

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Radon (222Rn) is a chemically inert, colorless, odorless, and tasteless gas that is produced in the course of the radioactive decay of uranium in soil and rocks.1 It diffuses from the ground to the air until it collapses, and has a half-life of about 3.8 days.2 Radon in outdoor air is rapidly diluted to negligible concentrations, and so, does not cause health concerns.3 However, in indoor environments such as houses and buildings, in which temperatures are generally higher compared to outdoor environments, a relatively negative pressure is formed and, consequently, radon flows into them from the ground. In winter, especially, when the temperature difference between the ground and indoor environments is huge and proper indoor ventilation is poor, radon that carried along the air flow can accumulate and reach high concentrations.45 Radon that enters the body through inhalation is accumulated in the lungs. Ionizing radiations, such as alpha rays that are released during decay, can cause DNA damage in the basal cells of the lungs and is known to increase the risk of lung cancer in the case of long-term exposure.2
The International Agency for Research on Cancer (IARC) classified radon and its decay products as human carcinogens, in 1988.6 The National Toxicology Program (NTP) in the US listed radon as a known human carcinogen, in 1994.7 The US Environmental Protection Agency (EPA), in 2003, concluded that radon is the second leading risk factor of lung cancer, in ever-smokers.38 However, the World Health Organization (WHO) noted that exposure to radon increases the risk of lung cancer, even in non-smokers.8
The geological structure of the Korean peninsula is the most important factor determining the origin and distribution of radon, in relation to the bedrock type.910 In the Republic of Korea (Korea), the distribution of granite tends to coincide with that of the Gangwon-do and Chungcheong-do regions, the surface soil of which have high radon concentrations. The United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCER) estimated the population-weighted average indoor radon concentration in the world to be 30 Bq/m3.11 Since 1989, in Korea, radon doses have been continuously measured, to estimate the annual average exposure in residential spaces.12 The arithmetic mean of the radon concentrations in the country, from 1989 to 2009, was estimated to be 62.1 Bq/m3; this is twice higher than the worldwide average.
Radon and cigarette smoke have synergistic effects and are known to increase the risk of lung cancer in smokers.313 Radon exposure concentrations, that are higher than the global average, are expected to contribute significantly to the incidence of lung cancer in Korean adult populations, which are associated with high smoking rates (more than 35% of the total population in the 1990s), relative to the rest of the world.14 However, few studies have evaluated the effects of long-term radon exposure on health, in Korea. Therefore, we estimated the disease burden associated with lung cancer caused due to exposure to residential radon, using national radon survey data.
METHODS
The process of estimating the disease burden of lung cancer due to residential radon exposure takes several steps. We have presented a flow chart (Fig. 1).
 | Fig. 1Flowchart for estimating disease burden of lung cancer attributable to residential radon exposure in Korea, 2013.DALY = disability-adjusted life years, YLL = years of life lost, YLD = years lost due to disability.
|
Residential radon concentration
We used nationwide radon survey data from the National Institute of Environmental Research, which conducted two surveys, from 2011 to 2014, in Korea. The survey for 2011–2012 was conducted on 10,946 houses that were selected based on the housing types. The survey for 2013–2014 was conducted on 8,000 houses.1516 The surveyed houses were selected considering the types of residential structures, such as detached houses, apartments, and multi-family dwellings. In multi-story buildings, only those living in the three floors above the basement were selected. Residential radon levels were measured over a period of 90 days in each house including winter season.
The nationwide radon survey, conducted in homes, measured radon concentrations only during winter, a season in which individuals were particularly vulnerable to indoor radon exposure. Therefore, using the data obtained from a nationwide radon survey, conducted in public facilities, which measured radon concentrations over four seasons in the same administrative district, the ratio of the annual average exposure and the exposure to radon in winter was calculated and converted to the annual average radon concentration in homes.17 The national average annual residential radon concentration in this study was calculated by applying 0.80 to the actual measured residential radon concentration in winter. This ratio is similar to the value (0.78) which was calculated through direct seasonal measurements in the Gangwon-do province.18 The annual average radon concentration in homes, across 234 administrative district units, was calculated as the annual average radon concentration of 17 provinces and metropolitan cities, using the population weight.
Exposure-risk relationship
We used the result of a previously conducted study that calculated the relative risk by using data on radon concentrations in Korean households, from 1999 to 2008, and lung cancer incidence data from the National Cancer Registry.19 The relative risk of the incidence of lung cancer due to radon exposure was estimated by applying a hierarchical Bayesian model after adjusting the prevalence of the smoking habit and the regional deprivation index, to examine the standardized incidence ratio (SIR) of lung cancer and radon concentration, in each region. The relative risk and 95% credible intervals of the incidences of lung cancer per 100 Bq/m3 were 1.105 (0.970, 1.268) for men, and 1.072 (0.914, 1.268) for women.19 The dose-response relationship between radon exposure and lung cancer incidence was assumed to be linear, and no threshold radon dose value was assumed.2021
Population attributable fraction (PAF)
The PAF for lung cancer, due to long-term radon exposure in Korean homes, was calculated using the following formula:
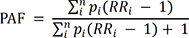
where Pi is the percentage of the population in relation to the level i of residential radon exposure, RRi is the relative risk at the exposure level i, and n is the total number of exposure levels.
The disease burden of lung cancer attributable to long-term radon exposure (AB) was calculated by multiplying the PAF by the total disability-adjusted life years (DALY) (or total deaths) from lung cancer (B).
The 95% confidence interval (CI) of the PAF was calculated using the Monte Carlo simulation method.
Disability weight (DW)
There are two sources of disability weights in the case of lung cancer. The Institute for Health Metrics and Evaluation (IHME), which is conducting a Global Burden of Disease (GBD) study, presents a general description of the health status of each disease and assigns disability weights, accordingly.22 The WHO cited the results of the IHME and then presented the DW according to the health status in the case of lung cancer.23 The results of the two institutions are almost similar, but we adopted the DW value obtained by the WHO. The health status in the case of lung cancer was described in four stages, and disability weights were applied accordingly. DW is applied when calculating the years lost due to disability (YLD), according to the health status.

Prevalencei is the prevalence of lung cancer in the health status level i, DWi is the disability weight in the health status level i, and n is the total number of health status levels.
Severity distribution of lung cancer in Korea
We categorized patients with lung cancer according to the stage of the disease and health status. Localized, regional, distant, and unknown stages were classified according to the extent of the metastasis.24 Unknown cases with intermediate 5-year survival rates, between the regional stage and the distant stage, were distributed in the aforementioned two stages. The terminal stage was classified based on whether or not patients were receiving medication.25
Morbidity and mortality data pertaining to lung cancer
The morbidity and mortality in 2013 were calculated by gender and age for lung cancer (C33–C34), using the national registration data of the National Cancer Center, and classified according to the ‘International Classification of Diseases and Related Health Problems, 10th Revision (ICD-10)’.
RESULTS
In order to estimate the population-weighted radon exposure (arithmetic mean) for the total Korean population, we estimated the distribution of house structures, annual mean radon concentrations, and populations according to each administrative area (Supplementary Table 1). The national distribution of the annual mean radon concentration was relatively high in mountainous terrains (Fig. 2). The highest annual mean radon exposure concentration at the district level was observed in Hwacheon (259.9 Bq/m3), Gangwon-do. The lowest value was observed in Jung-gu (25.8 Bq/m3), Busan. According to the structures of the houses, the annual mean exposure to radon was the highest 116.4 (± 50.4 as standard deviation) Bq/m3 in the case of detached houses. The corresponding level in the case of multi-family dwellings was 74.1 (± 30.0) Bq/m3, and in apartments, the level was at its lowest, 55.9 (± 21.1) Bq/m3 (Table 1). At the province level, the annual mean radon exposure concentration, applied by the population weight and distribution of house structures, was highest in Gangwon-do (110.9 Bq/m3) and the lowest in Ulsan (43.5 Bq/m3) (Supplementary Table 1). The population-weighted annual radon exposure concentration (arithmetic mean) in Korea was estimated to be 69.4 Bq/m3. The PAF for lung cancer was 0.066 (95% CI, 0–0.137) for men and 0.047 (0–0.134) for women. This suggests that, in Korea, 6.7% (0%–13.7%) and 4.7% (0%–13.4%) of all the cases of lung cancer, in men and women, respectively, was caused by residential radon exposure (Fig. 3).
 | Fig. 2Regional estimates of residential radon concentrations based on national radon survey data in Korea.
|
Table 1
Annual mean radon concentrationa, by house structure

| House structure | Annual mean radon concentration (Bq/m3) |
|---|---|
| Detached house | 116.4 ± 50.4 |
| Multi-family dwellingsb | 74.1 ± 30.0 |
| Apartment | 55.9 ± 21.1 |
All values are expressed as mean ± standard deviation.
aAnnual mean radon concentration by housing structure measured in 234 administrative districts; bMulti-family dwellings are not high-rise apartments, but buildings that are about five stories or less inhabited by several families.
![]()
 | Fig. 3Estimated population attributable fraction of lung cancer by administrative district in Korea.
|
Table 2 presents the DW and severity distributions, according to the health status. In the health status ‘Diagnosis and primary treatment,’ the DW was 0.294. Of all the lung cancer patients, 17.6% of the men and 20.0% of the women were categorized under the aforementioned health status; this status also had the lowest DW (Table 2). The largest percentage of lung cancer patients, at 43.8% of all the men and 48.6% of all the women, were classified into the ‘Terminal phase with medication’ category, while the smallest proportion, at 4.9% of all the men and 5.4% of all the women, fell under the category ‘Terminal phase without medication.’
Table 2
Disability weight and severity distribution, according to the health status in the case of lung cancer, in Koreaa

WHO = World Health Organization.
aDisability weight is a WHO estimate, and the severity distribution in male and female is estimated from lung cancer studies in Korea.
![]()
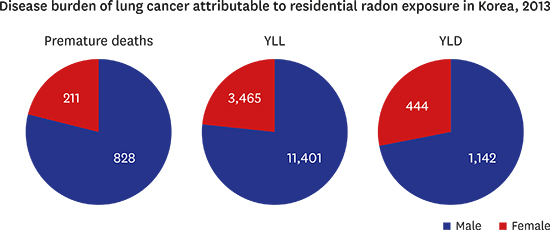
In 2013, the total disease burden of lung cancer attributable to residential radon exposure in Korea was 11,401 (0–23,654) years of life lost (YLL), 1,142 (0–2,361) YLD in men and 3,465 (0–10,148) YLL, 444 (0–1,306) YLD in women; the disease burden in men was about three times higher than that in women (Table 3). The number of premature deaths attributable to residential radon exposure in Korea was estimated to be 828 (0–1,713) in men and 211 (0–623) in women in 2013. The number of premature deaths among men was about four times higher than that among women (Table 3 and Supplementary Table 2).
Table 3
Disease burden of lung cancer attributable to indoor radon exposure, in Korea, 2013

Value: point estimate (95% confidence interval).
YLL = years of life lost, YLD = years lost due to disability.
![]()
DISCUSSION
There are two main methods of studying the risk of lung cancer attributable to residential radon exposure. One research method is the sixth Biological Effects on Ionizing Radiation Committee (BEIR-VI) risk model, which is widely used to estimate the health effects of residential radon exposure.1 The BEIR-VI model is based on mine worker studies exposed to radon. Lung cancer deaths from mine workers were associated with high concentrations of radon exposure, whereas lung cancer deaths from exposure to radon at home were low exposure, so extrapolation of results from mine worker studies was used.1 The BEIR-VI method, estimated through this extrapolation process, reported the results of the joint effects of smoking and radon. The synergistic effect of these two exposures in BEIR-VI model was characterized as submultiplicative, which is the intermediate between the multiplicative and additive.26 Under submultiplicative synergistic effect assumptions, the PAF for lung cancer due to residential radon exposure tend to be larger in non-smokers than in smokers.20 On the other hand, the BEIR-VI method, has a limitation in adjusting occupational exposures such as arsenic and diesel fumes in the mining environment that are not problematic in residential radon exposure studies.27
Another research method of residential radon exposure and lung cancer deaths was to assess the risk directly through case-control studies.2128 The European pooling study has the advantage of obtaining results based on real residential exposure data compared to the BEIR-VI risk model.20 In addition, since it is based on the exposure data of the residence, it is less influenced by the risk of lung cancer due to occupational exposure such as asbestos and arsenic. However, the European pooling study also reported that there was an error in classifying the smoking status and reflecting the variation in the radon concentration according to the residence space such as living room and bed room.20 Thus, these factors might induce underestimation of the risk levels in the European pooling study.29
The major differences between the two research methods are as follows. First, the effects of radon exposure on lung cancer deaths are different for smokers and non-smokers. Radon exposure in smokers is known to have a joint effect.13 Studies of mine workers exposed to high concentrations of radon showed that the increase in relative risk of lung cancer per unit radon exposure increase in non-smokers is substantially higher than in smokers, but, in residential radon exposure studies, about 11% risk increase was reported in nonsmokers at a statistically insignificant level.820 Second, the lung cancer risk of studies on mine workers vary with age at expression, but there is no age-related risk difference at expression in residential radon exposure studies.12030
In this study, we estimated the disease burden of lung cancer risk from residential radon exposure using the European pooling study method preferred by the Health Protection Agency in UK. The estimated disease burden of lung cancer was 11,401 (0–23,654) YLL, 1,142 (0–2,361) YLD in men and 3,465 (0–10,148) YLL, 444 (0–1,306) YLD in women. And the number of premature deaths was 828 (0–1,713) in men and 211 (0–623) in women, reflecting the PAF of lung cancers that are caused by residential radon exposure such as 6.7% (0%–13.7%) for men and 4.7% (0%–13.4%) for women. This was similar to the results of the IHME's GBD study, in which the PAF was found to be 5.4%, the disease burden 19,890 DALY, and the number of premature deaths 1,128 in total population of Korea.31
We estimated the disease burden of lung cancer, due to residential radon exposure, in Korea, based on residential radon measurement data, by house structure, that was collected from 2011–2014. The residential radon concentrations in 2011–2014 were found to be higher than those previously measured in 1989–2009.12 This may have been caused by the differences in the households selected for the survey. In addition, large variations were observed in the radon concentrations measured in winter, depending on the heating temperatures and ventilation rates, according to the outdoor air temperatures at the time of the measurement. In a study, which focused on hourly radon concentrations in indoor residential spaces, the radon concentration was found to gradually increase from the nighttime, peak at dawn and be at its lowest in the afternoon.32 Living rooms, which are main living spaces, were reported to have higher indoor radon concentrations than bedrooms.33 These effects were related to the presence of heating or ventilation, and whether or not windows were open; this implies that individual exposure concentrations can vary according to the time of day, at home. In the national radon survey, the concentration of indoor radon in multi-story buildings was measured only in the households located in the third floor or those below. It has been reported that in the lower stories (third story and lower) of high-rise buildings, such as apartments, the radon concentrations are 1.5-fold higher compared to those in the upper stories (tenth story or higher).34 Therefore, there is a possible overestimation of mean radon value in the apartments.34 In metropolitan areas, where the number of families living in apartments is higher, compared to rural areas, the possibility of overestimation may increase. It is also necessary to take into consideration that the radon concentrations in the indoor environments of high-rise apartments are known to be more influenced by emissions from building materials such as concrete and gypsum, rather than soil.
In calculating YLD, the median survival time in the case of advanced lung cancer was adopted as 8 months based on a previous report.35 In Korea, the cancer treatment for terminal phase cancer patients has undergone an aggressive change, and the median time period from the last chemotherapy session to death has been reported to be about 30 days.2536 Reflecting these finding, we applied the terminal phase with medication and terminal phase without medication at a ratio of 7:1. Since the severity distribution was estimated using data pertaining to the situation in Korea, it may vary from the global distribution.
The results of the PAF estimation varied depending on the risk calculation method.37 Based on the European Pooling Study method, it was found that the PAF of lung cancer due to residential radon exposure was 3.3% in the UK, 5.0% in Germany and France, 8.3% in Switzerland, and 8.3% in Korea.133839 However, studies which used the BEIR-VI method presented different results. It was reported that 8%–12% and 13.6%, of all the lung cancers were caused by residential radon exposure in France and Canada, respectively.1340 In Korea, which applied the BRIR-VI method, 13.5%–19.5% of all the lung cancer cases in men and 20.4%–28.2% of all the lung cancer cases in women were reported to be caused by radon exposure.38 Depending on the radon concentration data and the applied method, the PAF was estimated differently, but the European Pooling Study method was adopted by IHME, to calculate the disease burden of lung cancer attributable to residential radon exposure.41 In previous Korean studies based on the BEIR-VI risk model, PAF of other risk factors in lung cancer were estimated at 4.0%–4.5% in men except for the effects of smoking and radon. However, according to the GBD study, PAF for lung cancer in Korean men was 15.5% for air pollution due to ambient fine particulate matter (PM2.5), and 8.3% for insufficient fruit intake.31 In other words, the GBD study has relatively high PAF for lung cancer risk by other factors, and PM2.5 as ambient air pollutant is the second cause of lung cancer in Korea. WHO defines that PAF is the proportional reduction in mortality or diseases that would occur when the exposure as risk factor were reduced.42 Therefore, the sum of PAFs for individual risk factors can often exceed 100%. In the BEIR-VI method, PAF for lung cancer risk due to other factors tend to be underestimated in especially for men. Meanwhile, PAF of lung cancer risk due to residential radon exposure for Korean women were calculated as 20.4%–28.2% and other factors as 45.7%–51.7% in a previousstudy.38 The results of the GBD study on Korean women showed that PAF for lung cancer risk was 47.1% for smoking, 15.5% for ambient air pollution due to PM2.5, 11.2% for household air pollution related to cooking and 7.9% for insufficient fruit intake.31 In the GBD study, PAF of lung cancer risk due to residential radon exposure in Korea was calculated based on the European pooling study method and is 5.3% for the entire population.31
From the histological aspect of lung cancer, the risk of lung cancer by histological type per 100 Bq/m3 of radon exposure has been reported to be increased by about 31% in small cell carcinoma and by 6% in other type lung cancer in European pooling studies.21 In histological type of Korean female lung cancers, the adenocarcinoma was 34.6% and small cell carcinoma was 7.7% in 1999.43 The proportion of adenocarcinoma in Korean women continues to increase. In 2012, adenocarcinoma was 61.8% but small cell carcinoma was still 6.1% among all lung cancer.43 However, differences in the risk of lung cancer for radon exposure by histologic characteristics of lung cancer were not clear in studies of mine workers exposed to radon.20 This difference may be due to the effects of high concentrations of radon exposure in mine workers. Smoking rates in Korean women are slightly higher than in the past, but there is no significant difference. In addition, the residential radon exposure from past to current is gradually decreasing due to changes in the housing type and development of building technology. Therefore, it can be estimated that PAF of lung cancer due to residential radon exposure in Korean women is maintained at a certain level without fluctuations. The increased risk of lung cancer deaths in Korean women was greatly influenced by the increase in adenocarcinoma. Generally, this is not a pathologic type caused by smoking, nor is it to judge it as a pathologic type caused by residential radon exposure. Among lung cancer risk studies due to radon exposure, the results of studies on the histologic characteristics of lung cancer are insufficient. Therefore further studies are required to assess the risk associated with lung cancer histopathology for radon exposure.
In the case of lung cancers attributable to radon exposure, the effect size of the disease burden was determined by the relative risk and radon exposure level. Therefore, these two main factors were the key variables in interpreting the results of the present study. The relative risks applied in this study were calculated using ecological correlation studies, so the radon measurements obtained may not reflect the changes in individual exposures due to inter-regional migration. It was also difficult to reflect the changes in the structures of houses owing to rapid urbanization. However, in order to overcome these limitations, population-weighted radon concentrations were applied by calculating the house structure distribution and radon measurements for 234 administrative districts. It is considered that the processing of the detailed data, in the present study, produced reasonable results that are comparable to those of other international studies.
In 2014, it was estimated that 24,207 new cases of lung cancer were diagnosed in Korea, and that about 17,440 of these patients died of lung cancer.4445 The main reason for this was the high smoking rate (more than 35% of the total population in the 1990s) among Koreans, especially in the case of men (exceeded 70% in the 1990s), but the synergistic relationship between smoking and radon exposure was also a critical aspect as a risk factor.1446 In Korea, the smoking rates were higher in the rural areas, compared to the metropolitan and urban areas, and the radon exposure concentrations were also higher in the rural areas, in which the proportion of detached houses is higher than the proportion of apartments; in addition, a large number of these households are located in mountainous terrain.37 Socio-economically vulnerable groups, in whom the smoking rates were known to be high, were more vulnerable to radon exposure as a high percentage of these groups either live below the ground floor or in buildings that were built a long time ago and, thus, were likelier to have cracks.4748 As mentioned above, the incidence and mortality of lung cancer due to radon exposure, in Korea, was found to be higher in socio-economically disadvantaged populations. The PAF calculated in this study quantifies the magnitude of disease burden that can be reduced when the radon exposure level is lowered. Therefore, formulating a radon control policy is important in helping protect the rights of the aforementioned populations. It is suggested that the Korean government informs the public about the health benefits associated with reduced radon exposure and to enhance the risk communication.
This study estimated the disease burden based on the relative risk of lung cancer due to residential radon exposure and the population-weighted radon concentration by housing type in Korea. The average exposure level of the radon was 69.4 Bq/m3 in Korea. Premature deaths attributable to residential radon exposure was in 828 men (maximum 1,713 persons) and 211 women (maximum 623 persons). Residential radon concentration was highest in Gangwon Province, which has many mountainous areas. In residential type, the highest radon concentration was in detached houses near ground. Residents of detached houses in rural and mountainous areas are predominantly socio-economically disadvantaged population and their smoking rates are relatively high. Radon exposure levels vary significantly in Korea depending on the characteristics of the terrain and the type of residence. Therefore, effective intervention of lung cancer risks from residential radon exposure requires that more detailed levels of radon exposure be assessed in areas where vulnerable populations reside.
 XML Download
XML Download