

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Lung cancer is the leading cause of cancer-related death in men and women worldwide, including Korea.12 Only 18% of all patients with lung cancer are alive for 5 or more years after diagnosis.2 Lung cancers are largely classified into non-small cell lung cancer (NSCLC) and small cell lung cancer, with NSCLC accounting for about 80% of all cases. Early diagnosis is important to reduce lung cancer mortality. Recently, low-dose computer tomography (LDCT) has been introduced for early diagnosis of lung cancer.3 However, in addition to LDCT, we can use various methods to detect lung cancer, and using blood samples is one of the easiest and convenient methods.45
A variety of research techniques have been introduced to help understand the complex biology of lung cancer development, including microarrays, which have been used extensively to examine differential gene expression profiles in many cancers.6 More recently, next-generation sequencing techniques have been developed and have come into wide use for the large-scale genetic profiling of diverse types of cancers.7
In our previous report, we used next-generation RNA-sequencing (RNA-Seq) to compare the transcriptomes of human NSCLC tissues with those of the neighboring normal lung tissues using lung tissue specimens from cigarette smokers with NSCLC.8910 We found that cellular retinoic acid binding protein 2 (CRABP2) messenger RNA (mRNA) levels were significantly higher in cancer tissues than in neighboring normal lung tissues, and that expression of CRABP2 was detectable by immunohistochemistry in the cancer cells, but not in the normal lung cells.8 CRABP2 has been shown to facilitate the binding of retinoic acid to its cognate receptor complex, but its role in carcinogenesis is not known.1112
Here, we have measured CRABP2 protein levels in stored blood samples from NSCLC patients and matched controls and have attempted to clarify the clinical implications of plasma CRABP2 levels in patients with NSCLC.
METHODS
Study subjects and sample collection
Stored plasma from patients who were diagnosed with NSCLC between September 2009 and September 2013 was employed in this study. The NSCLC was pathologically proven. Blood samples were collected at the time of diagnosis and prior to initiation of any treatment. The samples were separated by centrifugation at 2,500 rpm for 20 minutes, and the plasma was stored at −80°C in the Biobank of the Kangwon National University Hospital (Chuncheon, Korea). Plasma from matched controls was selected from the Korea Biobank Network (Cheongju, Korea). The controls were matched 1:1 with the patients for age (± 5 years), sex, and duration of lifetime cigarette smoking (± 10 pack-years [PY]). The controls did not have any known malignancies or chronic pulmonary diseases. Clinical data for the NSCLC patients and the controls, including tumor histology, disease stage, co-morbidities, and overall survival time, were also collected.
Measurement of CRABP2 levels in the plasma samples
We measured CRABP2 levels in the plasma using commercially available enzyme-linked immunosorbent assay (ELISA) kits with specific monoclonal antibodies against CRABP2 (USCN Life Science Inc., Wuhan, China) in accordance with the manufacturer's instructions.12 In brief, we prepared serial dilutions of the standard from 20 ng/mL to 0 (0, 0.312, 0.625, 1.25, 2.5, 5, 10, and 20 ng/mL) in 10 mM phosphate-buffered saline. A volume of 100 μL of standard or sample was added to each well, and the plate was incubated at 37°C for 2 hours. After removing the liquid, we added 100 μL of detection reagent-A working solution to each well and incubated at 37°C for another 2 hours. We again emptied and washed the wells 3 times with 350 μL washing buffer, and then added 100 μL of detection reagent-B working solution and incubated at 37°C for 30 minutes. After emptying and washing 5 times with 350 μL buffer, we added 90 μL of substrate solution to each well and incubated the samples at 37°C for 15 to 25 minutes, shielded from light, for color development. We measured optical density (OD) at 405 nm using an ELISA plate reader. The OD values were converted to ng/mL using a standard curve generated for the standard substance reconstituted with sample diluent. All samples were tested in duplicate.
Statistical methods
Plasma levels of CRABP2 were compared between groups by t-test and analysis of variance (ANOVA). The χ2 test was used for evaluation of differences between groups. A receiver operating characteristic (ROC) curve was drawn to determine a threshold value of CRABP2 for differentiating NSCLC samples from controls. Survival analysis was performed using Kaplan-Meier methods, and survival rates were compared by log-rank or other comparison tests. Univariate and multivariate analyses based on the Cox proportional hazard model were performed to identify significant independent prognostic factors for NSCLC patients. All statistical analyses were conducted using the SPSS statistical package version 24.0 (SPSS Inc., Chicago, IL, USA). P < 0.05 indicated statistical significance.
RESULTS
Patient characteristics
Plasma specimens from a total of 122 patients with NSCLC and the same number of matched controls were examined in this study. The mean age of the NSCLC patients was 71.8 years, and the median duration of cigarette smoking was 34 PY (range, 0–150 PY). Male patients predominated (77.9%, 95 patients) in both groups. There were no significant differences between NSCLC patients and controls with regard to age, sex, or PY (Table 1). Patients in the control group had a higher rate of cerebrovascular accidents and those in the NSCLC group had a higher prevalence of concomitant chronic airway disease. The majority of NSCLC patients had advanced stage disease.
Table 1
Baseline characteristics of patients with NSCLC and control

Data are presented as means ± standard deviation (range) or number (%).
NSCLC = non-small cell lung cancer, PY = pack-years, TNM = tumor, node, metastasis, NS = non-specific.
![]()
Plasma levels of CRABP2
Plasma CRABP2 levels were significantly higher in samples from patients with NSCLC than those from the matched controls (mean level 37.63 ± 28.71 ng/mL vs. 24.09 ± 21.09 ng/mL, P < 0.001; Fig. 1). The difference remained significant after correction for cerebrovascular accidents and chronic airway disease using the general linear model (P = 0.001).
 | Fig. 1Plasma CRABP2 levels in specimens from NSCLC patients and controls. The boxes indicate the mean levels of CRABP2 in each groups. The upper and lower horizontal bar indicate the standard deviation. Plasma CRABP2 levels were significantly higher in patients with NSCLC than in the control group. This difference was consistent after correction for cerebrovascular accidents and chronic airway disease (P = 0.001). The upper and lower horizontal bars indicate the standard error.CRABP2 = cellular retinoic acid binding protein 2, NSCLC = non-small cell lung cancer.
|
A ROC curve was drawn to determine a threshold value for plasma CRABP2 levels in to differentiate NSCLC patients from controls (Fig. 2). The area under the curve (AUC) was 0.705, and the sensitivity and specificity of the plasma CRABP2 level for NSCLC were 70.5% and 66.4%, respectively, at a cut-off value of 24.0 ng/mL.
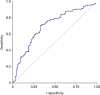 | Fig. 2ROC curve for plasma CRABP2 in NSCLC. AUC was 0.705 (94% confidence interval, 0.640–0.771). Sensitivity and specificity for NSCLC were 70.5% and 66.4% at a cut-off value of 24.0 ng/mL.ROC = receiver operator characteristic, CRABP2 = cellular retinoic acid binding protein 2, NSCLC = non-small cell lung cancer, AUC = area under the curve.
|
The plasma CRABP2 levels did not show any significant difference according to tumor, node, metastasis (TNM) stage, but the value tended to increase as the TNM stage increased (stage I: 23.1 ± 10.5 ng/mL; stage II: 35.8 ± 19.8 ng/mL; stage III: 35.6 ± 20.4 ng/mL; and stage IV: 40.3 ± 32.7 ng/mL; Table 2). There was no difference in plasma CRABP2 level according to the duration of lifetime smoking (PY) or histologic types (adenocarcinoma vs. squamous cell carcinoma) within the NSCLC patient group (Table 2).
Table 2
Plasma CRABP2 levels by subgroups in patients with NSCLC
Data are presented as means ± standard deviation.
CRABP2 = cellular retinoic acid binding protein 2, NSCLC = non-small cell lung cancer.
aP values were calculated by analysis of variance.
![]()
Survival analysis according to plasma CRABP2 levels in NSCLC patients
To identify whether high plasma levels of CRABP2 could be an independent prognostic marker for overall survival in patients with NSCLC, we performed univariate and multivariate analysis using Cox proportional hazard model. The multivariate analysis showed that poor overall survival in NSCLC was associated with old age (P = 0.008), large tumor size (P = 0.001), stage IV disease (P < 0.001), no treatment (P = 0.004) and higher plasma CRABP2 level (P = 0.050, Table 3).
Table 3
Univariate and multivariate analyses of overall survival in patients with NSCLC

NSCLC = non-small cell lung cancer, HR = hazard ratio, CI = confidence interval, CRABP2 = cellular retinoic acid binding protein 2.
aP values were calculated by Cox proportional hazard regression model.
![]()
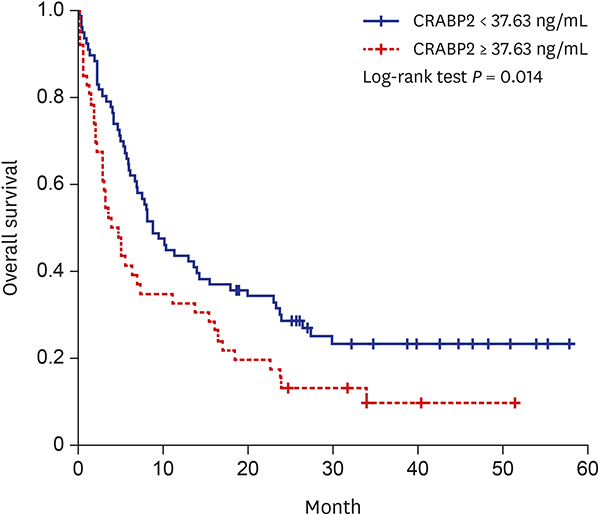
The median overall survival of the entire NSCLC group was 7.0 months (95% confidence interval, 4.8–9.2 months). We divided the NSCLC patients into two groups according to the mean value of the plasma CRABP2 levels (37.63 ng/mL) and found that plasma levels greater than this value were correlated with a poorer overall survival rate (P = 0.014, Fig. 3).
 | Fig. 3Kaplan-Meier survival curves. Overall survival according to plasma CRABP2 levels in NSCLC patients. The higher plasma CRABP2 levels were associated with lower overall survival rate among patients with NSCLC.CRABP2 = cellular retinoic acid binding protein 2, NSCLC = non-small cell lung cancer.
|
DISCUSSION
In this study, we found that the plasma CRABP2 levels in NSCLC patients was significantly increased compared with matched controls, and higher plasma CRABP2 level was associated poor overall survival in multivariate analysis.
CRABP2 is an intracellular lipid-binding protein that associates with retinoic acid and is thought to modulate retinoic acid signaling in the cell.12 Two isoforms (CRABP1 and CRABP2) have been identified, both of which have a high affinity for the ligand all-trans retinoic acid. These isoforms display 74% sequence identity in humans and are highly conserved among species. CRABP1 is expressed ubiquitously in adults, while CRABP2 is expressed only in the skin, uterus, ovary, and choroid plexus.11 The biological functions of the CRABP proteins are not completely understood. In mouse knockout studies, disruption of either CRABP isoform was associated with mild defects in limb development.13 CRABP1 has been found to act as a passive vehicle that binds and releases its ligand according to concentration gradients, while CRABP2 is known to deliver retinoic acid to the retinoic acid receptor (RAR), and the channeling of retinoic acid between CRABP2 and RAR results in a significant upregulation of holo-RAR formation and RAR transcription.12131415 CRABP2 overexpression in MCF-7 mammary carcinoma cells was associated with markedly enhanced sensitivity to retinoic acid-induced growth inhibition.13 Conversely, loss of CRABP2 expression has been correlated with resistance to retinoic acid-induced growth arrest in mammary carcinoma cell lines.16 Hence, CRABP2 expression appears to play a role in sensitizing cells to retinoic acid. Recently, a retinoic acid-independent anti-tumorigenic mechanism of CRABP2 was also proposed.17 The anti-carcinogenic action of the CRABP2 protein has been implied in other tumors, including astrocytomas18 and head and neck tumors.19
CRABP2 enhancement of retinoic acid signaling has generally been regarded as an anti-tumorigenic activity. However, there are contradictory reports, and the exact role of CRABP2 in general tumorigenesis requires further investigation. A recent proteomic analysis identified a high level of CRABP2 as a poor prognostic marker in estrogen receptor-negative breast tumors,20 and another study has identified CRABP2 as a subtype-specific biomarker of ovarian cancer.21 The authors of that study noted that CRABP2 was upregulated in serous ovarian carcinoma specimens and that CRABP2 expression was positively correlated with tumor grade and cancer stage. Significantly higher levels of CRABP2 mRNA have been observed in retinoblastoma tissues when compared with normal retinal tissues, and invasive retinoblastomas showed significantly higher levels of CRABP2 protein.22 Finally, CRABP2 was expressed at significantly higher levels in neuroblastoma with MycN amplification when compared with non-amplified-MycN neuroblastomas, and CRABP2 was identified as a novel target of the MycN oncogene.23 CRABP2 has also been found to be highly and specifically expressed in pancreatic ductal adenocarcinoma tissues, and it is more commonly expressed in high-grade precursor cancerous lesions than in low-grade lesions.24 As a possible explanation for these seemingly contradictory results, it has been noted that CRABP2 mediates proliferative activity through retinoic acid-induced peroxisome proliferator-activated receptor β/δ activation, not RAR, in the presence of another factor, fatty acid binding protein 5.25
To date, there have been only a very few studies of CRABP2 in NSCLC. One recent report found that CRABP2 mRNA levels as assessed by real-time polymerase chain reaction were elevated in 56% of 48 lung cancer specimens compared with adjacent normal tissue samples, and CRABP2 protein expression was also detected in 56% of tumor samples in that study.26 In addition, RNA-Seq in cancer tissue of NSCLC showed a 4.9-fold increase compared with normal lung tissue, and 72.1% of NSCLC samples showed expression of CRABP2 by immunohistochemistry.8
The results of our present study have shown for the first time that plasma levels of CRABP2 protein are significantly higher in plasma samples from NSCLC patients than in those from matched controls, and our ROC analysis suggested that plasma CRABP2 levels can be used as a diagnostic marker in patients with NSCLC. As described above, at a cut-off value of 24.0 ng/mL (the mean value of control samples), the sensitivity and specificity of CRABP2 in the NSCLC diagnosis were 70.5% and 66.4%, respectively, in this cohort. Thus, if validated in a future study, evaluation of plasma CRABP2 level may prove to be a convenient diagnostic assay for NSCLC, specifically adenocarcinoma or squamous cell carcinoma, as we did not identify any difference in plasma CRABP2 levels between these two histological types. Plasma CRABP2 levels also did not seem to be affected by the smoking status (PY).
This study has some limitations. We selected the control group not from a healthy population but from age- and sex-matched patients who had other diseases, excluding respiratory disease. In particular, patients in the control group had more cerebrovascular disease than did those in the NSCLC group. It is very difficult to find healthy subjects with no underlying disease who can be age- and sex-matched. Although we found a control group through the Korea Biobank Network, we were eventually forced to accept a difference in underlying diseases. Nevertheless, even after adjustment for difference values, the CRABP2 values were significantly different in the two groups. The second limitation is that most patients included in the study had stage IV disease (65.6%). The mean plasma CRABP2 level of patients in stage I was 23.1 ng/mL, indicating no difference between the control group and stage I patients. Therefore, CRABP2 may be limited as a marker for early lung cancer. However, the CRABP2 level was significantly increased in stage II patients compared with the control patients, and increased CRABP2 still reflected poor prognosis in the multivariate analysis. These findings suggest that CRABP2 is a useful biomarker for NSCLC.
As mentioned earlier, plasma CRABP2 levels tended to increase with increasing TNM stage. In the final multivariate analysis, we found that higher levels of plasma CRABP2 were associated with poor prognosis independently in NSCLC patients. As is the case with other tumor types,2125 the plasma CRABP2 level in cases of NSCLC may be an indicator of the biological aggressiveness of the tumor or it may simply be a reflection of the tumor burden.
In conclusion, our results are promising regarding the feasibility and utility of plasma CRABP2 as a novel diagnostic and prognostic marker in NSCLC, and the findings warrant further investigation.
 XML Download
XML Download