

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Sudden unexplained infant deaths (SUIDs) are defined as the death of an infant less than 1-year-old in which investigation, autopsy, medical history review, and appropriate laboratory testing fail to identify a specific cause of death, which includes cases that meet the definition of sudden infant death syndrome (SIDS).1 We previously reviewed 355 cases of SIDS in Korea, focusing on the sleep environment.2 Subsequently, the campaign for safe sleep environments including “back to sleep” was widely launched but more than 100 infants still die suddenly and unexplainably before the age of 1 year in Korea.
Long QT syndrome (LQTS) is a group of inheritable primary electric diseases of the heart. The disease cluster was first noted in a family where several children with congenital hearing loss exhibited QT prolongation in electrocardiography (ECG) examinations, and experienced recurrent syncope and sudden cardiac death, with an autosomal recessive inheritance (Jervelle and Lange-Nielsen [JLN] syndrome).3 LQTS is now understood to be a cardiac channelopathy involving ventricular repolarization delay due to a prolonged duration of the myocardial action potential. Postmortem genetic testing or molecular autopsy has revealed a strong association between LQTS variation and SIDS.45 It has been reported that 5.2%–14.0% of SIDS cases may be linked to LQTS,67 which affects the cardiac conduction system. Therefore, postmortem genetic testing has recently been recommended as a routine procedure in the autopsy of SIDS cases.68 Unfortunately, the molecular diagnosis of postmortem examinations is not yet a routine practice in Korea. In this study, we retrospectively reviewed 200 SIDS cases from a genetic viewpoint to determine the number of cases in Korea that may have been associated with LQTS variation and accumulate information to support the value of the availability of postmortem genetic testing for SIDS in Korea.
Go to : 
METHODS
We designed a retrospective study to test for the presence of genetic risk factors involving LQTS in SIDS in Korea. The cases analyzed were retrieved from a nationwide pool of infant deaths recorded between January 2005 and December 2013. After a thorough review of the police investigative and autopsy reports as well as a histological re-examination, 200 cases of SIDS IA and IB were selected according to Krous et al.9 The SIDS IA group was defined based on the following characteristics: cases aged 21 to 270 days at the time of death with a normal clinical history, term delivery, normal growth and development, no familial history of sudden unexplained deaths, and no suspicious scenes. A comprehensive postmortem investigation including toxicological, microbiological, vitreous chemistry, or metabolic screening studies with death scene investigation by police authorities was conducted. Category IB consisted of infant deaths that met the general definition as well as all the criteria for category IA except for this investigation. Infants of the SIDS category II, which includes deaths outside the SIDS I age range (21 days to 9 months) and cases where accidental asphyxia, were excluded in this study.9 The obtained data included the position in which the deceased was found.
The genomic DNA from 200 SIDS patients was extracted from the organ (the heart or liver) tissue paraffin-embedded blocks using the QIAamp DNA FFPE tissue kit (QIAGEN, Hilden, Germany). Owing to expected low DNA yields from the paraffin-embedded tissue samples from each patient, all DNA quantities were determined using a NANODROP™ LITE spectrophotometer (Thermo Fisher Scientific Inc., Waltham, MA, USA). Table 1 shows the 85 DNA variants from 6 genes (KCNQ1, SCN5A, KCNE1, KCNE2, KCNJ2, and CAV3), ascertained from the literature using PubMed (www.ncbi.nlm.nih.gov) based on their reported involvement in SIDS,1011121314151617181920 which were investigated using a real-time polymerase chain reaction (PCR) single nucleotide polymorphism (SNP) assay.
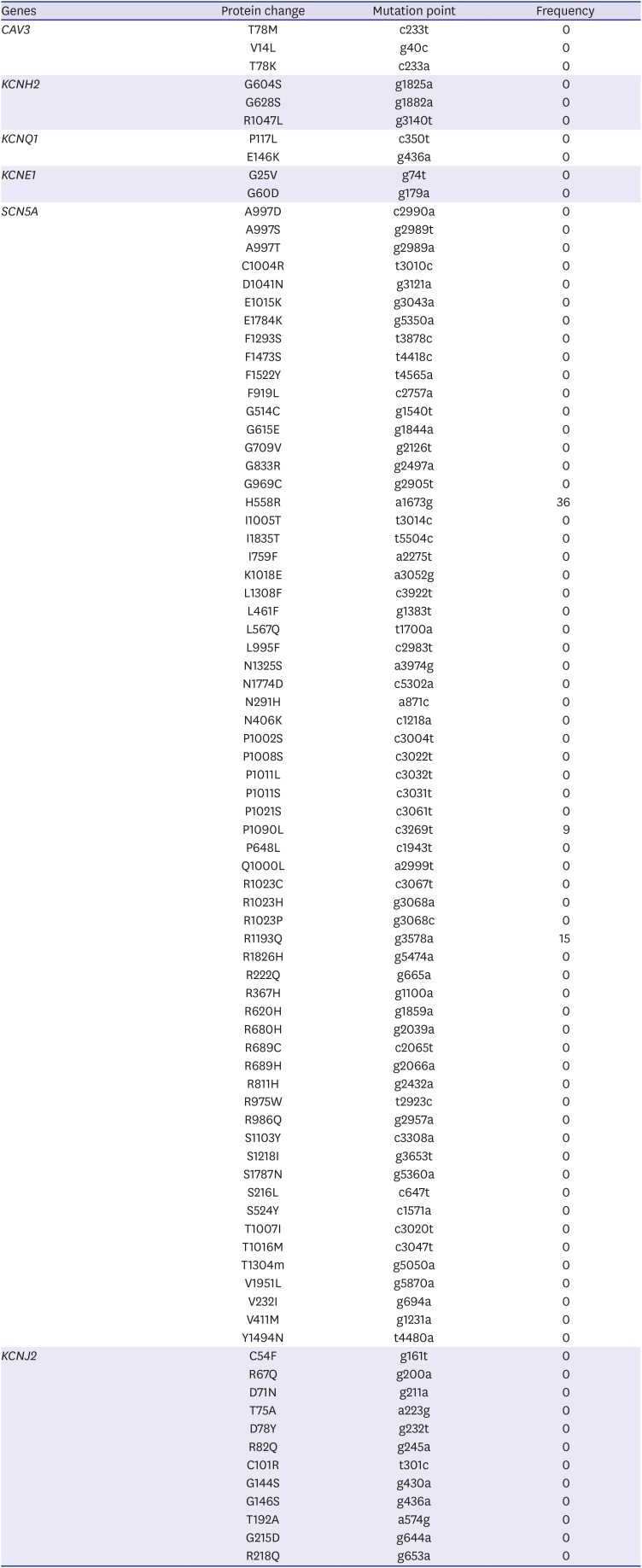
Table 1
LQT-related genes investigated in this study
![]()
The SNP genotyping with real-time PCR used a pair of primers and a specific dye-labeled probe for each allele: allele 1 (normal) was labeled with FAM, and the other allele 2 (mutation) was labeled with HEX. During amplification, the generation of FAM, HEX, or both types of fluorescence indicate an allele 1 homozygote, allele 2 homozygote, and a heterozygote, respectively. The quencher dye at the 3ʹ end of each probe was BHQ®-1 (black hole quencher® 1). Some primers and probes were designed firsthand whereas others were purchased from Applied Biosystems (AB) Taqman SNP assays mto human SM (Life Technologies, Carlsbad, CA, USA).
Real-time PCR was performed with 20 ng gDNA using the iQ probe SuperMix and CFX Connect™ real-time PCR (Bio-Rad, Hercules, MA, USA) according to the manufacturer's protocol. The PCR conditions were as follows: an initial incubation at 95°C for 5 minutes, followed by 50 cycles of denaturation at 95°C for 15 seconds and annealing and extension at 60°C–68°C (temperatures depended on primers) for 30 seconds. Multiplex genotyping strategies were used to confirm the results with TaqMan. The PCR for sequence analysis was performed using the Prime STAR™ HS (premix, TAKARA, Shiga, Japan) according to the manufacturer's protocol.
Ethics statement
The study was confirmed as a research activity qualifies as non-human participant by the Institutional Review Board of Seoul National University Hospital (No. 2018-001). All data were analyzed anonymously. The requirement for informed consent was waived by the board.
Go to :
RESULTS
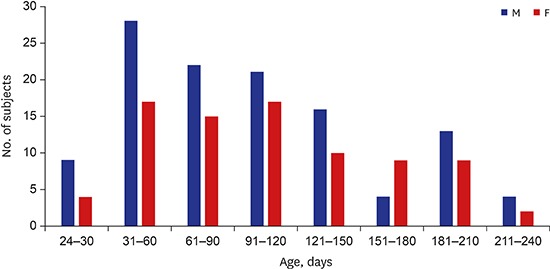
The results showed that 58% of the 200 SIDS cases were male infants (116 male and 84 female infants, respectively). In addition, the mean age was 140 days (median, 107 days; range, 24 to 270 days) and all the infants were of Asian ethnicity (Fig. 1). SIDS IA category criteria were fulfilled in 45 cases (22.5%) whereas the rest were determined to be SIDS IB (Table 2). All infants died in their sleep.
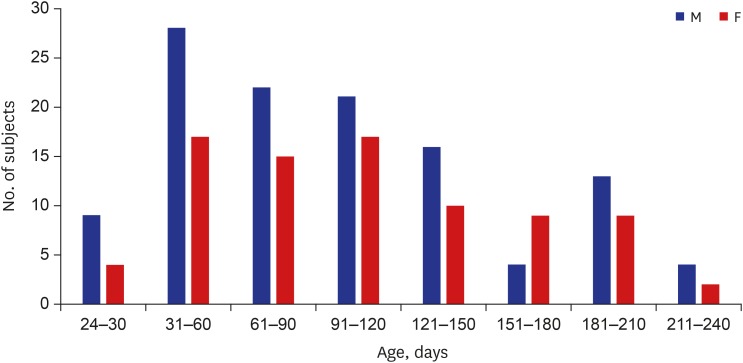 | Fig. 1Age and sex distribution of SIDS subjects.SIDS = sudden infant death syndrome, M = male, F = female.
|
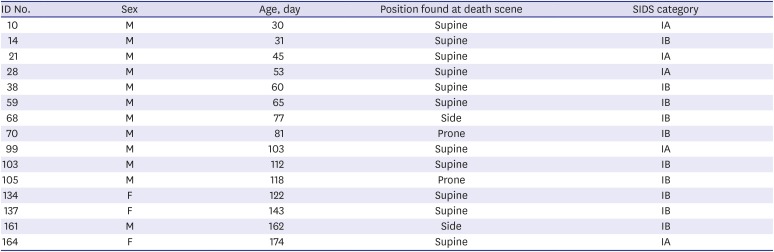
Table 2
Demographics, history, investigations, cardiac testing in 15 cases, which showed a genetic variant (R1193Q in SCN5A)
![]()
Table 1 shows the variants of LQTS-related genes detected in SIDS in this study. A previously reported SNP,122122 H558R in exon 12 and P1090L in exon 18 of the SCN5A gene was found in 36 and 9 (18.0% and 4.5%) SIDS cases, respectively. No variants indicating possible pathogenicity were found in this study.
Fifteen cases (7.5%) had R1193Q in SCN5A (Table 1), which has been reported in association with LQTS and Brugada syndrome (BS),2223 but a recent study showed it to be a common polymorphism in Asians.12 The prevalence of the R1193Q mutation showed no statistical significance in relation to sex, SIDS category, and position of the infant at the death scene.
Go to :
DISCUSSION
Although a molecular autopsy is not included as a standard protocol in SIDS cases, postmortem genetic testing is increasingly being recommended, especially focusing on arrhythmia syndrome.2425 Tester and Ackerman26 estimated that approximately 10% of all SIDS cases were actually caused by cardiac channelopathies resulting in LQTS. A previous large population-based study also reported that pathogenic variants associated with KCNH2 and SCN5A were found in 9.5% of subjects.18
From the start of this study, we cautiously selected category IA and IB SIDS cases and excluded those in category II to exclude the mechanical asphyxia and assess the precise relationship between SIDS and LQTS. We hypothesized that approximately 5%–10% of the pathogenic variants would be identified in this SIDS cohort. However, pathogenic variants associated with KCNQ1, SCN5A, KCNE1, KCNE2, KCNJ2, and CAV3 were not observed. In particular, detection of the R1193Q mutation in 15 cases was confusing. Previously, the R1193Q variant was reported in association with LQTS and BS.2122 This variant was present in 0.3%, 8%, and 12% of Caucasians, Asians,12 and the Han Chinese,22 respectively.
Subsequently, the variant R1193Q was considered a common polymorphism in Asian populations.27 However, the influence of the R1193Q mutation in BS and LQTS currently remains unclear. The genetic risk might be polygenic and, thus, the R1193Q mutation in the SCN5A gene could influence variants of other genes, not previously reported.28
Routine analysis of LQTS-related genes in postmortem examination of SIDS cases has been recommended since channelopathies may be caused by pathogenic variants in genes associated with structural heart disease.29 However, a recent review reported that the overall diagnostic yield of gene variants in SIDS cases was substantially lower than that in the Exome Aggregation Consortium (ExAC) 14% vs. 41%, respectively.30 No significant differences were found between SIDS and ExAC yields for any genes. The New Zealand study also showed that no significant pathologic variants were found in the non-selected series of SIDS.28 In our study, the diagnostic rate of the pathological variants related to LQTS was zero, subsequently could raise the question as to whether a routine molecular autopsy associated with LQTS would be necessary for all cases of SIDS.
The New Zealand study also showed few positive variants in SIDS study, which suggests that postmortem genetic testing in SIDS should be conducted in cases with a familial clinical history of sudden death or cardiac arrhythmia and the absence of risk factors such as a bed-sharing. Rare mutations associated with inherited cardiac diseases including LQTS, BS, and catecholaminergic polymorphic ventricular tachycardia (CPVT) could still explain more than 14% of SIDS cases.30 However, a molecular autopsy with large cohorts using next-generation sequencing (NGS) is still necessary.
Forensic pathologists have established archives of formalin-fixed, paraffin-embedded (FFPE) tissue samples. Although molecular analysis using FFPE tissue samples has shown comparable quality,31 the cost of genetic testing has increased compared to the test using DNA extracted from blood. Presently, there is an urgent need to establish a national tissue (blood) bank for SIDS in Korea. Moreover, to elucidate the genetic risk associated with SIDS, simultaneous genetic testing of parents and siblings with a familial history of sudden death, syncope, and clinically proven arrhythmia would be reasonable, which is also effective for genetic counseling.
However, in Korea, the decision to perform a medico-legal autopsy is made by public prosecutors, and the autopsy is typically performed if warranted, such as in suspicious deaths associated with a likely crime. Therefore, numerous cases of SUIDs were not pathologically investigated and no genetic counseling to prevent the sudden deaths of siblings has been established in Korea. Forensic molecular autopsy and valuable genetic counseling by clinicians should be performed to prevent SIDS.
This study has some potential limitations that need to be considered. First, FFPE could cause DNA fragmentation, resulting in low DNA yields, which could increase the risk of allelic locus dropout.32 In this study, the DNA extraction and TaqMan SNP assays were performed in triplicate for all the point mutations, which were confirmed using sequence analysis. Second, recent studies used large gene panels investigated using NGS,3334 which would likely be a more promising method to discover the etiology of SIDS than other methods. However, there was no blood preservation for SIDS cases and, therefore, we had to analyze small panels of LQTS genes. Currently, we are preserving blood samples of SIDS cases to perform prospective studies using NGS to target all channelopathy-associated genes including those related to LQTS, Brugada, CPVT, and structural cardiac genes.
Despite these limitations, this study has many strengths. For instance, to the best of our knowledge, this is the first report of genetic analysis in Korean SIDS. Most previous studies were conducted in Western countries.1011121314151617181920 Since other factors such as racial and environmental factors might be associated with SIDS, nationwide studies would have crucial implications. Second, this is the first study to focus on LQTS in SIDS in Korea. The collection of medico-legal autopsy data that provides the criteria for molecular autopsies in SIDS with clinical information including familial history for cardiac events is especially challenging in qualitative research in SIDS.
In conclusion, only 15 of the 85 DNA variants tested from 6 genes involved in the LQTS exhibited R1193Q in SCN5A with doubtful pathogenicity, and no pathogenic variants were observed. Considering the diagnostic yield in this study was close to zero, these findings suggest that molecular autopsy should be cautiously conducted in select cases with a familial clinical history to improve the quality and availability of genetic counseling for the families of victims. Furthermore, other factors affecting the sudden death of vulnerable infants should be investigated through comprehensive autopsy examinations since the development of SIDS is complex and multifactorial.
Moreover, it is necessary to establish a national young sudden death registry and investigative program including genetic counseling to explore the genetic background of inherited cardiac conditions including LQTS, BS, and CPVT as well as discover and assess genetic risk factors for SIDS in Korea.
Go to :
 XML Download
XML Download