

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The anatomy of the distal radius is complex. The columnar concept of the distal radius was proposed in 1996 by Dr. Rikli and Regazzoni to simplify the surgical planning of distal radius fractures by dividing the complex geometry of the distal radius into two columns with relatively simple geometry.1) In this conception, the lateral column includes the radial styloid and scaphoid fossa, while the intermediate column includes the lunate fossa and sigmoid notch. The application of two small dorsal plates, one to each column (in accordance with the columnar concept), provides improved outcomes over a single dorsal plate in terms of extensor-related complications.2)
The introduction of the innovative volar locking plate (VLP) in the late 1990s changed the landscape of the surgical treatment of distal radius fractures.3) The use of anatomical VLPs rapidly increased given its advantages over the dorsal counterpart, which include a simple anatomy in the volar distal radius and less tendon irritation because of a thicker soft tissue layer at the plate-tendon interface.4) Numerous studies have reported a fast recovery with good functional and radiographic outcomes after the stabilization of distal radius fractures with a VLP.5678) As VLPs are considered to be anatomically designed, the use of the VLP as a template for the reduction of displaced fracture fragments or the correction of the malunion of the distal radius is a widely employed technique among orthopedic surgeons.
However, several plate design related complications have been reported, such as suboptimal alignment following stabilization,910) with or without subsequent limited motion of the distal radioulnar joint,11) or flexor tendon ruptures.1213) Studies investigating the fit of anatomical VLPs have demonstrated an inadequate fit to the volar surface of the distal radius.1415) Recent anatomical studies employing Caucasian cadavers have demonstrated a significant angular difference between the lateral and intermediate columns, as well as between men and women.161718) It appears that the nonconformity of the plate to the distal radius is caused by inter-individual differences in the distal radius anatomy itself rather than the plate design. However, the degree of variability in the morphometry of the distal radius has not been studied. Understanding the morphometric variation in the distal radius may help surgeons avoid post-surgical complications related to the suboptimal alignment of the distal radius by encouraging surgeons to be prepared for a prompt modification of the anatomical plate during surgery and rely less on the plate design to achieve a patient-specific alignment of the distal radius. The purpose of this study was to evaluate the degree of variability in the morphometry of the distal radius and identify factors associated with the variability.
METHODS
An anatomical study was performed, investigating the morphometric characteristics of the volar surface of the distal radius in Korean cadavers. A total of 81 Korean cadaveric radii (right, 41; left, 40) from 38 male and 43 female cadavers, with a mean age of 55.3 years (range, 39 to 68 years), were analyzed. All the cadavers had provided written consent during their lifetime to donate their body for research and educational purposes. Radiographs of the wrist were taken before a computed tomography (CT) scan to exclude any bone diseases or fractures. Subsequently, CT images were obtained (176 slices with a slice thickness of 0.75 mm) using a dual-source multidetector CT system (Somatom definition AS+, Siemens Healthcare, Forchheim, Germany). The raw data (in Digital Imaging and Communication in Medicine format) were reconstructed to three-dimensional (3D) images using a 3D software program (MIMICS 13.1; Materialise, Leuven, Belgium) and were converted to stereolithography (STL) files. The STL files were imported into the 3D CAD program (Solid-Works 2013; Dassault Systemes, Waltham, MA, USA) and the volar surface angle (VSA) and volar surface width (VSW) of the distal radius were measured. We chose the VSA and VSW because they were most frequently measured variables in the previous anatomical studies.171819)
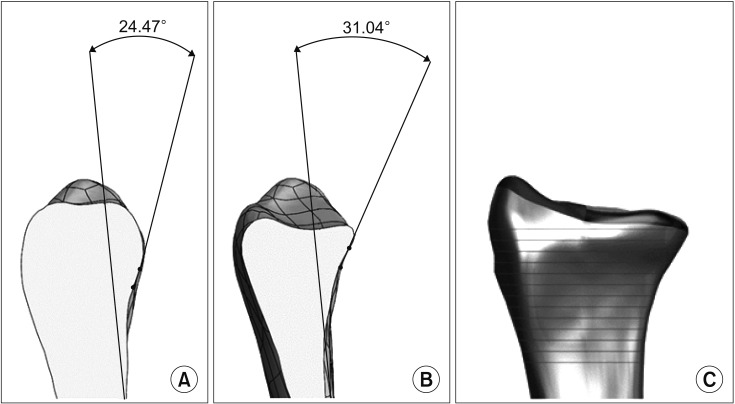
To measure the VSA, we defined the centers of the scaphoid and lunate fossa as the meeting point of three curved surfaces, consisting of the volar, dorsal, and lateral/medial articular surfaces of each fossa, respectively. Sagittal section images were then reconstructed along the planes crossing the center of each fossa, which were parallel to the central axis of the distal radius (Fig. 1A and B). The VSA at the lateral column (Fig. 1A) was defined as the angle between the line along the volar surface of the radial shaft and the line along the volar surface of the radial metaphysis in the sagittal reconstruction images at the center of the scaphoid fossa of the radius. The VSA at the intermediate column (Fig. 1B) was similarly measured at the center of the lunate fossa of the radius.1)
The VSW was defined as the length of a line drawn on the volar surface of the radius from the ulnar to the radial margin, perpendicular to the central axis of the distal radius. The VSW was measured from the watershed line to a point 20 mm proximal to the watershed line, in increments of 2 mm (Fig. 1C).
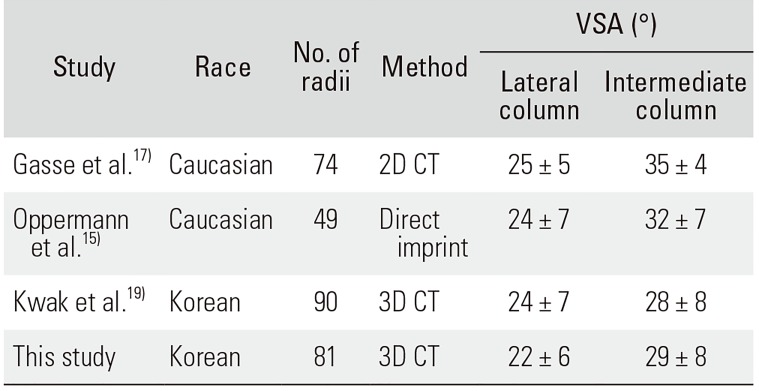
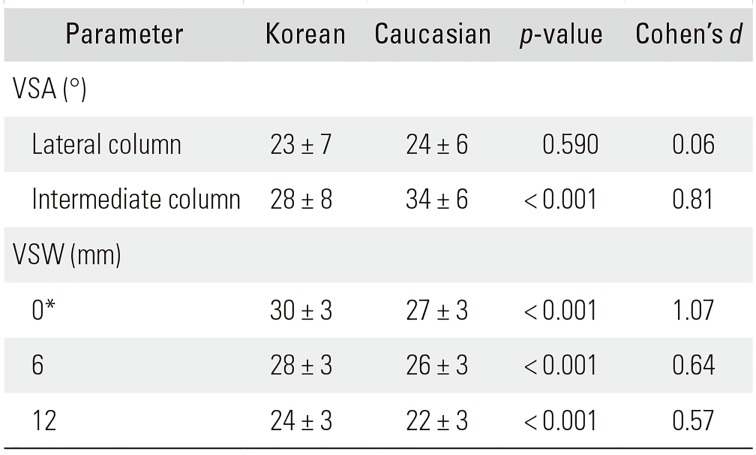
All measurements were conducted twice by one researcher (JHS) and were averaged. The morphometric data of Caucasian radii were pooled from two previous studies,1718) and those of Korean radii were pooled from the present study and one previous study (Table 1).19)
Statistical analyses were performed using IBM SPSS ver. 23.0 (IBM Corp., Armonk, NY, USA). Each morphometric variable was confirmed to follow a Gaussian distribution; thus, parametric tests were performed. Paired sample t-tests were used to evaluate differences between the lateral and intermediate columns. Student t-tests were used to evaluate differences between males and females and between Koreans and Caucasians. Pearson correlation coefficients were calculated to evaluate relationships between demographic and morphometric data. The level of significance was set at p < 0.05. The coefficient of variation (CV) was used to assess the variability in morphometric parameters. The CV is obtained by calculating the standard deviation as a percentage of the group mean; a CV of < 10% is classified as low, 10%–20% is classified as medium, 21%–30% is classified as high, and > 30% is classified as very high.20) Cohen's d, which is the difference between two means divided by the standard deviation, was used to estimate effect sizes; a Cohen's d of ≥ 0.2 is considered small, ≥ 0.5 is considered medium, and ≥ 0.8 is considered large.21)
We conducted this study in compliance with the principles of the Declaration of Helsinki. The protocol of this study was reviewed and approved by the Institutional Review Board of Hallym University Sacred Heart Hospital (IRB No. 2016-I144). The informed consent was waived because this was a cadaveric study.
RESULTS
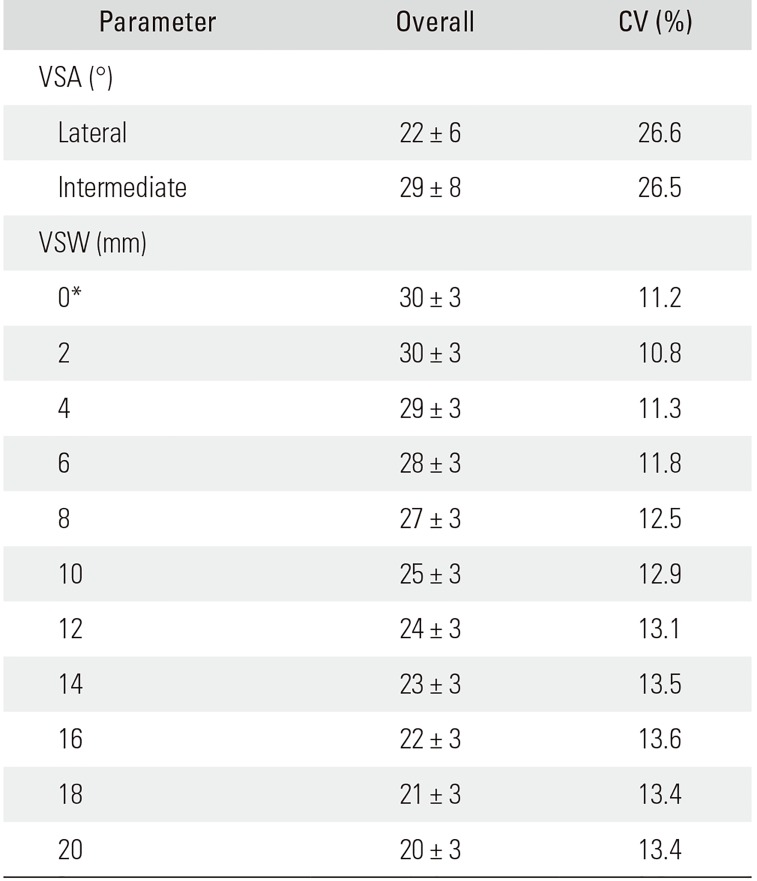
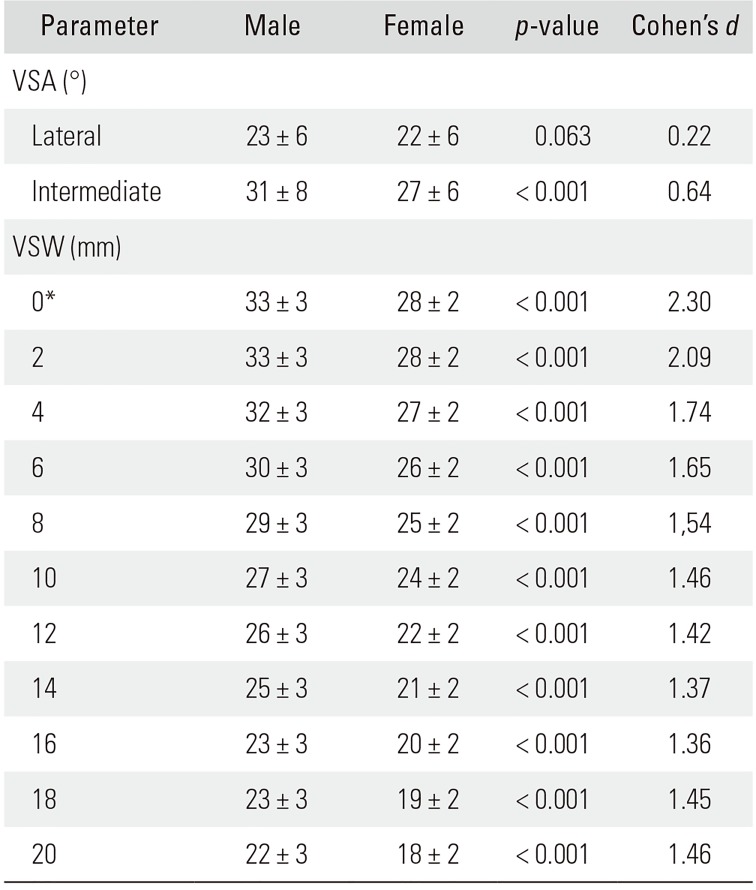
The VSA was significantly greater at the intermediate column than at the lateral column (29° ± 8° vs. 22° ± 6°, p < 0.001) (Table 2). Although males showed a significantly greater VSA than that in females at the intermediate column in Koreans (31° ± 8° vs. 27° ± 6°, p < 0.001) (Table 3), the sex difference was not significant for the VSA at the lateral column (p = 0.063). Caucasians had a significantly greater VSA than that in Koreans (34° ± 6° vs. 28° ± 8°, p < 0.001) (Table 4). The VSA showed high variability, as determined by the CV, and the differences in the VSA between columns and race were large, while the difference between the sexes was medium, as determined by the effect size.
The average VSW of the distal radius in Koreans was 30 ± 3 mm at the watershed line and became narrower proximally. The variability of the VSW was medium as determined by the CV (Table 2). Males had significantly larger VSWs than those in females (p < 0.001) (Table 3), and Koreans had significantly larger VSWs than those in Caucasians (p < 0.001) (Table 4). The differences in the VSW between sex and race were large and medium, respectively, as assessed by the effect size.
Age had a significant, but weak, negative correlation with the VSA at the intermediate column (r = −0.154, p = 0.041), but it did not correlate with the VSW (p > 0.05). Height was significantly correlated with the VSW (r = 0.576, p < 0.001), but it did not correlate with the VSA (p > 0.05).
DISCUSSION
The recently developed VLPs are considered to have an anatomical design and have been widely used to restore normal alignment following distal radius fractures or malunion. However, a significant discrepancy has been demonstrated between the plate design and the anatomy of the volar surface of the native distal radius.1415) This discrepancy may be attributable to morphometric variations in the volar aspect of the distal radius rather than the plate design. However, the variability in the morphometry of the distal radius is not well understood. In the current study, we demonstrated that the morphometry of the volar aspect of the distal radius has considerable variability, which is associated with column, sex, and race.
Previous studies found a poor fit of the anatomical VLPs to the volar surface of the distal radius. Buzzell et al.14) found that only 3%–6% of contact area existed between the volar surface and seven different types of volar fixed-angle plates when the plates were fixed in their best-fit position. Additionally, Oppermann et al.15) showed that a substantial gap (up to 4.8 mm) was present between the volar cortex of the distal radius and the VLPs when the plates were fixed proximally in their best-fit position. These discrepancies between the plate and distal radius can be explained by the large variability of the VSA demonstrated in the current study. For example, as the standard deviations of the VSA for the lateral and intermediate columns were 6° and 8°, the probability that an angle difference of at least 6° or 8° (which corresponds to a gap of approximately 2–3 mm between the plate and the native distal radius, assuming that the length was 2 cm for the portion of the plate distal to the volar angulation) occurs between the distal radius and the plate is estimated to be 31.8%. In other words, there can be malunion or significant plate protrusion-related complications in approximately one-third of cases, even when a perfect anatomical plate is used. A similar situation has been reported where the use of an anatomical VLP resulted in an excessive palmar tilt with a subsequent limitation of motion in the distal radioulnar joint.11) Therefore, our findings suggest that the multiple size options need to be available to effectively address the anatomical variations of the distal radius, or the plate alignment should be tailored to the patient's specific anatomy during surgery, even when anatomical VLPs are in use.
In the present study, the VSA at the intermediate column was significantly larger than that at the lateral column. This finding is consistent with that of prior studies, in which the VSA at the intermediate column was larger than that at the lateral column by an average of 3° to 10°.16171819) In addition, sex was found to be an important factor contributing to anatomical variation in the distal radius. Sex differences have been reported in previous studies as well; however, the pattern of the differences has been inconsistent. Oppermann et al.15) reported that only the VSA at the lateral column was significantly greater in males than in females, whereas Kwak et al.19) reported that the VSAs at the lateral and intermediate columns were larger in males than in females. In contrast, we found that only the VSA at the intermediate column was significantly greater in males than in females. This inconsistency may arise from heterogeneity in the study designs, racial differences, or type I errors; thus, further research is needed for clarification.
In the current study, we found that there were racial differences in the morphometry of the distal radius. Using the pooled data from three other studies and the present study, we found that Caucasians have a 6° greater VSA at the intermediate column than that in Koreans, which is a large difference. However, Koreans had a significantly greater width of the distal radius than that in Caucasians although the difference was only medium in size. Taken together, the results of the current study indicate that sex and race are significant factors contributing to variability in the anatomy of the distal radius, and these factors need to be considered in the preoperative planning and operating theater to achieve patient-specific alignment of the distal radius. For example, as the plate design is different across different manufacturers, a plate with more volar angulation may be a better choice for Caucasian patients.
The present study has several limitations. First, the mean age of the subjects was in the 50s; thus, the study population may not be representative of the broader Korean population. However, age did not substantially affect the anatomical variation of the distal radius in the present study; thus, aging does not appear to be a significant issue. Second, there could be other potential factors affecting the morphometric variations of the distal radius other than age, sex, or ethnicity. We could not analyze these factors because we could not obtain socioeconomic or medical data of the cadaveric donors. Third, the pooled data might differ from the population data within each race because of the heterogeneity of the study designs and the relatively small number of subjects. Fourth, although the morphometric variation of the volar distal radius was statistically significant and large, the clinical implications remain to be determined. Fifth, we could not provide any practical guidelines to effectively address the substantial morphometric variability in the volar surface of the distal radius. The most accurate method to predict a discrepancy between the plate and the distal radius may be probably to perform a CT scan of the contralateral normal wrist and measure the VSA and VSW. However, this postulation should be tested in the future study. Sixth, we could not find any study reporting on the morphometric variability in the other parts of the body in Koreans, and thus we could not judge whether the volar surface of the distal radius has a significantly different variability compared to the other parts of the body. However, even if the variation of the distal radius morphometry is within the range of natural variations of the body, this does not necessarily mean that the morphometric variation of the distal radius could not be a cause for discrepancy between the plate and the distal radius anatomy.
In conclusion, we found that considerable morphometric variation exists in the volar distal radius and that the factors of sex, race, and column significantly contribute to this variation. The presence of morphometric variation may be one of the causative factors for postoperative complications, such as over-reduction with a subsequent limitation of prosupination or flexor tendon rupture, following the use of anatomical VLPs. These results suggest that surgeons should carefully choose an anatomical VLP with appropriate angulation characteristics for each patient to achieve patient-specific alignment of the distal radius.
 XML Download
XML Download