

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
School crises, such as safety-accidents, school violence, and suicide have been steadily occurring in the world. In Korea, the most common cause of death among teenagers is suicide, and this accounts for a major part of school crises. According to the 2017 data published by Statistics Korea, suicide has been the top leading cause of death among young people aged 9 to 24 years since 2007. The suicide rate of teenagers is on a slight decline since 2011 at 8.9 deaths per 100,000 persons; however, teenage suicide is still a serious concern for the Korean government.
There are approximately 800,000 suicides a year worldwide, and it is estimated that at least six people are directly affected by each suicide death.1 Adolescents who have experienced peer suicide may be vulnerable to suicide intentions or attempts due to negative psychological symptoms including complicated grief, depression, anxiety or sadness.2 And they may experience difficulties with regard to major functions including academic achievement or social interactions to the adult period.3 Therefore early postvention would be helpful to assist suicide survivors through their grief process and prevent suicide in the future.456
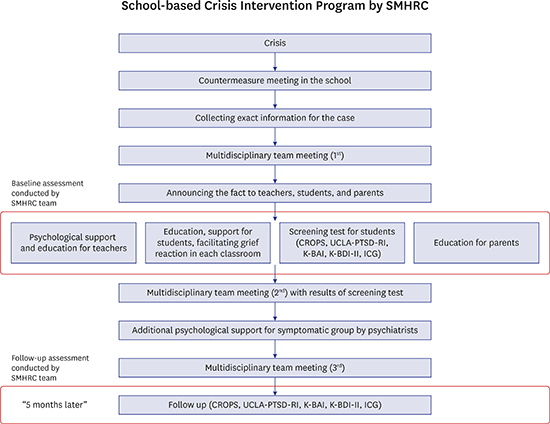
Policy initiatives of school-based crisis intervention programs to reduce the negative psychological impact of peer suicide have been carried out in Korea since 2012 by the School Mental Health Resources and Research Center (SMHRC) financed by the Ministry of Education. The SMHRC was established in 2012 to improve student mental health using evidence-based practices and aimed to be the national hub to support school mental health, to empower school teachers, and to foster trauma-informed schools by research, education and networking. A child and adolescent psychiatrist and professor is the director of the SMHRC, and the team consists of four social workers, three clinical psychologists, one administrative staff, and several part-time child and adolescent psychiatrists. One of the major projects undertaken by the SMHRC was the school crisis intervention program. When a student suicide occurs, the school reports to the Ministry of Education and the SMHRC team begins to apply the crisis intervention program. The typical sequence of the crisis intervention program is shown in the flow-chart (Fig. 1). Details may vary slightly depending on the circumstances of the school, and follow-up is only possible for the school with which the principal's consent was obtained.
 | Fig. 1Crisis intervention flow-chart. Baseline assessment: one week after the incident of student suicide and follow-up assessment: five months after the baseline assessment.SMHRC = School Mental Health Resources and Research Center, CROPS = Child Report of Post-traumatic Symptoms, UCLA-PTSD-RI = The University of California at Los Angeles PTSD reaction index, K-BAI = Korean-Beck Anxiety Inventory, K-BDI-II = Korean-Beck Depression Inventory-II, ICG = Inventory of Complicated Grief.
|
In Korea, more than 95% of the-school-aged youths attend school, and they spend considerable time there. Although Korean schools are an ideal setting to provide crisis intervention in terms of efficiency and structure, most Korean schools are reluctant to seek help and not even willing to share information about the traumatic events in schools. This is based on the direct experience of over 40 postventions of student suicide in more than 100 cases per year for 4 years at the SMHRC. Korean schools tend to have a very conservative atmosphere and vulnerability to criticism compared to those of western countries. Undertaking responsibility for a crisis is a serious issue in the Korean society. The Confucian cultural background may also influence people to regard suicide as a major fault; thereby leading schools to make efforts to avoid being stigmatized.
To the best of our knowledge, there has been no previous study on school-based postvention in Korea. Studies on children and adolescents who have experienced traumatic events are also scarce in Korea. Kim et al.7 examined the symptoms of post-traumatic stress and anxiety/depression in Korean children after direct or indirect exposure to a single incident of trauma during a fire escape drill. They provided important evidence that various anxiety/depressive disorders, in addition to post-traumatic stress disorder (PTSD), might occur following a direct or indirect exposure to trauma.7 This indicates that a precise diagnosis and persistent management are required to alleviate depression or post-traumatic symptoms to maintain the mental health of students exposed to a trauma. Another study conducted in Korea showed that children's depressive symptoms after being exposed to accidental death during a fire escape drill predicted lower quality of life in children and higher parental rearing stress after 2 years.8
The primary goal of this prospective cohort study was to follow-up post-traumatic stress, depression, anxiety, and complicated grief in Korean high school students who experienced the mental trauma of peer suicide in the same school. A previous large epidemiological survey in the United States found higher lifetime prevalence rates of Diagnostic and Statistical Manual (DSM)-IV PTSD among female adolescents (7.3%) than that among male adolescents (2.2%).9 The secondary goal of this study was to examine the differences in post-traumatic stress, depression, anxiety, and complicated grief between male and female students.
METHODS
Participants
On March 5, 2016, a third-grade high school student in Korea committed suicide in her home by hanging. Immediately after the suicide incident, the SMHRC team provided the crisis intervention program to the remaining students and teachers. A total of 1,032 adolescents and their parents who experienced the peer suicide in 2016 signed a written agreement to participate in this follow-up study. Among them, a total of 956 (girls 506, boys 450) students who provided sufficient data were finally included in the statistical analysis. Participants were divided into two groups according to the Child Report of Post-traumatic Symptoms (CROPS) scores at baseline assessment. The students with the CROPS score of 19 or higher were classified as ‘trauma group’ and the students with the CROPS score of less than 19 were classified as ‘non-trauma group.’
Procedure
Fig. 1 is a flow-chart of the study procedure. This study was conducted in the course of a crisis intervention program in one school, where the incident of student suicide suddenly occurred, provided by the SMHRC upon the official requests from the school, regional office of Education and the Ministry of Education. The crisis response team of the SMHRC consists of child and adolescent psychiatrists, clinical psychologists, and social workers. The study team visited each school more than thrice during the intervention, investigated each case, and provided consultation to teachers in a supportive way.
First, after talking to the school principal, vice principal, and teachers during the first multidisciplinary team meeting, the study team got agreement from the principals to conduct follow-up study and analysis. After the first meeting, we helped the school to inform all teachers, students, and parents. Education, as part of postvention, comprising contents related to the promotion of normal grief reaction and coping was provided to each class for 50 minutes one week after the incident of peer suicide. It was also conducted for teachers and parents separately.
In addition to these educational sessions, screening tests were conducted for all students to measure the post-traumatic symptoms (CROPS), the post-traumatic stress symptoms (The University of California at Los Angeles PTSD reaction index; UCLA-PTSD-RI), the anxiety symptoms (The Korean-Beck Anxiety Inventory; K-BAI), the depressive symptoms (The Korean-Beck Depression Inventory-II; K-BDI-II), and the complicated grief reaction (The Inventory of Complicated Grief; ICG). The demographic information was also collected. For a selected symptomatic group of students, the psychiatrists visited the school, conducted individual interviews up to three times for each student, and helped with referral if necessary. The crisis intervention program was carried out by following this process. According to the school conditions, the follow-up tests were performed 5 months later, and all the screening tests initially conducted were performed again.
Assessment
CROPS
The CROPS is a 26-item self-report measure of post-traumatic symptoms for the previous seven days designed for individuals ages 6 through 18. This is a 3-point Likert scale (0 = none, 1 = some, 2 = lots). Higher scores reflect more post-traumatic stress symptoms.10 A total score can range from 0 to 52, and a total score of 19 is considered as a cutoff point for significant post-traumatic symptoms. The Cronbach's α for the Korean version of CROPS was 0.91.11
UCLA-PTSD-RI
UCLA-PTSD-RI is a PTSD measurement tool that meets the PTSD diagnostic criteria of DSM-IV-TR. The 9-question UCLA-PTSD-RI asks about PTSD symptoms, guilt, and trauma. The students with a score of 10 or higher have severe PTSD symptoms. The internal consistencies of the 9- and 8-item versions of the Abb-UCLA PTSD RI-Korean were found to be high (Cronbach's α = 0.843 and 0.842, respectively).12
K-BAI
The Beck Anxiety Inventory (BAI) is a 21-item multiple-choice self-report inventory that measures the severity of an anxiety designed for individuals aged 14 and over. The Cronbach's α ranges from 0.92 to 0.94 and test-retest reliability is 0.75.13 A total score of 0–7 is interpreted as a ‘Minimal’ level of anxiety; 8–15 as ‘Mild’; 16–25 as ‘Moderate’; and 26–63 as ‘Severe.’ The Cronbach's α and test-retest reliability for the Korean version of BAI were 0.90 and 0.84, respectively.14
K-BDI-II
The Beck Depression Inventory (BDI) is a 21-question multiple-choice self-report inventory, one of the most widely used psychometric tests for measuring the severity of depression.15 The BDI-II is designed for individuals aged 13 and over, and is composed of items relating to symptoms of depression. A total score of 0–13 is interpreted as a ‘Minimal’ level of depression; 14–19 as ‘Mild’; 20–28 as ‘Moderate’; and 29–63 as ‘Severe.’ The Cronbach's α for the Korean version of BDI-II total score was 0.89. The correlation between the BDI-II and the Patient Health Questionnaire-9 (PHQ-9) was strong (r = 0.75).1617
ICG
The ICG measures symptoms associated with loss, which is distinct from depression and anxiety. The 19-item, self-report ICG is composed of questions asking about sickness such as longing for the dead, feeling overwhelmed by death, guilt, and self-blame. The ICG is a 5-point scale, meaning that the higher the score, the greater the mood response to loss. The Cronbach's α and the test-retest reliability for the Korean version of ICG were 0.87 and 0.75, respectively.18
Statistical analysis
All statistical analyses were performed using SPSS statistics (version 21.0; IBM Corp., Armonk, NY, USA). For demographic data, χ2 test and independent sample t-test were used. For before-and-after comparison in each group, paired sample t-test was performed. To show the effect of the intervention among two groups in post-traumatic stress symptoms, depression, anxiety, and complicated grief with the passage of time, repeated measure analysis of variance (ANOVA) was performed. To identify risk factors, logistic regression analysis was utilized.
RESULTS
Table 1 shows the demographic characteristics of the two groups. Of all students, 83 students were classified as trauma group with significant post-traumatic stress symptoms. Among them, 57 (68.7%) students were female and 26 (31.3%) students were male. Using logistic regression analysis, only female sex was analyzed as a risk factor for the higher CROPS scores at baseline assessment (odds ratio = 1.79; P = 0.03). Other than sex, there were no demographic factors associated with the higher CROPS scores.
Table 1
Demographic data

Data are presented as means ± standard deviation (range) or number (%).
CROPS = Child Report of Posttraumatic Symptoms, SES = subjective economic status.
![]()
Paired sample t-test revealed statistically significant differences in the CROPS, the UCLA-PTSD-RI, the K-BAI, the K-BDI-II, and the ICG scores between baseline and follow-up assessments in both groups (Table 2). Fig. 2 shows the effects of the time passage and the group differences. Repeated measure ANOVA revealed that the scores of the ‘trauma group’ dropped more sharply in the CROPS, the UCLA-PTSD-RI, the K-BAI, the K-BDI-II, and the ICG compared to those of the ‘non-trauma group’ (Fig. 2). This indicated that the postvention was helpful to reduce the post-traumatic stress symptoms, anxiety and depressive symptoms, and complicated grief reaction among trauma group.
Table 2
Comparison of baseline and follow-up assessment

CROPS = Child Report of Post-traumatic Symptoms, UCLA-PTSD-RI = The University of California at Los Angeles PTSD reaction index, K-BAI = Korean-Beck Anxiety Inventory, K-BDI-II = Korean-Beck Depression Inventory-II, ICG = Inventory of Complicated Grief, B = baseline, F = follow-up.
![]()
 | Fig. 2Changes in the clinical scales (repeated measure analysis of variance). Baseline: one week after the incident of student suicide, Follow-up: five months after the baseline assessment, and Statistics: CROPS (F = 260.4, P = 0.00), UCLA-PTSD-RI (F = 136.8, P = 0.00), K-BAI (F = 127.9, P = 0.00), K-BDI-II (F = 105.2, P = 0.00), ICG (F = 86.4, P = 0.00).CROPS = Child Report of Post-traumatic Symptoms, UCLA-PTSD-RI = The University of California at Los Angeles PTSD reaction index, K-BAI = Korean-Beck Anxiety Inventory, K-BDI-II = Korean-Beck Depression Inventory-II, ICG = Inventory of Complicated Grief.
|
Fig. 3 shows the point prevalence rates of the symptoms of anxiety, depression, and post-traumatic stress among female and male students. The symptomatic group included students with scores greater than or equal to the cutoff value on the CROPS, the UCLA-PTSD-RI and, the ICG and those with moderate to severe scores on the K-BAI and, the K-BDI-II. The 9.09% of the female students and 4.44% of the male students showed significant post-traumatic stress symptoms on the CROPS at baseline assessment. The rates of symptomatic group with post-traumatic stress, anxiety, and depressive symptoms were higher among the female students than the male students at both assessments.
 | Fig. 3Symptomatic group rate at baseline and follow-up assessment.CROPS = Child Report of Post-traumatic Symptoms, UCLA-PTSD-RI = The University of California at Los Angeles PTSD reaction index, K-BAI = Korean-Beck Anxiety Inventory, K-BDI-II = Korean-Beck Depression Inventory-II, ICG = Inventory of Complicated Grief, B = baseline, F = follow-up.
|
DISCUSSION
This is a prospective cohort study, which demonstrates the process of school-based crisis intervention programs conducted in one Korean high school and provides the before-and-after comparison of the program. The intervention was performed among high school students after the incident of student suicide. The participants were divided into the ‘trauma group’ and the ‘non-trauma’ group according to the scores of the CROPS. At baseline assessment, 8.6% (n = 83) of the students scored 19 or higher on the CROPS. This finding is comparable with those of previous studies on post-traumatic disorders. Overall, 6.7% of the adolescents met the diagnostic criteria for PTSD since the spring 2011 tornado outbreak in Alabama and Joplin, Missouri.19 Another prior study found that as many as 36% of the children and adolescents exposed to a range of traumatic events were diagnosed with PTSD.20 A recent meta-analysis reported that the rate of PTSD among children after trauma exposure is approximately 15.9%, which varied according to the type of trauma and gender.21 However, the rates of PTSD among children and adolescent disaster survivors vary widely depending on the studied population and the measures used to assess diagnosis, with rates ranging from 1% to 60%.22 The measures used to assess post-traumatic symptoms in this study were different from those used in previously mentioned studies, therefore, it may be inappropriate to directly compare the outcomes without considering any demographic factors, types of traumatic events, and the clinical differences.
After the intervention, 2.9% (n = 28) of the students still remained in the ‘trauma group’ at the five months follow-up assessment. And the ‘trauma group’ still shows higher scores than the ‘non-trauma group’ after five months follow-up. Although intervention has helped to reduce symptoms in the trauma group, the five months follow-up period was a short time to complete recovery in the Trauma group. Hong et al.23 conducted a thirty months prospective follow-up study for children exposed to a single incident of psychological trauma in Korea. They classified four groups of children named ‘recovery’ (19.9%) with initially high and then gradually decreasing PTSD symptoms, ‘resilience’ (72.7%) with consistently lower level of PTSD symptoms, ‘chronic dysfunction’ (1.8%), and ‘delayed reaction’ (5,6%) according to Bonanno's conceptual model.23 The Recovery type demonstrated a favorable outcome at thirty months follow-up but still showed more considerable PTSD symptomatology than the Resilience type.23 It is understandable in this context that there is a difference in trauma scores between the Trauma group and the Non-trauma group after intervention in our study.
Recent studies have shown an increasing recognition of gender differences in PTSD, with women having twice the rate of the disorder compared to men.24 A significantly higher symptom severity with respect to trauma experience has been found among girls compared to boys.25 Sex differences in trauma experience were also observed in this study. The symptomatic group rate of female students was higher than that of male students on all the scales at baseline assessments (Fig. 3). It suggested that higher proportion of the female students showed post-traumatic stress symptoms, anxiety and depressive symptoms, and complicated grief reaction than the male students after the incident of peer suicide.
According to the results of the paired sample t-test and the repeated measures ANOVA, the school-based crisis intervention program conducted in this study was effective in reducing post-traumatic stress symptoms, anxiety, depressive symptoms, and complicated grief (Table 2 and Fig. 2). The most important finding of our study was that after a crisis, such as a student suicide occurring in a school, the remaining students might experience complicated grief, symptoms of anxiety, depression, and post-traumatic stress. These symptoms might spontaneously improve over time. However, prior studies have shown that the course of PTSD without treatment is largely a chronic one.26 In a study conducted in Korea, 1.8% of elementary school students who witnessed deaths had chronic dysfunction, and 5.8% of them had delayed traumatic reaction after 30 months.23 The scarce research in adolescents also points to possible chronicity of PTSD symptoms in this population.27 Many individuals recover from PTSD without treatment, and the steepest decline in rates of PTSD is usually seen in the first year.28 This still leaves a substantial minority — roughly a third — who are likely to develop a chronic disorder which may persist for years if left untreated (National Institute for Health and Care Excellence [NICE], 2005).28 Therefore, for them, providing appropriate psychological support, including educational intervention and screening tests could possibly facilitate the process of alleviating the symptoms. Several previous studies have demonstrated that performing postvention for the suicide survivors has a positive association with lower post-traumatic symptomatology.2930 Furthermore, postvention may prevent acting out of unspoken trauma and suicidality among the potentially bereaved and depressed adolescents exposed to suicide.31
There are limitations to this study. First, this study was conducted during the process of providing crisis intervention services to schools with the support of the Ministry of Education; it was difficult to conduct a long-term follow-up study because the timing of the follow-up was determined according to the circumstances of the schools. Second, various psychosocial factors were not examined. A meta-analysis of 64 studies assessing risk factors for PTSD among children and adolescents aged 6 to 18 revealed that factors relating to the subjective experience of the event (including peri-trauma fear and perceived life-threat) and post-trauma variables (including low social support, social withdrawal, psychiatric comorbidity, poor family functioning, and the use of certain cognitive strategies such as distraction and thought suppression) accounted for medium-to-large effect sizes in the prediction of PTSD, while pre-trauma factors (including female gender, low intelligence, low socioeconomic status, pre-trauma life events, pre-trauma low self-esteem, pre-trauma psychological problems in the youth and parents) accounted for only small-to-medium effect sizes.32 In future studies, it is important to identify these risk factors. Third, the level of intimacy between the student who committed suicide and the suicide survivors was not assessed. It may affect the post-traumatic stress symptoms and depressive symptoms. Finally, we could not assess any preexisting psychopathology prior to the peer suicide.
However, our findings are meaningful in that this is the first study to demonstrate the process of school crisis intervention in Korea and examine its effectiveness. Furthermore, it is also important that the findings of this study are used as the basis for devising policies to support schools in the event of a crisis such as student suicides.
Our findings indicate that the students who experienced the traumatic event of peer suicide in the same school suffered from various symptoms, such as complicated grief, anxiety, depression, and post-traumatic stress. This suggests that school-based crisis intervention when a peer suicide occurs helps improvement of these trauma-related symptoms. It might be an effective way to prevent suicide spreading among students by alleviating trauma-related symptoms.
 XML Download
XML Download