

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Gallbladder (GB) cancer is a highly aggressive malignancy and surgical resection is the only effective treatment, as there are currently no effective systemic treatments. Although most guidelines1234 suggest that T2 GB cancer should be treated by extended cholecystectomy (ECx) and there is widespread consensus among surgeons, practically the rate of performing ECx is far lower than the expectation56789 and several studies1011121314 have reported that a less extensive procedure consisting of cholecystectomy with lymphadenectomy and without hepatectomy is an effective surgical procedure for T2 GB cancer. Therefore, adequate surgical extent of T2 GB cancer has remained as a major clinical interest to hepatobiliary surgeons. Low incidence of this disease has prevented randomized trials designed to assess appropriate surgical procedures, which has hindered the formulation of evidence-based guidelines.
In this study, the Korean Pancreas Surgery Club (KPSC), as one of the nations in which GB cancer is most prevalent in the world, undertook nationwide multicenter study, which involved 14 university hospitals, to investigate the clinical features and clinical outcomes of T2 GB cancer and to determine appropriate surgical strategy.
METHODS
This study was designed by the KPSC Scientific Committee. A workshop was held on June 12, 2014, to approve the study design and to agree on a questionnaire. Subsequently, a nationwide survey was undertaken at 14 university hospitals (tertiary hospitals), located in seven Korean provinces. KPSC members were required to complete the questionnaire and a case registration form for each patient that underwent surgery for pathologically proven T2 GB cancer. To obtain the actual survival data, we confined the study period from January 1, 2000, to December 31, 2009, which allowed the latest case achieves 5 postoperative years. Clinicopathologic findings and long-term follow-up results were analyzed as predetermined by the KPSC workshop.
Tumor stage was determined according to the seventh edition of the American Joint Committee on Cancer (AJCC) staging system.15 T2 GB cancer was defined as cancer confined to perimuscular connective tissue and no extension beyond serosa or into liver and extent of nodal disease was transformed into the categorical variables, N0, N1, and N2. Operative procedures were defined as follows. Simple cholecystectomy (SCx) was defined as cholecystectomy alone and ECx as cholecystectomy, liver wedge resection or segment 4b and 5 segmentectomy and regional lymph node (LN) dissection. Although no consensus was reached regarding the extent of regional LN dissection, for the questionnaire survey all participating surgeons responded that they routinely dissected pericystic LN and nodes around the hepatoduodenal ligament. Even for SCx, an achieved pathologically negative surgical margin was regarded as R0 resection. Para-aortic LN metastasis was regarded as distant metastasis (M1) and surgery for these patients were defined as palliative resection.
Continuous data are expressed as means ± standard deviations. Categorical variables were compared using Pearson's χ2 test, and continuous variables using the Mann-Whitney U test. All parameters with a P value of < 0.05 by univariate analysis were included in the multivariate model. Overall survival time was calculated from date of operation to date of last follow-up for surviving patients or to the date of death due to GB cancer. Survival statuses and cause of death were confirmed with the assistance of the Korean Ministry of Public Administration and Security. Survival was calculated using the Kaplan-Meier method, and differences were analyzed using the log-rank test. A Cox regression model was used to identify prognostic factors. The statistical analysis was performed using SPSS ver. 18.0 for Windows (SPSS, Chicago, IL, USA).
RESULTS
Demographics and clinical presentations
A total 410 patients were included in this study. The male to female ratio was 1:1.2, mean patient age at diagnosis was 64.1 ± 10.2 years (range, 34–87) and mean follow-up period was 63.5 ± 10.6 months (range, 2.2–181). In preoperative findings, abdominal pain was the most common symptom (60.4%) and GB abnormality was detected after routine check-up in about 26% of the patients without symptom. In 133 patients (32.4%), GB cancer was incidentally detected after cholecystectomy under suspicion of benign GB disease.
Surgical interventions and postoperative morbidity and mortality
SCx was performed in 193 patients (47.1%). Among them, LN dissection with SCx was performed in 64 (33.2%) patients. A second operation after SCx was performed in 74 of 267 patients (27.7%) and there were no residual tumors at GB bed in all 74 resected specimens. ECx was performed in 206 patients (47.8%). Among them, liver wedge resection was performed in 161 patients (60.0%) and segment 4b and 5 segmentectomy was performed in 45 patients (40.0%). Six patients underwent extended right hemihepatectomy and five patients underwent pancreaticoduodenectomy and ECx. These 11 patients were classified into the ECx group in the following analyses.
Curative resection (R0) was performed in 360 patients (87.8%). Palliative resection was conducted in 50 patients (12.2%). Para-aortic LN metastasis was detected in 17 patients (17/410, 4.1%). In 19 patients (19/50, 38%), although tumor cells at the cystic duct margin confirmed at permanent pathology, they refused further operation. In 5 patients, liver metastases distant from liver bed were detected intraoperatively and three patients had peritoneal seedlings.
Postoperative morbidities occurred in 29 patients (7.0%). There were seven postoperative deaths (1.7%) due to sepsis or respiratory failure.
LN metastasis
LN dissection was performed in 281 patients (68.5%). The mean overall number of retrieved LN was 5.52 (range, 1–20) and 21 patients (21/281 = 7.4%) had fewer than 3 retrieved LNs. LN metastasis occurred in 100 patients (100/281, 35.6%). Among them, 83 patients (83.0%) had N1 LN metastasis and 17 patients (17%) had N2 LN metastasis.
Recurrence
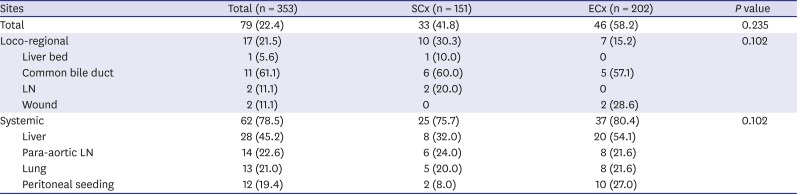
Among 353 patient who underwent R0 resection excluding 7 patients having in-hospital mortality, 79 patients (22.5%) experienced disease recurrence during the mean 63.5 ± 10.6 months follow-up period. Systemic recurrence (n = 62, 78.5%) was more common than locoregional recurrence (n = 17, 21.5%). Eight patients developed locoregional recurrence and systemic metastasis simultaneously, and 15 patients developed systemic metastasis at more than two sites. Median time to recurrence was 12.5 months. Recurrence occurred in 33 patients (33/79, 41.8%) after SCx and in 46 patients (46/79, 58.2%) after ECx (P = 0.235). Recurrence patterns and sites by operation type are summarized in Table 1. The rate of liver metastasis in the group that underwent liver bed wedge resection and in the group that underwent 4b and 5 segmentectomy was not significantly different (6.7% vs. 13.3%, P = 0.273). Recurrence in the liver bed occurred in one patient who had undergone open cholecystectomy. Two patients experienced recurrence at the surgical wound after ECx, but there was no case of port site recurrence. Recurrence occurred more frequently in patients with LN metastasis (27.8% vs. 14.7%, P = 0.026), preoperative elevated level of serum carcinoembryonic antigen (CEA) (20.8% vs 9.8%, P = 0.035) and serum cancer antigen (CA) 19-9 (41.2% vs. 18.3%, P = 0.001). There was no significant difference in recurrence free survival and recurrence pattern in terms of operative procedures, especially between SCx and ECx and whether to perform LN dissection or not.
Table 1
Recurrence patterns and sites according to operations
Long-term survival
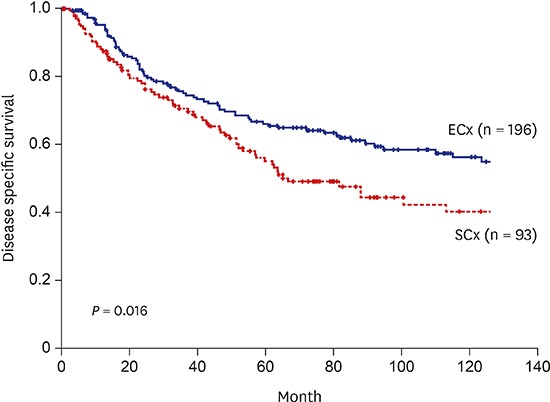
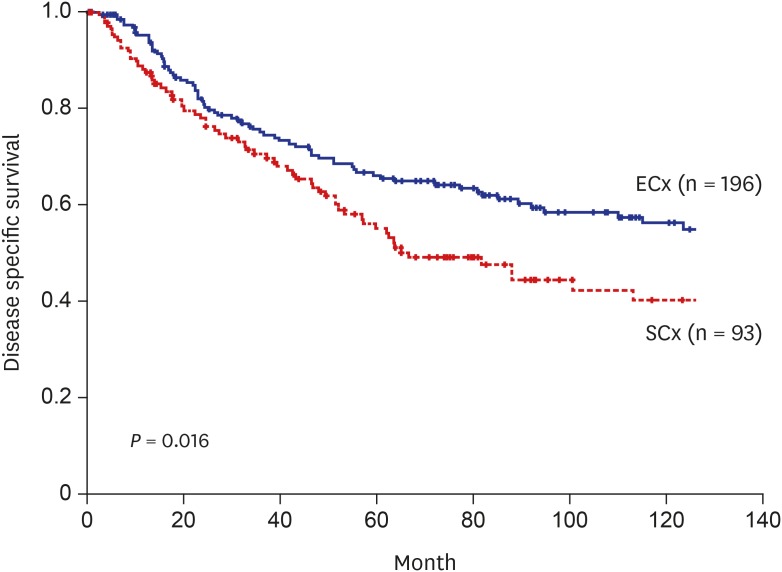
The 5-year cumulative survival rate (5YSR) for the patients who underwent curative resection was 61.2%, while that for the patients who underwent palliative resection was 11.4% (P < 0.001). The patients without LN metastasis (N0) showed better survival than the patients with LN metastasis or unknown LN metastasis status (73.4% vs. 39.8% vs. 52.2%, P < 0.001). A comparison between N1 and N2, N1 group showed better survival than N2 group (39.8% vs. 6.7%, P < 0.001). For the patient who underwent curative resection, LN dissection group showed better survival than the group without LN dissection (63.6% vs. 53.5%, P = 0.047). ECx group showed better survival than the SCx group (65.4% vs. 54.0, P = 0.016) (Fig. 1). There was no significant difference in the 5YSR between the group that underwent ECx as an initial operation and the group that underwent ECx after second operation (64.9% vs. 68.7, P = 0.977). The 5YSR was 65.7% in the group of patients who underwent wedge resection of the GB bed and 63.2% in the group of patients who underwent 4b and 5 segmentectomy (P = 0.795). Especially for N0 patients there was no significant difference in 5YSR between SCx and ECx groups (68.7% vs. 73.6%, P = 0.173). In SCx group, 5YSR was not significantly different between open and laparoscopic cholecystectomy groups (52.7% vs. 53.1%, P = 0.895).
Prognostic factors
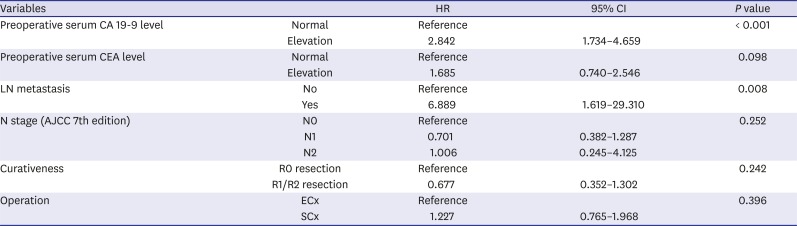
Univariate analysis showed that preoperative elevated serum CEA level, preoperative elevated serum CA 19-9 level, LN metastasis, N1, 2 stage (AJCC 7th edition), operation (SCx), surgical curativeness (R0 vs. R1/R2) were significant prognostic factors (Table 2). However, multivariate analysis using the Cox proportional hazard model revealed that preoperative elevated serum CA 19-9 level (hazard ratio [HR], 2.842; P < 0.001) and LN metastasis (HR, 6.889; P = 0.008) significantly predicted poor prognosis (Table 3).
Table 2
Univariate analysis of prognostic factors
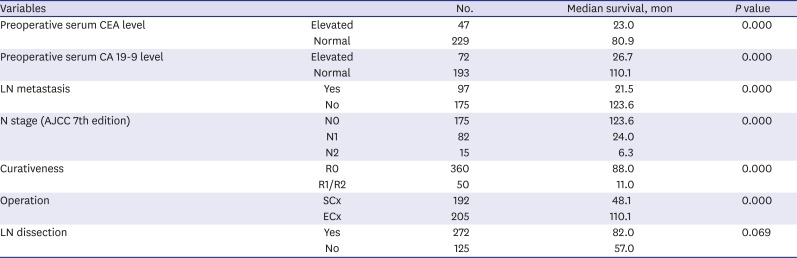
Table 3
Multivariate analysis of prognostic factors
DISCUSSION
GB cancer is an aggressive disease with late presentation, rapid progression, early recurrence, and dismal outcome. The depth of penetration (T classification) is a critical prognostic factor in patients with GB cancer and the criteria to make a decision which operative procedure will be performed. For T2 GB cancer, published guidelines1234 recommend ECx, although they are based on retrospective studies on relatively few selected patients and furthermore, the rate of performing ECx was far lower than the expectation to discuss statistical significance.56789 The present study that enrolled relatively large patients in one of the most prevalent region on GB cancer showed better survival of ECx than SCx in curatively resected patients (65.4% vs. 54.0%, P = 0.016). However, in subgroup analysis, especially for N0 patients, there was no significant difference in 5YSR between SCx and ECx groups (68.7% vs.73.6%, P = 0.173). Several studies1011121314 showed comparable survival in a less extensive procedure consisting of cholecystectomy with lymphadenectomy and without hepatectomy to that in ECx as the present study and they consisted of a large number of patients without LN metastasis. Although this suggests that the patients with T2 GB cancer and no LN metastasis could be the indication of SCx, till now we cannot diagnose depth of invasion and LN metastasis preoperatively. Therefore, ECx would be the adequate surgical strategy of T2 GB cancer. Since most of the patients with GB cancer tend to be elderly and incidentally detected GB cancer, which needs second operation according to the current guidelines,1234 is increasing, the effort to find the criteria of less invasive surgical procedure would be meaningful and development of diagnostic imaging tool should proceed concurrently.
LN metastasis is one of the well-known prognostic factors of GB cancer. For T2 GB cancer, it ranges from 33% to 62%.5678161718 In the present study, LN metastasis was one of the proven prognostic factors in multivariate analysis and LN dissection group showed better survival than the group without LN dissection (63.6% vs. 53.5%, P = 0.047). This suggests that LN dissection should be performed routinely for T2 GB cancer. Although recently published AJCC 8th edition changed N stage on the basis of number of positive LNs, the present study demonstrated survival difference according to the location of positive LNs, i.e., N1 group showed better survival than N2 group (39.8% vs. 6.7%, P < 0.001). Further evaluation for N stage according to location and number of LNs should be performed.
Recently, several studies192021 focused on the tumor location in the GB as a prognostic factor and criteria of selection of surgical procedure in T2 GB cancer. The GB has a unique anatomical character, with half of its body being attached to the liver, with a hepatic side and peritoneal side. This location might be the risk of tumor invasion and the mode of cancer spread. However, how to define the hepatic side and the peritoneal side (i.e., histopathological definition19 or radiological definition2021) is not yet established. This inconsistent definition might cause the different results of recently published studies192021 and the clinical significance of the location of the tumor has not yet been clarified. However, AJCC 8th edition divided T2 tumor into T2a and T2b according to the location of tumor based on the study by Shindoh et al.19 that defined the location histopathologically. The pitfall of the histopathological definition is that for SCx or for tumor located near the cystic duct or GB neck, it is impossible to classify the location. Because the present study is retrospective multicenter study, the information of tumor location could not be obtained. Consensus for the definition of tumor location should be achieved and on the basis of the definition, further well-designed large-scale study should be performed.
For T2 GB cancer, partial hepatectomy is thought to be valuable in the aspect of achievement of tumor-free margin on the liver side and prophylactic resection to prevent liver metastasis.16 Wedge resection of GB bed and 4b+ 5 segmentectomy has been used for these purposes. The rationale of 4b+ 5 segmentectomy is removal of micrometastases in the liver. However, the results that residual disease on the resected GB bed was rare than expected including the present study.1622 The common recurrence in the liver was not local recurrence at the liver bed but systemic recurrence at multiple sites. And it raises questions about the need for more extended liver resection and about the possibility to prevent hematogenous liver metastasis by an extension of resected hepatic segments to 4b+ 5. The present study demonstrated that there was no significant difference in 5YSR between the group of patients who underwent wedge resection of the GB bed and the group of patients who underwent 4b and 5 segmentectomy (65.7% vs. 63.2%, P = 0.795). Therefore, though a multicenter randomized controlled study should confirm this, the extent of hepatic resection is not a prognostic factor of T2 GB cancer and wedge resection of GB bed could be the proper procedure for ECx.
Little information has been published on the recurrence rates and patterns of T2 GB cancer. In the present study, systemic recurrence was found to be more common than locoregional recurrence (78.5% vs. 21.5%), and recurrence occurred more frequently in patients with LN metastasis (27.8% vs. 14.7%, P = 0.026). Based on this pattern of disease recurrence and risk factor, effective postoperative adjuvant therapy should be considered especially for the patients with LN metastasis. However, in the present study, unfortunately, because no standard postoperative treatment or indications for treatment have been established and adjuvant regimens were so diverse, analysis was pointless. Because there is a paucity of evidence provided by randomized trials, adjuvant therapy guidelines for GB cancer are based on retrospective data and expert opinion. Hence, a multicenter, large-scale prospective study is warranted to validate the efficacy of adjuvant treatment strategies in GB cancer.
Although the present study had a retrospective design and limitations, there are several strengths. First, the present study is one of the largest studies on T2 GB cancer in the world from one of the countries with high prevalence of GB cancer. Second, the information used was relatively precise because the participated surgeons performed the operations themselves and had long-term follow-up data on most of the patients enrolled, which should allow analysis of recurrence data as a distinct characteristic from other nationwide studies.
Summarizing, ECx showed better survival than SCx in terms of survival in T2 GB cancer and wedge resection of GB bed could be the proper extent for ECx. Therefore, ECx should be recommended for T2 GB cancer. However, in subgroup analysis, especially for N0 patients, there was no significant difference in 5YSR between SCx and ECx groups; and further study for the criteria of less invasive surgical procedure is needed. Because systemic recurrence was more common and recurrence occurred more frequently in patients with LN metastasis, postoperative adjuvant therapy should be considered especially for the patients with LN metastasis. Now Korean nation-wide database on GB cancer is under construction and in the near future further discussion would be possible.
 XML Download
XML Download