

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Metabolic syndrome (MS) is defined as a cluster of cardiovascular disease (CVD) risk factors that typically include central obesity, elevated blood pressure (BP), impaired glucose metabolism, and dyslipidemia.1 Because obesity is a key component of the syndrome, the prevalence of MS in adults continues to rise as the prevalence of obesity has increased dramatically.2 MS is not only associated with an increased risk of type 2 diabetes but also with increased risk of CVD morbidity and mortality.345
The prevalence of MS is increasing worldwide and this increasing trend also has been observed in Asian countries. According to Korea National Health and Nutritional Examination Survey (KHANES) 1998–2007, the prevalence of MS in Korea has increased from 24.9% to 31.3%.6 In particular, the prevalence of MS at younger age has increased significantly during this period. Young adults with MS have higher risk of developing CVD and type 2 diabetes. Prevention and early intervention of MS among younger individuals will be very important to decrease morbidity and mortality of CVD, diabetes, and its complications.
Most Korean military service consists of young soldiers, recruited at the average age of early 20s. Regular physical trainings, restricted dietary patterns, and the army lifestyle may have a positive impact on the overall health status but there is paucity of data regarding the prevalence of MS in the Korean military. Understanding the prevalence of MS and risk factors among young soldiers would be very important, as it is required for most Korean males to serve in the military.
A corporal health-screening program (CHSP) has been implemented throughout the Korean military since 2012. CHSP includes a basic physical examination consisting of anthropometric measurements and blood sampling for routine chemistry. We had access to a health database of approximately 5,000 young soldiers during the study period, including waist circumference which is a good indicator for abdominal obesity, a well-known risk factor for insulin resistance, which further predisposes individuals to type 2 diabetes.
The objectives of this study were to: 1) estimate the prevalence of obesity, and MS, and investigate common components of MS among Korean military members, using the 2005 revised National Cholesterol Education Program Adult Treatment Panels III (NCEP-ATP III) criteria, as proposed by the American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement (AHA/NHLB),7 and 2) make a comparison with Korean young adults in the general population using KHANES data.
METHODS
Study population
We conducted a retrospective, cross-sectional study of 4,803 young military participants who underwent a CHSP at one division medical battalion in the Republic of Korea (ROK) armed forces between October 2013 and October 2014. A CHSP is required for all soldiers promoting to at least a rank of corporal in the ROK armed forces. We excluded 37 subjects who had missing data for any of the individual MS criteria necessary to diagnosis MS.
We also had access to data from the KHANES, a nation-wide, population-based, cross-sectional health survey conducted by the Korea Centers for Disease Control and Prevention. A stratified, multistage probability sampling design was used to produce representative data. We obtained a sample of 1,108 young adults with age between 19–29 years from the fifth KNHNES conducted in 2010–2013.
Measurements
The participants in the CHSP underwent a routine physical examination that included measurement of height, weight, BP, and overnight fasting blood sampling. Standard height was measured without shoes to the nearest 0.1 cm. Weight was determined without shoes, wearing light clothes. Waist circumference was measured midway between the lower limit of the rib cage and the iliac crest. BP was measured using a standard mercury sphygmomanometer after being seated for at least 5 minutes. Blood was sampled after 12 hours of fasting, and venous blood glucose, total cholesterol (TC), triglycerides (TGs), and high- and low-density lipoprotein cholesterol (HDL-C and LDL-C, respectively) were measured.
A questionnaire on lifestyle was conducted among participants and the questionnaire included the following: how many times have you performed strenuous activity for more than 10 minutes that caused you to breathe heavily during the past one week? For smoking status, participants were asked whether they were smoking at the time of survey interview (yes/no). A similar survey was extracted from KHANES to match with the questionnaire conducted during CHSP.
Definitions of MS and obesity
The revised NCEP-ATP III criteria was used to identify those individuals with MS7 and the following were considered risk factors for MS: 1) abdominal obesity ≥ 90 cm according to World Health Organization Asian specific cut off value,8 2) hypertriglyceridemia, defined as TG ≥ 150 mg/dL, or taking TG-lowering medication, 3) low HDL-C, defined as HDL-C < 40 mg/dL in men, 4) high BP, defined as systolic BP/diastolic BP ≥ 130/85 mmHg or taking antihypertensive medication, and 5) high fasting plasma glucose (FPG) ≥ 100 mg/dL or taking antidiabetic medication (insulin or oral agents).
Statistical analysis
Data was presented as means ± standard deviation and prevalence of obesity, MS, and all components of MS were provided in percent (%). The χ2 test was used for the comparison of prevalence of MS in each group, and two sample t-tests were used for the comparison of continuous variables. Multivariate logistic regression analysis was used to identify independent risk factors for development of MS, obesity and each components of MS. P < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS version 19.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Table 1 shows the baseline characteristics of the 4,803 military personnel compared with 1,108 civilians aged between 19–29 years old from KHANES. The mean age of military participants was 20.8 ± 1.1 years, which was lower than that of the civilian participants. Among anthropometric and laboratory measurements, mean body mass index (BMI), waist circumference, diastolic BP, and FPG values were lower in the military group than in the civilian group (all, P < 0.001). Regarding lifestyle factors, 54.3% of military participants were smokers and 18.5% of military participants were engaged in regular, vigorous physical activity.
Table 1
Comparison of basic characteristics between Korean military personnel and civilians
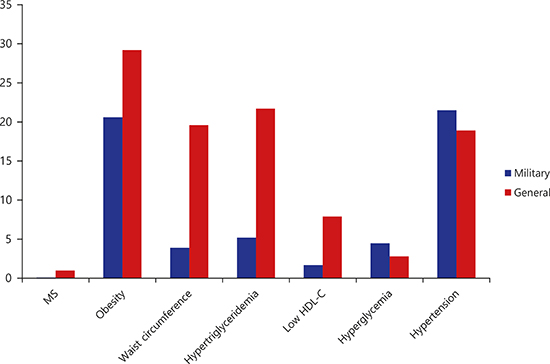
The prevalence of MS and obesity was much lower in the military group than in the civilian group (0.8% vs. 7.9% and 20.6% vs. 29.2%, MS and obesity, respectively; Table 2). Furthermore, those components to fulfill the diagnosis of MS were different between the two groups. Compared with civilian participants, military participants reported lower prevalence for most clinical variables such as BMI (20.6% vs. 29.2%), abdominal obesity (5.8% vs. 15.2%), hyperlipidemia (5.2% vs. 21.7%), high blood TG (3.9% vs. 19.6%) and hyperglycemia (1.7% vs. 7.9%). Conversely, higher prevalence of high BP was observed among military participants than civilians (21.5% vs. 18.2%).
Table 2
Prevalence of MS and each component abnormality between Korean military personnel and civilian men aged 19–29 years

Age older than 25 years was the most significant risk factor associated with development of MS and obesity in the civilian group (MS, odds ratio [OR], 3.17; 95% confidence interval [CI], 1.91–5.26 and obesity, OR, 1.61; 95% CI, 1.24–2.11) in multiple logistic analysis (Table 3). For the military group, the effect of age was not demonstrated as no participants were above 25 years. However, smoking lowered risk of obesity (OR, 0.81; 95% CI, 0.70–0.94), and high intensity physical activity showed protective effect against MS (OR, 0.19; 95% CI, 0.04–0.78) and obesity (OR, 0.81; 95% CI, 0.66–0.99) in the military group.
Table 3
Multiple logistic analysis of MS and obesity among Korean military personnel and civilian men aged 19–29 years

We also performed other analyses to further explore risk factors for each component of MS in both groups (Table 4). In the civilian group, age greater than 25 years old again was one of the strongest risk factors for development of most components of MS except low HDL-C level; abdominal obesity (OR, 1.77; 95% CI, 1.26–2.49), high BP (OR, 1.91; 95% CI, 1.39–2.63), hypertriglyceridemia (OR, 2.31; 95% CI, 1.68–3.19), and hyperglycemia (OR, 2.41; 95% CI, 1.49–3.86). Moreover, increased intensity of physical activities only showed the trend of lowering risk on each component of MS but did not meet statistical significance as only a small portion of civilians (8.8%) were engaged in regular physical activity. Conversely, higher intensity of physical activity showed protective effect on lowering of abdominal obesity (OR, 0.54; 95% CI, 0.37–0.79), high BP (OR, 0.79; 95% CI, 0.65–0.97) and hypertriglyceridemia (OR, 0.58; 95% CI, 0.37–0.91) in the military group. Interestingly, current smokers showed lower risk of having high BP in the military group.
Table 4
Multiple logistic analysis of the factors associated with MS among Korean military personnel and civilian men aged 19–29 years

Moreover, there were some differences among branches of the army in the military group. Compared with the infantry branch, the support branch appeared to have lower risk of high BP (OR, 0.76; 95% CI, 0.66–0.94) but higher risk of hypertriglyceridemia (OR, 1.46; 95% CI, 1.04–2.04).
DISCUSSION
In this study, we have identified the prevalence and risk factors for MS, obesity and its components in a large military group and compared it with the civilians of similar age. The overall baseline health status was better in the military group compared with the general population, except high BP. As expected with greater portion of military participants engaged in physical activities, the prevalence of MS and obesity was lower in the military group compared with civilians and physical activity attenuated risk of having abdominal obesity, high BP and hypertriglyceridemia in military group. As demonstrated in previous studies, smoking again showed the inverse association with obesity in the military group.91011 In the civilian group, age was the most important risk factor affecting the overall health status.
Previous studies have investigated the prevalence of obesity and MS in the military in other countries.121314151617181920 A similar tendency was observed in the comparison between US military and civilians. The prevalence of MS in military personnel was significantly lower than that of the general population.21 Soldiers tend to have higher BP and smoke more but have better lipid profile, fasting glucose and lower BMI than the general public.17 However, the prevalence of MS in military personnel in the current study was significantly lower than other studies.1213141820 The organization of the ROK armed forces is quite unique from armed forces in other countries. Korea has a mandatory draft system and most Korean men serve in the military in their early 20s. Therefore, participants in the current study are limited to young soldiers with mean age of 20.8 years old, which is significantly younger than military members of other countries.
Moreover, there are other factors contributing to low prevalence of MS in Korean military. When young Korean men are initially recruited, all of them undergo physical examinations and those individuals with underlying medical conditions including extreme BMI or high BP are either being exempt from military service or being placed in public service. Therefore, those military personnel included in the current study may have superior health status relative to the general population. However, this is not the decisive reason contributing to the health status of army members, because most of the men in Korea are recruited in the army and CHSP was performed for those who were about one-year post-recruitment. In addition, the military creates special circumstances where members are exposed to regular, high intensity physical activities. According to previous studies, military life and training had positive impact on overall health status.1920222324 Furthermore, this finding may imply that the prevalence of MS differs due to ethnic groups. In general, Asians have lower risk of obesity and MS than people from western countries although its prevalence in Asian countries continues to rise since the introduction of westernized diet.25
Our study analyzed the risk factors associated with MS, obesity and each component of MS in both groups using multiple logistic regression analysis. The prevalence of high BP among military members was higher than that of civilians. Stressful situations in the army may have contributed to development of high BP which was also demonstrated in previous studies.1217 Moreover, stress in the army was considered as a risk factor for newly reported hypertension after combat deployments in US army.2627 Similarly, high BP was more prevalent among active duty service soldiers in the current study. In the analysis of military branches, the infantry branch had higher risk of high BP than the artillery and armored groups. The infantry is considered to be the most active branch among the armed forces and this finding also reinforces the notion that stressful conditions may increase the risk of high BP. Therefore, proper stress management in the army will have positive effect on prevention and management of high BP. As expected, regular physical activity attenuated the risk of MS and obesity in the military group. This is in accord with previous studies where they also found that physical activity was effective in decreasing the risk of MS in both the military and general population.1214282930 However, physical activity did not demonstrate the positive impact against MS among civilians in this study and we think that this is because the civilian group may have been influenced by multiple factors that are beyond the scope of the current study, while the military group is under controlled circumstances where confounders may have minimal effect.
Although smoking is a well-known risk factor for high BP as well as MS, the prevalence of high BP in the current study was lower in smokers than non-smokers in the military group. This is contrary to previous findings where they showed smoking was a risk factor for hypertension and MS.313233 We thought BMI rather than smoking may have affected BP in young adults.34353637 It also reflects the fact that smokers have lower BMI.3839 Our study also supports this concept by the fact fewer obese soldiers were found in the smoking group. Interestingly, age older than 25 years was a key factor affecting the prevalence of obesity, MS, and each component of MS in civilians. This finding can be explained by the fact that the lifestyle of 20-year-old men varies greatly after 25 years of age. Many men tend to start their career with more sedentary lifestyle after 25 years of age and this change in their lifestyles may have significant impact on overall health status.
Our study has several strengths. First, this study included 4,803 military personnel to estimate the prevalence of MS, which is the largest study so far. Second, the baseline characteristics of the military were compared with general population of similar age, thus well demonstrating the effect of active duty in military. Third, we analyzed the risk factors of MS, obesity and each component of MS in both military and civilian groups.
The current study also has several limitations. First, this was a retrospective, cross-sectional study which may not demonstrate the direct causal effect. Second, the age distribution between the two groups was different, which might have affected the results of this study. While the age distribution in the military was concentrated in the early 20s, data from KHANES showed even distribution throughout ages 20–29 years. However, when we performed subgroup analysis, limiting to individuals under 25 years of age, we obtained similar results (data not shown). Third, the data were absent on other well-documented risk factors for MS and obesity, such as diet, family history or other medical conditions.
This study reported that the prevalence of MS and obesity in the Korean military are lower than civilians of the same age group. However, the prevalence of high BP and current smokers are higher in the military population, emphasizing the importance of proper stress management and/or preventative programs in the military. Future, prospective clinical studies which include variables related to lifestyle interventions such as physical activity and nutrition are needed in parallel to the assessment of MS and obesity in the military.
 XML Download
XML Download