

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Clavicular fractures are common injuries and account for approximately 15% of the upper extremity fractures and 5% of all fractures.1) Surgical fixation is recommended for displaced unstable clavicular fractures because the rates of delayed union or nonunion are high with conservative treatment.23) In particular, the plate fixation provides stabilization to the fracture and immediate pain relief among various surgical treatments; as a result, it enables early mobilization.45) Clavicular fractures mostly occur in young active males, and early return to activities is preferable in this population.6) Therefore, the indication for the internal fixation of clavicular fractures should be broadened.6) Several studies have reported satisfactory functional outcomes after plate fixation.46)
Appropriate pain control after shoulder surgery enhances postoperative rehabilitation, leading to early mobilization and functional recovery, including range of motion and muscle power.78) Therefore, aggressive pain management in the early postoperative period is a major issue for patients who undergo shoulder surgery.78) The supraclavicular nerve arises from the third and fourth cervical nerves and emerges beneath the posterior border of the sternocleidomastoid muscle.910) The supraclavicular nerve branches into the medial, intermediate, and lateral supraclavicular nerves at the sternocleidomastoid and descends into the posterior triangle of the neck beneath the platysma and deep cervical fascia.910) Recently, the selective supraclavicular nerve block is considered useful because clavicular fracture surgery without cervical plexus nerve block may lead to phrenic nerve paralysis.91011)
Opioids are still used to manage pain after orthopedic surgery.1213) However, opioids increase the risk of various adverse effects such as nausea and vomiting, pruritus, sedation, respiratory depression, and urinary retention.1213) To improve analgesia and reduce opioid-related side effects, a multimodal pain management has been introduced, which has been reported to improve functional recovery and shorten periods of hospitalization after orthopedic surgery.1214) In particular, surgical-site injections (SIs) after arthroplasty or arthroscopy have been reported to decrease postoperative pain effectively with low side-effect rates.121315)
Postoperative pain is known to affect the stress reaction after surgery; this stress reaction is characterized by increased pituitary hormones or other biomarker secretion, which has secondary effects on the hormone secretion of the target organs.1617) Several studies have reported significant differences in the levels of stress biomarkers, namely, dehydroepiandrosterone sulfate (DHEA-S),18) insulin,19) and fibrinogen20) between the patients with musculoskeletal pain and the patients without pain.
The objective of the present study was to assess the effect of a surgical-site, multimodal drug injection following plate fixation for clavicular fractures by evaluating the visual analogue scale (VAS) pain scores and objective pain-related stress biomarkers in the early postoperative period. Our hypothesis was that the injection-cohort would demonstrate better VAS pain score outcomes and changes in the levels of pain-related stress biomarkers in the early postoperative period.
METHODS
Participants
We conducted this study in compliance with the principles of the Declaration of Helsinki. The protocol of this study was reviewed and approved by the Institutional Review Board of Dankook University Hospital (IRB No. 2018-05-011), informed consent was obtained from 50 consecutive patients who underwent plating for the mid-shaft and distal clavicular fractures between May 2017 and April 2018. Skeletally mature patients with closed displaced mid-shaft clavicular fractures (Robinson type 2B) and Neer type-II distal clavicular fractures were included in the study.21) Patients with polytrauma, those with medial-third clavicular fractures, and those in whom intravenous patient-controlled analgesia (PCA) or oral medication was discontinued because of side effects were excluded from the study. To evaluate whether SIs have pain management benefits, the patients were randomly divided into two groups (SI and no-SI groups). The SI group patients were assessed first, and then the no-SI group patients.
Surgery Technique
All surgeries were performed by a single, experienced orthopedic surgeon (JSY). General anesthesia was used in all patients. In beach chair position, a transverse incision was made over the fracture site. The fracture site was exposed and reduced with the help of bone holding forceps. Subsequently, according to the pattern of the fracture, a 3.0-mm precontoured low contact plate (LCP), a superior lateral clavicle LCP, or a hook LCP (TDM, Seoul, Korea) was applied over the superior surface of the clavicle. An arm pouch was used for 6 weeks after surgery in all patients. Assisted passive mobilization was started 1 week after the surgery.
SI Group
The injection was evenly distributed between the deep and superficial soft tissues in an extra-articular pattern without injecting the drug into the synovium or capsule directly. It was distributed between the deep tissues (periosteum) and the superficial tissues (platysma, trapezius, pectoralis major, deltoid musculature, and subcutaneous plane) prior to wound closure. Careful attention was paid to avoid injecting the drug into the neurovascular bundles.
The mixture of anesthetics consisted of 1 ampule of epinephrine hydrochloride (HCL; 1 mg/mL, 1 mL/ampule), one ampule of morphine sulfate (5 mg/0.5 mL, 0.5 mL/ampule), two ampules of ropivacaine HCL (Naropin 0.75%, 7.5 mg/mL, 20 mL/ampule; Astrazeneca, London, UK), and normal saline 20 mL; thus, the total volume of anesthetic mixture was 61.5 mL.22) In this study, we injected 30 mL of the total 61.5 mL anesthetic mixture.
Outcome Measures
The primary outcome was the VAS pain score over the first 3 postoperative days. The patients were instructed to use a 10-cm VAS to describe their current level of comfort, with the end-points 0 corresponding to no pain and 10 corresponding to the most extreme possible pain. Pain assessments (using the means of all individual data points) were completed while the patients were at rest immediately prior to the surgical procedure in the post-anesthesia care unit, and at every 6 hours following the surgical procedure until the postoperative hour (POH) 72. The VAS pain scores were collected by the nursing staff in the inpatient ward.
After the operation, postoperative intravenous PCA for 24 hours (Fentanyl 0.2 mg/mL/kg, Ketorolac 0.02 mg/mL/kg, and Ramosetron 0.015 mg/mL at 1 mL/hr, a bolus dose of 1 mL, and at a lockout interval of 15 minutes) was used in all patients. Oral medications (Ultracet ER semi, Celebrex 200 mg, and pregabalin 75 mg) were also prescribed twice a day from the day after the surgery; the first dose of these medications was administered at 6 hours after the surgery. Moreover, if the patients wanted further pain control or had a VAS pain score of 7 points until POH 72, 75 mg of intravenous tramadol was administered, and the intravenous tramadol requirement was also recorded. We did not use other medications for pain management. Every patient was hospitalized for 3 days after the surgery. During the hospitalization, intravenous tramadol was used as a rescue drug whenever necessary.
To evaluate the stress biomarkers, blood sampling was conducted at 6:00 AM on the day of the surgery and at POH 24, 48, and 72.16) Plasma insulin levels were determined by electrochemiluminescence using an immunoanalyzer (GAMMA-10; Shin Jin Medics, Goyang, Korea) in our hospital laboratory. Plasma DHEA-S levels were measured by a γ-counter (GAMMA-10, Shin Jin Medics) using a DHEA-S RIA CT kit (Immunotech, Monrovia, CA, USA) in the Seoul Clinical Laboratories. Plasma fibrinogen levels were determined by an automated coagulation analyzer (ACL TOP 700; Instrumentation Laboratory, Werfen, Bedford, MA, USA) in our hospital laboratory. The levels of the pain-related stress biomarkers, namely, insulin, DHEA-S, and fibrinogen, were also recorded.16)
Statistical Analysis
The Student t-test was used to determine the significance of intergroup differences in the continuous variables; the Fisher exact or chi-square test was used to determine the differences in the categorical variables. Correlations between the pain-related biomarkers and the VAS pain scores were analyzed by Pearson correlation analysis. All the values are presented as means with standard deviations, and p-values of < 0.05 were considered statistically significant. The statistical analysis was performed with IBM SPSS ver. 22.0 (IBM Corp., Armonk, NY, USA).
Go to : 
RESULTS
Fifty patients were included as the study population, and 25 patients were included in each group. There was no significant difference between the two groups with respect to age, sex, body mass index, American Society of Anesthesiologists status, ratio of diabetes mellitus, preoperative VAS pain score, fracture site, fixation method, and time for surgery (Table 1). There was no local side effect (wound dehiscence, skin discoloration, and superficial or deep infection) after surgical-site, multimodal drug injection.
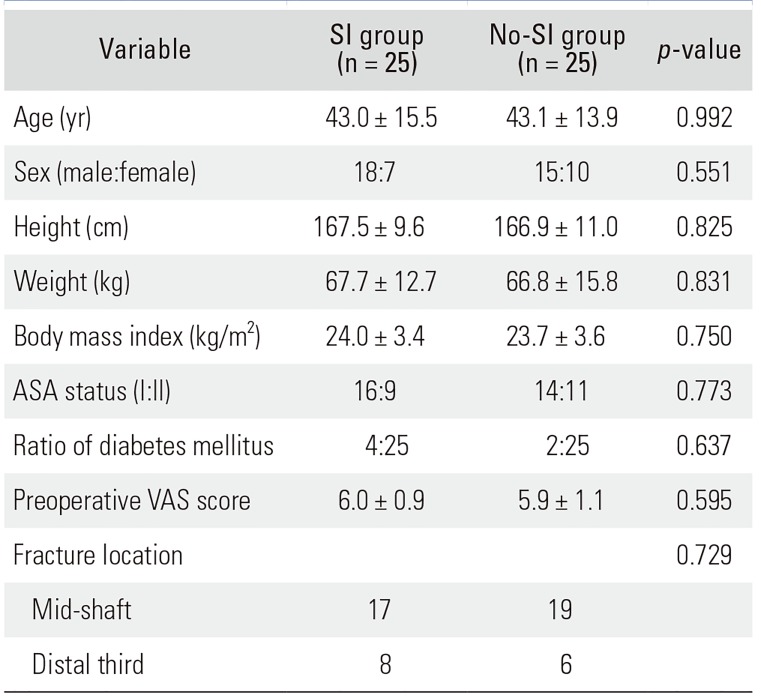
Table 1
Demographic Data
![]()
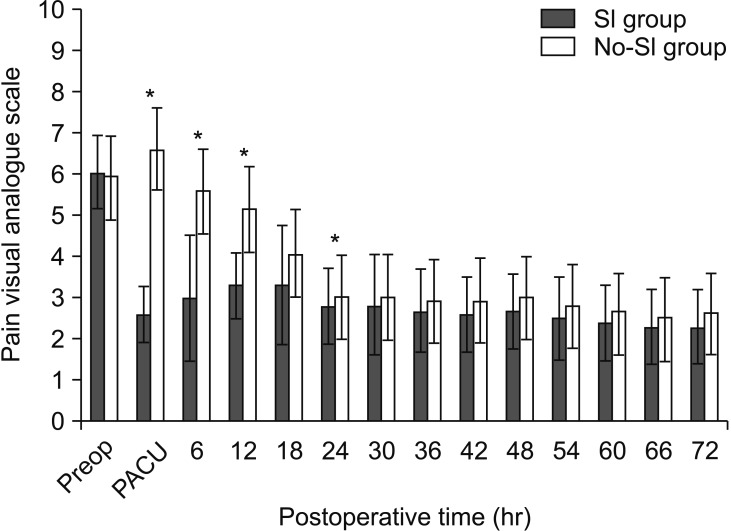
After the surgery, the SI group demonstrated significantly lower VAS pain scores than the no-SI group until POH 24, except for the POH 18. The mean value and standard deviation was 2.6 ± 0.7 for the SI group, and 6.6 ± 1.0 for the no-SI group in the recovery room (p < 0.001); 3.0 ± 1.5 for the SI group, and 5.6 ± 0.9 for the no-SI group at POH 6 (p < 0.001); 3.3 ± 1.4 for the SI group, and 5.1 ± 1.4 for the no-SI group at POH 12 (p = 0.003); 3.3 ± 1.4 for the SI group, and 4.1 ± 1.6 for the no-SI group at POH 18 (p = 0.061); and 2.8 ± 1.2 for the SI group, and 3.0 ± 0.9 for the no-SI group at POH 24 (p = 0.001). After 30 hours, all VAS pain scores between the two groups showed no statistically significant differences (Fig. 1).
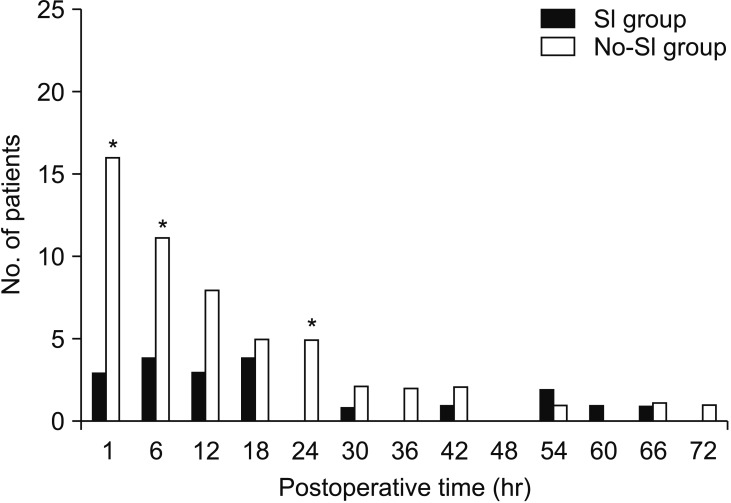
Additional rescue-tramadol requirement was significantly lower in the SI group than in the no-SI group until POH 24, except for POH 12 and 18. At POH 1, three patients in the SI group and 16 patients in the no-SI group required a rescue dose of tramadol (p < 0.001). At POH 6, there was a significant difference in the tramadol requirement between the SI group (4/25) and the no-SI group (11/25, p = 0.024). At POH 12 and 18, there were no significant differences (p = 0.088 and p = 0.685) between the groups. At POH 24, no patient in the SI group required rescue-tramadol, whereas five patients in the no-SI group required a rescue dose of tramadol (p = 0.018). After 30 hours, no statistically significant differences were observed for tramadol requirement between the two groups (Fig. 2).
At POH 72, the mean DHEA-S level significantly decreased in the no-SI group (74.2 ± 47.0 µg/dL) as compared to that in the SI group (110.1 ± 87.1 µg/dL; p = 0.046) (Fig. 3A). However, the levels of insulin and fibrinogen did not differ significantly between the two groups during the study period of 72 hours (Fig. 3B and C). The correlations between the VAS pain scores and each biomarker were also compared. The correlation values between all the biomarkers (DHEA-S, insulin, and fibrinogen) and the VAS pain scores were not significantly different between the two groups (p > 0.05).
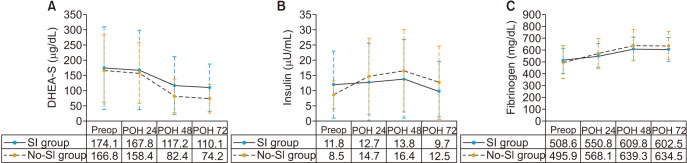 | Fig. 3(A) At postoperative hour (POH) 72, the mean dehydroepiandrosterone sulfate (DHEA-S) level significantly decreased in the no-surgical-site injection (SI) group (74.2 ± 47.0 µg/dL) as compared to that in the SI group (110.1 ± 87.1 µg/dL; p = 0.046). (B, C) There were no significant changes in the levels of insulin and fibrinogen until POH 72 (p > 0.05). All the values are presented as the mean and the standard deviations. Preop: preoperative.
|
Go to :
DISCUSSION
In this study, the mean VAS pain score was significantly low in the SI group as compared to that in the no-SI group on the operation day, except for POH 18. The DHEA-S levels significantly decreased in the SI group as compared to those in the no-SI group at POH 72. There were no significant changes in the insulin or fibrinogen levels at POH 72.
Multimodal analgesia inclusive of SI is commonly utilized for pain management in patients undergoing arthroplasty, and the safety and efficacy profiles of this method are excellent.2324) Although various pain control protocols have evolved over recent years for patients with musculoskeletal trauma, surgical-site, multimodal drug injection has been reported to be progressing recently as a new analgesic method after the surgical treatment for musculoskeletal trauma.22252627) To the best of our knowledge, this investigation is the first study to assess the effect and safety of the surgical-site multimodal drug injection on the mid-shaft clavicular fractures, along with the evaluation of stress biomarkers.
A previous study assessing the plasma concentrations of ropivacaine following an SI with the same dosing parameters as those employed in the present study reported that no patient reached an intravascular concentration at which the side effects may occur.22) The SI can preserve motor functions, which may enable early mobilization and limit the side effects associated with systemic narcotics.27) The preservation of the motor functions with the SI technique may lead to a decreased prevalence of in-hospital falls as compared to that occurring from peripheral nerve blocks.27)
Reducing the consumption of systemic narcotics is an important goal of multimodal pain control. In several studies, SI has been reported to reduce narcotic consumption significantly, which consequently decreased the narcotic-associated adverse effects including nausea, rash, emesis, and pruritus.2829) The standard of care at our institution is to use tramadol as a rescue analgesic. For 42 hours after the surgery, the mean additional rescue-tramadol requirement was lower in the SI group as compared to that in the no-SI group. In particular, at POH 1, 6, and 24, additional rescue-tramadol requirement was significantly lower in the SI group than that in the no-SI group.
In the present study, the VAS pain score in the SI group increased at POH 12 and 18. Oh et al.30) referred to this phenomenon as “rebound pain” that lessens the effect of interscalene block analgesic strategy. Therefore, the phenomenon in the present study can also be considered as rebound pain after SI.
The stress response after the surgery can be characterized by immunologic, neuro-humoral, and metabolic alterations.31) The hypothesis of this study was that the stress response would be characterized mainly by postoperative pain; therefore, the SI may modulate the extent of this response.
The relationship of DHEA-S, pain, and psychological distress has been reported.1832) It has been described frequently that, as a pain predicting marker, DHEA-S decreased when pain arose; therefore, DHEA-S is also useful as a biomarker for orthopedic pain.18) Finset et al.32) also described that DHEA-S was negatively associated with musculoskeletal pain and psychological distress. In our study, the mean DHEA-S level in the no-SI group decreased rapidly after POH 48 than that in the SI group. In particular, the mean DHEA-S level in the no-SI group decreased significantly at POH 72 compared to that in the SI group (Fig. 3A).
Previous studies have reported that pain is related with insulin resistance.33) Insulin sensitivity after operation decreases according to the magnitude of surgery because a major surgery may be more painful than a minor surgery.34) Liu et al.16) reported that compared to the only general anesthesia group (20.39 ± 25.60 µU/mL), the insulin level significantly decreased in the general anesthesia with interscalene block group (10.55 ± 7.92 µU/mL) at POH 42 (p = 0.048). Uchida et al.19) reported an insulin resistance during surgery and suggested that postoperative insulin resistance is partially prevented by epidural anesthesia. In this study, although there were no statistically significant differences between the two groups, the mean insulin level in the no-SI group increased more rapidly at POH 24 (8.5 to 14.7 µU/mL) than that in the SI group (11.8 to 12.7 µU/mL). Although the mean preoperative insulin level in the SI group was higher than that in the no-SI group, all of the mean postoperative insulin levels in the SI group were lower than those in the no-SI group (Fig. 3B).
Schell et al.35) reported that linear regression analyses showed statistically significant predicting values of higher fibrinogen levels at the initial test instance for pain 12 months after surgery, and thus they suggested the main role of fibrinogen in the human body as an inflammatory protein. However, Liu et al.16) reported that among all patients who underwent a surgery, there was no significant difference in the fibrinogen level between two groups divided into the only general anesthesia group and general anesthesia with the interscalene block group. In the present study, although all of the fibrinogen levels increased until POH 48 in both groups and then decreased at POH 72, there were no significant differences in the fibrinogen level between the two groups (Fig. 3C).
There are several limitations in the present study. First, this study is a retrospective study, not a prospective randomized controlled study. Second, the sample size was small. Chung et al.22) suggested that 22 patients were needed in each group to demonstrate a 20% difference in pain severity (power, 80%; p = 0.05); however, Liu et al.16) suggested that for a difference of 1.0 to 1.3 points in VAS pain, 44 patients were required per group to detect a 1.5-point difference (power, 80%; p = 0.05). Third, the diabetes mellitus patients were not excluded. For an accurate evaluation of the relation between postoperative pain and insulin, comparison of the glucose and insulin levels is necessary in diabetes mellitus patients. However, this limitation did not affect the results of the intergroup comparison because the ratio of diabetes mellitus showed no difference between two groups. Fourth, the stress biomarkers were evaluated at only POH 24, 48, and 72; however, the measurement of VAS pain scores was performed every 6 hours. Liu et al.16) reported that there was no correlation between VAS pain scores and the stress biomarkers. The present study also showed no correlation between the VAS pain scores and the stress biomarkers. We think these results could be attributable to the statistical analysis based on limited data because the correlation in the two groups was only evaluated at POH 24, 48, and 72, not every 6 hours. The stress biomarkers tended to show delayed relation with VAS pain scores in previous studies. In addition, the DHEA-S level decreased after surgery while the levels of insulin and fibrinogen increased at POH 24 and 48 and then decreased at POH 72 (Fig. 3).
After internal fixation of the clavicular fracture, surgical-site, multimodal drug injection relieved pain effectively on the day of surgery without any complications. Therefore, we believe that surgical-site, multimodal injection is a safe and effective method for pain management after internal fixation of a clavicular fracture.
Go to :
 XML Download
XML Download