 1.4 to 7.9-fold greater prevalence of DD in men than in women.81012151617 In this study, the prevalence of DD in men was 1.85 times higher than that in women, and the incidence was 4.67 times higher in men than in women. The reason the difference in prevalence is less than the difference in incidence is thought to be as follows. First, women have a longer life span than men. Second, women's average age of onset of DD is about five years earlier than that of men. For these reasons, the duration of DD in women is presumed to be longer than that in men. The most common comorbid disease was hypertension (30.5% of DD patients); however, it was similar to the prevalence of hypertension in adult Koreans (32%). The second most common disease, diabetes, was associated with 26.7% of DD patients which was more than twice the prevalence of diabetes (10.6%) in the general Korean population.18 In fact, diabetes has been reported as an important risk factor for DD in many previous studies.17192021 Hyperlipidemia was associated with 20.4% of DD patients and was similar to that of the general Korean population (19.5%).18
Korea and Taiwan were the only countries where epidemiological studies were conducted for the whole population. This nationwide study was possible because of the social insurance scheme under which all citizens are insured. Since information on all domestic medical services is processed by a single organization called the HIRA, systematic and uniform data collection is possible. The large volume of data generated by the HIRA can be utilized by researchers through appropriate procedures. The Taiwan's data called National Health Insurance Research Database (NHIRD) is generated in a similar way to Korean HIRA database and therefore contains similar information such as patient identification number, sex, date of birth, dates of admission and discharge, diagnosis and procedure codes, details of prescription, and so on. If there is a difference, data from Taiwan is obtained from 2001 to 2011, but data from Korea is from 2007 to 2014. On the other hand, the previous studies related to the epidemiology of DD were mostly based on epidemiological surveys by sampling on specific aspects such as regions, age, and sex.8101215 Such studies are available in western countries where DD is relatively common, and are difficult to apply in areas where prevalence is very low, such as in Asia. This is because the rarity of the disease makes it difficult to extrapolate the prevalence in small areas of the country. In addition, the prevalence of diseases such as DD, which has a strong relationship with age and sex, can be significantly affected by the composition of the population in that area. Therefore, adequate statistical standardization of the population is necessary to compare regional epidemiological surveys with other countries or ethnic groups. This study also sought to improve statistical confidence by standardizing the population composition of Korea to the population of OECD member countries.
A large data-based study such as this is more accurate than a study based on patient's subjective diagnosis, such as that obtained via questionnaires, because it follows the physician's judgement and decision at all medical institutions when entering the disease code.22 However, individual diagnoses by physicians may be less uniform because the spectrum of symptoms of DD varies from palpable nodule to flexion contracture. In fact, if there is a physician diagnosing DD on the basis of the flexion contracture that occurs only in less than 1/5 of the DD cases, the prevalence may be underestimated.11 In addition, patients with mild DD who have not visited a medical facility because they have only a palpable mass without any other uncomfortable symptoms may be excluded from counting of prevalent cases. Therefore, the overall prevalent population of DD cases may tend to be underestimated in the large data-based study.23 Another limitation of this study is the lack of information about surgical treatment of DD. Fasciectomy, which is commonly used to treat DD, was not coded in the insurance billing system, thus physicians used a variety of different codes instead.2 Therefore, it was difficult to accurately investigate the surgeries performed on DD patients.
In conclusion, the prevalence and incidence of DD in Korea were significantly lower than those in western countries and higher than that in Taiwan. There was no statistically significant change in the annual prevalence for seven years and the incidence decreased slightly over the study period. The increase in the number of surgeries for DD per year was statistically significant. Hypertension, diabetes and hyperlipidemia were the most common comorbid diseases. Diabetes in DD patients was twice as common as in the general population of Korea.
 XML Download
XML Download