

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Workers must adapt to rapidly changing working conditions and psychosocial factors in the labor market. Thus, appropriate and comprehensive approaches are needed to address job stress-related issues in the workplace. In addition, psychosocial factors (including job stress and mental health) have been important issues in the field of occupational health, especially in developed countries. In this context, researchers, management, health providers, trade unions, and policy makers were interested in productivity, sustainable employment, and the burden of social change. Furthermore, there was increasing evidence that job stress was significantly associated with mental disorders,123 coronary heart disease,45 stroke,6 diabetes mellitus,7 hypertension,89 and musculoskeletal disorders.10 Therefore, it is important to measure accurately the job stress-related burden of disease (BOD), in order to efficiently allocate limited resources and facilitate rational decision-making to promote workers' health.
The World Health Organization (WHO) and the Global Burden of Disease (GBD) study suggested that death and disability-adjusted life years (DALY) was a useful metric for quantifying BOD. DALY is defined as the sum of years of life lost (YLL: burden due to death) and years lived with a disability (YLD: burden due to disability). Another metric for quantifying the effect of job stress on BOD is the population attributable fraction (PAF). PAF or BOD for specific causes were rare in Korea but it is worthwhile to estimate the social impact or to decide policy priority. Thus, the job stress-attributable BOD can be calculated by multiplying DALY and PAF.1112
Psychiatric disorders account for a large part of the global BOD, and the WHO has predicted that unipolar depressive disorder will become the leading cause of global BOD by 2030 (6.2% of the total DALY, up from 4.3% in 2004).13 In addition, for several years during the 21st century, Korea has ranked highest in suicide rate among the members of the Organization for Economic Co-operation and Development.14 Thus, Korean companies became increasingly interested in the mental health of their workers. Furthermore, the Samsung Economic Research Institute reported that the number of mental illnesses patients increased by 50% from 1.58 million people in 2004 to 2.31 million people in 2010. Moreover, the estimated socioeconomic cost of mental illness in 2010 was approximately 23 trillion KRW (approximately 19 billion USD), which corresponds to approximately 2.01% of the Korean gross domestic product (GDP) in 2010. The indirect cost of lost productivity was estimated to be approximately 20 trillion KRW. This significant economic burden highlights the importance of job stress-related mental health issues (e.g., psychiatric disorders and suicide).15
Previous studies have revealed relatively consistent associations between job stress and several cardiovascular diseases, which were listed as occupational diseases in the Enforcement Decree of the Korean Industrial Accident Compensation Insurance Act. These cardiovascular diseases include intracerebral hemorrhage, subarachnoid hemorrhage, cerebral infarction, myocardial infarction, and dissecting aortic aneurysm with work-related causes (including psychological strain), rather than natural disease progression.16 Cardiovascular diseases and cerebrovascular diseases were the second and third leading causes of death in Korea, which suggests that these diseases are important targets when estimating the BOD from job stress in Korea. Interestingly, a French study from 2003 revealed that the attributable fractions of job stress were 25% for cardiovascular disease, 34% for anxiety and depression, and 27% for musculoskeletal disorders.1718
The present study aimed to evaluate the role of job stress in disease development by estimating PAF for job stress in selected health outcomes and job stress related DALY in Korea.
METHODS
Health outcomes
We selected health outcomes as target diseases, which were defined by the following conditions: 1) the relative risk (RR) available (for calculating PAF) by reviewing literature, 2) disease prevalences available or calculable based on representative data, and 3) health outcomes with high priority with respect to the Korean occupational backgrounds and policy making; diseases that were the leading cause of death or were increasing in incidence would be eligible for this condition. Finally, the present study considered ischemic heart disease (IHD), stroke, major depressive disorder (MDD), and suicide as the health outcomes from job stress.
PAF
PAF was calculated using the following formula, as suggested by Levin and used in many previous studies1920:
In this equation, P denotes the proportion of workers who were exposed to job stress and RR denotes the RR of job stress related diseases.
The PAFs for ischemic stroke and hemorrhagic stroke were calculated using their respective RRs, and the total PAF for stroke was calculated by adding the PAF values for ischemic and hemorrhagic strokes.
The Korean National Police Agency has reported that approximately 4% of suicides were related to work- or workplace-related issues.21 Thus, we used this value to estimate PAF because no other studies have reported RRs or PAFs for job stress-related suicide in Korea.
Proportions of workers exposed to job stress
Based on Karasek's job strain model, high job strain occurs “when job demands are high and job decision latitude is low.”22 Approximately 21.2% of Korean workers were estimated to have high job strain exposure, based on the 2006 Korean Working Conditions Survey.23 The survey population represented active workers aged 15–65 years as the minimum age for employment in Korea was 15 years. The survey was conducted through face-to-face interviews using questionnaires, which was almost identical to the Fourth European Working Conditions Survey conducted in 2005.24 In that study, job strain was categorized into four levels (low, active, passive, and high strain groups) using the combination of job demands exposure and job control. Prior to 2011, the year for which we estimated the prevalence of the target diseases, the Korean Working Conditions Survey had been conducted twice (in 2006 and 2010). Thus, we used data from 2006, which included the results of the job strain exposure proportion.
RR
The RRs in the present study were obtained from studies of meta-analyses that we selected after reviewing the literature. We considered these studies appropriate for our purposes, as they reported recent advances in this field and used well-designed strategies. Kivimäki and Kawachi25 reported job strain-related RRs for incident coronary heart disease (1.33–1.44) in their review of 17 cohort studies since 2003. In addition, an RR of 1.34 (95% confidence interval [CI]: 1.18–1.51) was reported based on the IPD-Work Consortium data (10 unpublished studies, with previously published studies excluded).4 Moreover, job strain was associated with hazard ratios of 1.24 (95% CI, 1.05–1.46) for ischemic stroke and 1.01 (95% CI, 0.75–1.36) for hemorrhagic stroke.26
In their meta-analysis, Theorell et al.27 reported that job strain exposure was associated with a weighted odds ratio (OR) of 1.74 (95% CI, 1.53–1.96) for depression. However, Theorell et al.27 evaluated both diagnosed depression and depressive symptoms (a much milder state), and Jauregui and Schnall28 assumed that these depression outcomes could increase the duration of sickness or reduce workplace productivity and quality. As we agree with this approach, we believe that it was acceptable to use their OR which approximates RR based on the assumption that the disease prevalence was low in the population.29
DALY
The following formula was used to estimate YLD based on the burden of disability:
In this equation, P denotes the prevalence of disease and DW denotes the disability weight, which quantifies health levels that are associated with non-fatal outcomes. We initially considered the DW values that were suggested by the GBD study, although they need to be modified to be properly used in the present study. Thus, we used the average values if there were multiple DW choices available from the GBD study.30 For example, the GBD study classified the DW of MDD into 1) mild episodes = 0.145, 2) moderate episodes = 0.396, and 3) severe episodes = 0.658; thus, the final DW of MDD was defined as the average value (0.400). We used this method because we could not classify our prevalence data according to the disease classification approach used in the GBD study.
Disease prevalence was the preferred measure for calculating DALY, although it was difficult to directly calculate the prevalences in Korea because of the lack of available and representative data. Thus, we estimated the numbers of IHD and stroke cases based on 2011 claims data from the Health Insurance Review and Assessment Service.31 This estimation used the following parameters: 1) the health outcomes were matched only based on the code of the main diagnosis (excluding sub-diagnoses), 2) the health outcomes were defined as IHD (International Classification of Diseases-10 codes: I20–I25) and stroke (I60–I64), and 3) the claims were only submitted for inpatients. Based on these parameters, we calculated that there were 203,648 cases of IHD and 215,630 cases of stroke.
The MDD prevalence was estimated using data from the 2011 Korean Epidemiological Survey of Mental Disorders,32 which reported a 1-year prevalence of 3.1% for MDD among 18–74-year-old adults. Based on the mid-registration population during 2013 (the consensus standard), this prevalence corresponded to 1,271,312 MDD cases. As we assumed that the diseases' minimum latency periods were 0 years, we targeted individuals who were ≥ 15 years old (i.e., the minimum age of the economically active population). However, adults and children who were < 18 years old have different classification systems for mental illnesses and there were no data, that was why we only considered individuals who were 18–74 years old for the MDD calculations.
The following formula was used to estimate YLL based on the burden of death:
In this equation, N denotes the number of deaths and L denotes the life expectancy. For example, if a woman dies of stroke at the age of 50 years, the YLL for stroke would be 36, based on a life expectancy of 86 years for Korean women. N and L were estimated from the national cause-of-death statistics (N) and life table (L), which were published by Statistics Korea in 2013 (IHD: I20–I25, stroke: I60–I64, I67, and I69, suicide: X60–X84).33
RESULTS
Approximately 21.2% of Korean workers were exposed to high job strain. When we evaluated the effects of job strain, we found that it was attributable for approximately 6.7% of IHD cases, 6.9% of stroke cases (4.8% for ischemic stroke and 2.1% for hemorrhagic stroke), 13.6% of MDD cases, and 4% of suicides (Table 1). The estimated prevalences per 100,000 people were 473 for IHD, 501 for stroke, and 3,100 for MDD. The deaths per 100,000 people were estimated to be 32 for IHD, 59 for stroke, and 67 for suicide. The total DALY values per 100,000 people were estimated to be 563 for IHD, 1,048 for stroke, 1,240 for MDD, and 1,102 for suicide. The total BOD per 100,000 people in terms of job stress-attributable DALY were estimated to be 38 for IHD, 72 for stroke, 168 for MDD, and 44 for suicide (Table 2). The detailed data that were used to calculate these findings are shown in Table 3.
Table 1
Estimates of RR and PAF for selected stress-related health outcomes

| Health outcomes | RR (95% CI)a | PAF (%)b |
|---|---|---|
| IHD | 1.34 (1.18–1.52)4,25 | 6.72 |
| Stroke (ischemic) | 1.24 (1.05–1.46)25,29 | 4.84 |
| Stroke (hemorrhagic) | 1.01 (0.75–1.36)25,29 | 2.08 |
| Stroke (all) | - | 6.92 |
| MDD | 1.74 (1.53–1.96)1 | 13.60 |
| Suicide | - | 4.0025 |
PAF was calculated using the following formula: PAF = P × (RR – 1)/(1 + P × [RR – 1]), where P denotes the proportion of workers exposed to job stress (21.2% was used in the present study).
RR = relative risk, PAF = population attributable fraction, CI = confidence interval, IHD = ischemic heart disease, MDD = major depressive disorder.
aThis pooled RR value from prospective studies was obtained by comparing to employees free of job strain; bApproximately 21.2% of Korean workers were thought to have high job strain exposure, based on the 2006 Korean Working Conditions Survey.23
![]()
Table 2
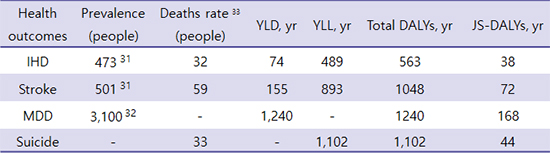
Prevalences, deaths, total DALYs, and JS-DALYs for selected health outcomes in 2013 (unit: per 100,000 people)

| Health outcomes | Prevalence (people) | Deaths rate33 (people) | YLD, yr | YLL, yr | Total DALYs, yr | JS-DALYs, yr |
|---|---|---|---|---|---|---|
| IHD | 47331 | 32 | 74 | 489 | 563 | 38 |
| Stroke | 50131 | 59 | 155 | 893 | 1,048 | 72 |
| MDD | 3,10032 | - | 1,240 | - | 1,240 | 168 |
| Suicide | - | 33 | - | 1,102 | 1,102 | 44 |
The mid-year registration population was used in 2013 (persons who were ≥ 15 years old [43,037,646 people] or were ≥ 18 years old and had major depressive disorders [41,010,081 people]). All values were reported per 100,000 people.
DALYs = disability-adjusted life years, JS-DALYs = job stress-attributable DALYs, IHD = ischemic heart disease, MDD = major depressive disorder, YLD = years lived with disability, prevalence × disability weight30, YLL = years of life lost, number of deaths × life expectancy33, Total DALYs = YLD + YLL, JS-DALYs = Total DALY × population attributable fraction (PAF).
![]()
Table 3
Age-specific data needed to calculate total DALYs for selected health outcomes

| Age, yr | Prevalence (people)31 | Death (people)32 | Life expectancy, yr32 | DW30 | YLD, yr | YLL, yr | Total DALYs, yr | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | Male | Female | Male | Female | Male | Female | |||
| IHD | ||||||||||||||
| 15–19 | 131 | 46 | 0 | 0 | 63.90 | 70.41 | 0.157 | 20.5 | 7.2 | 0.0 | 0.0 | 20.5 | 7.2 | |
| 20–24 | 238 | 138 | 2 | 0 | 58.99 | 65.46 | 0.157 | 37.4 | 21.7 | 118.0 | 0.0 | 155.4 | 21.7 | |
| 25–29 | 492 | 292 | 16 | 1 | 54.13 | 60.54 | 0.157 | 77.3 | 45.9 | 866.1 | 60.5 | 943.4 | 106.4 | |
| 30–34 | 946 | 377 | 28 | 4 | 49.29 | 55.64 | 0.157 | 148.5 | 59.2 | 1,380.1 | 222.6 | 1,528.7 | 281.7 | |
| 35–39 | 2,415 | 749 | 90 | 10 | 44.48 | 50.77 | 0.157 | 379.2 | 117.5 | 4,003.2 | 507.7 | 4,382.4 | 625.2 | |
| 40–44 | 4,354 | 1,923 | 175 | 21 | 39.73 | 45.92 | 0.157 | 683.5 | 301.9 | 6,952.8 | 964.3 | 7,636.3 | 1,266.2 | |
| 45–49 | 7,954 | 3,423 | 295 | 38 | 35.07 | 41.11 | 0.157 | 1,248.8 | 537.4 | 10,345.7 | 1,562.2 | 11,594.4 | 2,099.6 | |
| 50–54 | 12,939 | 7,308 | 528 | 65 | 30.57 | 36.34 | 0.157 | 2,031.3 | 1,147.3 | 16,141.0 | 2,362.1 | 18,172.3 | 3,509.4 | |
| 55–59 | 15,046 | 8,962 | 583 | 98 | 26.22 | 31.63 | 0.157 | 2,362.2 | 1,407.0 | 15,286.3 | 3,099.7 | 17,648.5 | 4,506.7 | |
| 60–64 | 16,246 | 10,869 | 590 | 159 | 22.03 | 26.96 | 0.157 | 2,550.7 | 1,706.4 | 12,997.7 | 4,286.6 | 15,548.4 | 5,993.1 | |
| 65–69 | 17,062 | 14,315 | 645 | 249 | 18.00 | 22.39 | 0.157 | 2,678.7 | 2,247.5 | 11,610.0 | 5,575.1 | 14,288.7 | 7,822.6 | |
| 70–74 | 15,393 | 17,561 | 1,029 | 677 | 14.19 | 17.98 | 0.157 | 2,416.6 | 2,757.1 | 14,601.5 | 12,172.5 | 17,018.1 | 14,929.6 | |
| 75–79 | 10,738 | 14,308 | 1,238 | 1,123 | 10.83 | 13.89 | 0.157 | 1,685.9 | 2,246.3 | 13,407.5 | 15,598.5 | 15,093.5 | 17,844.8 | |
| 80+ | 7,522.96 | 11,900 | 1,934 | 3,969 | 8.00 | 10.26 | 0.157 | 1,181.1 | 1,868.3 | 15,472.0 | 40,721.9 | 16,653.1 | 42,590.2 | |
| Total | 111,477 | 92,171 | 7,153 | 6,414 | - | - | - | 17,502 | 14,471 | 123,182 | 87,134 | 140,684 | 101,605 | |
| Stroke | ||||||||||||||
| 15–19 | 115 | 38 | 9 | 1 | 63.90 | 70.41 | 0.309 | 35.7 | 11.9 | 575.1 | 70.4 | 610.8 | 82.3 | |
| 20–24 | 169 | 154 | 13 | 7 | 58.99 | 65.46 | 0.309 | 52.3 | 47.5 | 766.9 | 458.2 | 819.2 | 505.8 | |
| 25–29 | 423 | 292 | 20 | 10 | 54.13 | 60.54 | 0.309 | 130.7 | 90.3 | 1,082.6 | 605.4 | 1,213.3 | 695.7 | |
| 30–34 | 746 | 423 | 42 | 34 | 49.29 | 55.64 | 0.309 | 230.6 | 130.7 | 2,070.2 | 1,891.8 | 2,300.7 | 2,022.5 | |
| 35–39 | 1,508 | 785 | 102 | 43 | 44.48 | 50.77 | 0.309 | 465.9 | 242.4 | 4,537.0 | 2,183.1 | 5,002.8 | 2,425.6 | |
| 40–44 | 3,492 | 1,969 | 209 | 116 | 39.73 | 45.92 | 0.309 | 1,079.1 | 608.5 | 8,303.6 | 5,326.7 | 9,382.7 | 5,935.2 | |
| 45–49 | 5,908 | 3,408 | 386 | 170 | 35.07 | 41.11 | 0.309 | 1,825.5 | 1,053.0 | 13,537.0 | 6,988.7 | 15,362.5 | 8,041.7 | |
| 50–54 | 10,046 | 5,777 | 590 | 300 | 30.57 | 36.34 | 0.309 | 3,104.3 | 1,785.1 | 18,036.3 | 10,902.0 | 21,140.6 | 12,687.1 | |
| 55–59 | 11,562 | 7,177 | 690 | 279 | 26.22 | 31.63 | 0.309 | 3,572.5 | 2,217.7 | 18,091.8 | 8,824.8 | 21,664.3 | 11,042.4 | |
| 60–64 | 13,315 | 8,669 | 801 | 320 | 22.03 | 26.96 | 0.309 | 4,114.5 | 2,678.8 | 17,646.0 | 8,627.2 | 21,760.5 | 11,306.0 | |
| 65–69 | 15,862 | 13,000 | 1,072 | 547 | 18.00 | 22.39 | 0.309 | 4,901.3 | 4,016.9 | 19,296.0 | 12,247.3 | 24,197.3 | 16,264.3 | |
| 70–74 | 17,308 | 19,977 | 1,963 | 1,398 | 14.19 | 17.98 | 0.309 | 5,348.1 | 6,172.8 | 27,855.0 | 25,136.0 | 33,203.1 | 31,308.8 | |
| 75–79 | 14,415 | 20,931 | 2,486 | 2,459 | 10.83 | 13.89 | 0.309 | 4,454.3 | 6,467.6 | 26,923.4 | 34,155.5 | 31,377.7 | 40,623.1 | |
| 80+ | 12,708 | 25,454 | 3,706 | 7,658 | 8.00 | 10.26 | 0.309 | 3,926.6 | 7,865.2 | 29,648.0 | 78,571.1 | 33,574.6 | 86,436.3 | |
| Total | 107,577 | 108,053 | 12,089 | 13,342 | - | - | - | 33,241 | 33,388 | 188,369 | 195,988 | 221,610 | 229,377 | |
| MDD | ||||||||||||||
| Total | 1,271,312 | - | - | - | 0.400 | 508,525 | - | - | 508,525 | |||||
| Suicide | ||||||||||||||
| 15–19 | - | - | 165 | 106 | 63.90 | 70.41 | - | - | - | 10,543.5 | 7,463.5 | 10,543.5 | 7,463.5 | |
| 20–24 | - | - | 308 | 177 | 58.99 | 65.46 | - | - | - | 18,168.9 | 11,586.4 | 18,168.9 | 11,586.4 | |
| 25–29 | - | - | 412 | 287 | 54.13 | 60.54 | - | - | - | 22,301.6 | 17,375.0 | 22,301.6 | 17,375.0 | |
| 30–34 | - | - | 714 | 411 | 49.29 | 55.64 | - | - | - | 35,193.1 | 22,868.0 | 35,193.1 | 22,868.0 | |
| 35–39 | - | - | 775 | 375 | 44.48 | 50.77 | - | - | - | 34,472.0 | 19,038.8 | 34,472.0 | 19,038.8 | |
| 40–44 | - | - | 1,025 | 434 | 39.73 | 45.92 | - | - | - | 40,723.3 | 19,929.3 | 40,723.3 | 19,929.3 | |
| 45–49 | - | - | 1,076 | 332 | 35.07 | 41.11 | - | - | - | 37,735.3 | 13,648.5 | 37,735.3 | 13,648.5 | |
| 50–54 | - | - | 1,236 | 409 | 30.57 | 36.34 | - | - | - | 37,784.5 | 14,863.1 | 37,784.5 | 14,863.1 | |
| 55–59 | - | - | 1,030 | 288 | 26.22 | 31.63 | - | - | - | 27,006.6 | 9,109.4 | 27,006.6 | 9,109.4 | |
| 60–64 | - | - | 746 | 212 | 22.03 | 26.96 | - | - | - | 16,434.4 | 5,715.5 | 16,434.4 | 5,715.5 | |
| 65–69 | - | - | 608 | 202 | 18.00 | 22.39 | - | - | - | 10,944.0 | 4,522.8 | 10,944.0 | 4,522.8 | |
| 70–74 | - | - | 752 | 302 | 14.19 | 17.98 | - | - | - | 10,670.9 | 5,430.0 | 10,670.9 | 5,430.0 | |
| 75–79 | - | - | 638 | 312 | 10.83 | 13.89 | - | - | - | 6,909.5 | 4,333.7 | 6,909.5 | 4,333.7 | |
| 80+ | - | - | 553 | 504 | 8.00 | 10.26 | - | - | - | 4,424.0 | 5,171.0 | 4,424.0 | 5,171.0 | |
| Total | - | - | 10,038 | 4,351 | - | - | - | - | - | 313,312 | 161,055 | 313,312 | 161,055 | |
![]()
DISCUSSION
As a result of the present study, the PAFs (%) for IHD, ischemic stroke, hemorrhagic stroke, MDD, and suicide were estimated to be 6.72, 4.84, 2.08, 13.6, and 4.00, respectively. Also, job stress-attributable BODs were estimated to be 38 years per 100,000 people for IHD, 72 years per 100,000 people for stroke, 168 years per 100,000 people for MDD, and 44 years per 100,000 people for suicide.
Sultan-Taïeb et al.1718 reported that 8.8%–10.2% (men) and 0.2%–1.1% (women) of coronary heart disease morbidity and 15.2%–19.8% (men) and 14.3%–27.1% (women) of mental disorders (defined as clinical depression) were attributable to job strain in France. This French study was the only one that estimated the PAF of job strain. Similar to the present study, the French job stress exposure data were calculated using the Karasek model,22 which defines job strain as a combination of high psychological demands at work (i.e., task quantity and complexity, and time pressure) and low decision-making latitude (i.e., decision authority and skill discretion). However, direct comparison with the French results was difficult for some reasons: 1) Unlike the French study, we did not consider gender differences, 2) The prevalence of job strain exposure was different (19.6% for men and 28.2% for women came from the national survey conducted in France in 2003), and 3) We used the RR values given in the studies of a meta-analysis, while they derived RRs from their own systematic review.
The exposure prevalence of job strain among Korean workers was estimated to be 21.2%, based on data from a cross-sectional questionnaire survey of 7,856 Korean workers.23 As the PAF is very sensitive to changes in this value, care should be taken when selecting the data. We tried to reflect the Korean working environment and find the latest value at the same time; however, we had no choice but to select the result. This value would be representative, but there might be a gap with the current situation because it was from 2006. Several other studies have used different epidemiological data and reported similar findings: 19% among Finnish men and 23% among Finnish women,1934 18.6% among Australian men and 25.5% among Australian women,35 and 23.2% among the general French population (19.6% for men and 28.2% for women).36 Although we were unable to provide sex-specific Korean estimates, our data provide useful perspective regarding the Korean working environment.
In the present study, we estimated the prevalence of IHD and stroke using 2011 claims data from the Health Insurance Review and Assessment Service, and also estimated the MDD prevalence based on data from the Korean suicide prevention center. According to the 2011 Korea National Health and Nutrition Examination Survey report, the prevalence of physician-diagnosed disease were 2.4% for angina or myocardial infarction among > 30-year-old individuals, 3.8% for stroke among > 50-year-old individuals, and 4.5% for depression among > 30-year-old individuals.37 However, these values were noticeably different from our estimates: 0.6% for IHD among > 30-year-old individuals, 1.3% for stroke among > 50-year-old individuals, and 3.9% for MDD among > 30-year-old individuals. This result was dependent on the respondents' reports and did not cover detailed diagnosis that we would like to estimate. On the other hand, our results would be more relevant in that they contained detailed and accurate diagnoses, and especially for stroke, we analyzed the claims data entered by doctors, not survey data. However, since the health insurance data was for the general population rather than workers, strictly speaking, the estimates do not reflect the prevalence among workers. Thus, it is possible that the prevalence was overestimated. We could not estimate the accurate prevalence among Korean workers by analyzing the claims data from the Health Insurance Review and Assessment Service. Self-employed workers, who accounted for 23.1% of the economically active population in 201138 and laborers are classified as district subscribers, which means they could not be distinguished from the general population.
In the GBD report, Korea was included in a group of countries with DALY values of 600–1,200 per 100,000 person-years for stroke and 0–300 per 100,000 person-years for IHD.39 The present study estimated a relatively high DALY value for IHD, although the DALY value was similar for stroke. However, it was difficult to guess why the DALY for IHD in this study was high, because we could not figure out which data was used to estimate the DALYs. Similarly, Hong et al.40 have reported that the Korean DALY for ischemic stroke was 483 per 100,000 person-years. This result was obtained from using the incidence of ischemic stroke by analyzing the health insurance data of 2004. Unlike these studies, we used the prevalence, not the incidence that was commonly used in estimating BOD. It was also impossible to measure the portion of job stress-attributable BOD among the total DALY.
The assessment of job stress-related health effects should be performed based on an understanding of the specific working environments and situations in each country. However, there were limited Korean studies regarding this topic, which made it difficult to estimate job stress-related BOD using domestic data. Inevitably, the present study has several limitations that should be considered. First, we did not consider other diseases that are relevant to job strain, such as musculoskeletal disorders, because it was difficult to access prevalence data and reasonable RR values of many types of musculoskeletal disorders to calculate DALY. In addition, musculoskeletal disorders were excluded from the analysis because of possible reverse causation. Second, the data were not analyzed according to sex. However, it is reasonable to estimate the BOD with DALY as it is obtained by summation and there were no available study results to measure job stress exposure proportion by sex. Third, our result may be overestimated, and not accurately reflect the Korean working environment, as it was impossible to access data on prevalence or death rate targeting the Korean working population. Fourth, we replaced the RR with an OR for depression and with a hazard ratio for stroke. However, the prevalences of diseases were so low that the results obtained by using OR were not expected to make a large difference. Fifth, the proportion of workers exposed to job stress may not reflect the current working environment as there is a gap between the time of data collection and the present. Despite these limitations, the present study provides a useful perspective regarding the Korean working environment, and was designed to estimate the outcomes in a way that closely reflected this working environment. In particular, we tried to increase the validity of the calculated value by using representative data such as claim data from the Health Insurance Review and Assessment Service.
Despite several limitations due to data, the present study would be meaningful in that studies on PAF or BOD for specific causes were rare in Korea, and especially since studies on the calculation of BOD from job stress were also rare globally. However, in order to estimate the BOD more accurately, further studies would be necessary to: 1) Estimate the disease prevalence according to the employment type by using nationally representative data such as data of the National Health Insurance Service, 2) Calculate accurate RR values through a large-scale cohort study of workers, and 3) Evaluate the proportions of workers exposed to other job stressors including job strain.
BOD could be used to quantitatively estimate major health impacts and could be applied as the main outcome of public health policy, unlike other estimates of health impact such as mortality or morbidity. This is the first study to attempt to estimate the Korean BOD from job stress using the latest and best available data. As society becomes more concerned about suicides or deaths due to cerebrovascular disease in the working-age population in relation to burden at the workplace, estimating the BOD from job stress is essential in determining the priority of the national policy on prevention.
 XML Download
XML Download