

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Incorrect creation of bone tunnels is one of the most common causes of failure of anterior cruciate ligament (ACL) reconstruction.1) Their accurate location is an essential factor for placing the intra-articular graft of an appropriate length as well as preventing impingement, limited motion, flexion contracture, laxity, and early failure.23)
Conventional transtibial (TT) techniques for ACL reconstruction have limitations in creating femoral tunnels on the anatomical footprint of the ACL. Therefore, they have been modified, and thus termed as modified TT techniques. The modified techniques have been reported to be useful in creating oblique femoral and tibial tunnels while preserving the native femoral footprint of the ACL.4567) It remains problematic, however, that more oblique and shorter tibial tunnels should be created for drilling femoral and tibial footprints through their centers.8) Due to the shorter tibial tunnel, the bone-patellar tendon-bone (BPTB) graft of patellar and tibial bone blocks (25–30 mm) becomes longer than the tunnel. Graft-tunnel length mismatch with BPTB grafts occurs accordingly. This has been described as a potential complication of the modified TT techniques for ACL reconstruction using the BPTB graft, which may lead to graft extrusion, failure of interference screw fixation as well as decreased stiffness, micromovement, and laxity of the graft.91011) To avoid this, a shorter BPTB graft is required for the modified TT techniques in ACL reconstruction. Still, there is a paucity of data regarding the optimal length of patellar and tibial bone blocks. Given the above background, we conducted this study to determine the optimal length of patellar and tibial bone blocks for the modified TT techniques in ACL reconstruction using the BPTB graft.
METHODS
Patients and Study Setting
The current single-center, retrospective study was conducted in a total of 64 patients with an ACL tear who underwent surgery at Konkuk University Chungju Hospital between March 2015 and February 2016. Inclusion criteria for the current study are as follows: (1) patients with available follow-up data; (2) patients who underwent primary ACL reconstruction with the autologous BPTB graft; and (3) patients who underwent surgery using the modified TT techniques. Exclusion criteria for the current study are as follows: (1) patients who had a past history of knee surgery, revision ACL reconstruction, or multi-ligamentous reconstruction surgery; (2) patients lost to follow up; and (3) patients who were deemed to be ineligible for study participation according to our judgment.
We therefore enrolled a total of 64 patients in the current study. The study was approved by the Institutional Review Board of Konkuk University Chungju Hospital (IRB No. KUCH-2013-048). Informed consent was waived due to its retrospective nature.
Operative Procedure
Standard arthroscopic ACL reconstruction was performed using the autologous BPTB graft via the modified TT technique by the senior author (DK). All the tibial tunnels were created using a tibial drill guide (Arthrex, Naples, FL, USA), which was set at 50° and intra-articularly positioned at the center of the footprint of ACL. To create the anatomical femoral tunnel, the tibial drill guide was placed more horizontally and then directed to the common intraarticular entry point at the center of the tibial footprint of ACL. Subsequently, the extra-articular starting point was placed on the cortex of the medial tibia midway between the tibial tuberosity and the posteromedial margin of tibia, which was just superior to the pes anserinus and anterior to the medial collateral ligament. Then, with the knee joint placed in varus and external rotation, attempts were made to create the femoral tunnel in the anatomical femoral footprint of the ACL.
Measurement of the Length of the Tunnel
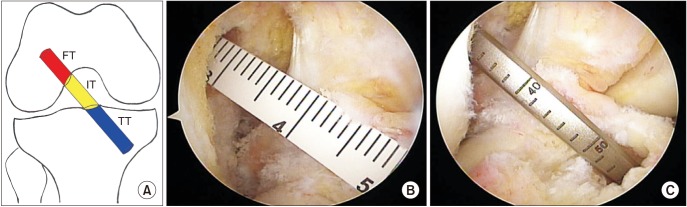
After harvesting the BPTB graft, we measured its length and that of the patellar tendon, patellar bone block and tibial bone block using the arthroscopic ruler and double-checked measurements using a length gauge. Both the femoral tunnel and the tibial tunnel were evaluated for the total length, the intra-articular, inter-tunnel distance (Fig. 1). After the passage and fixation of autologous BPTB graft, the length of protruded graft, such as graft-tunnel length mismatch, was measured using the ruler. All measurements were recorded.
Patient Evaluation and Criteria
We postoperatively analyzed the position of intraarticular openings of femoral and tibial tunnels on three-dimensional (3D) multi-detector computed tomography scans using the GE Lightspeed 16-slice scanner (Toshiba, Otawara, Japan), as previously described.12) We evaluated baseline and clinical characteristics of the patients, such as age, sex, height, and bone mass index (BMI) through a retrospective analysis of medical records.
In the current study, outcome measures include the length of tibial and femoral tunnels, inter-tunnel distance, length of the BPTB graft, the patellar tendon, the patellar bone block, and the tibial bone block, and graft-tunnel length mismatch. Moreover, the total length of tunnels was defined as a sum of the length of the tibial tunnel, intertunnel distance, and length of the femoral tunnel. Furthermore, the optimal length of the bone block was calculated as (the total length of tunnels − the length of the patellar tendon) / 2. Finally, we analyzed correlations of outcome measures with the height and BMI of the patients.
Data Analysis
All data was expressed as mean ± standard deviation. Each outcome measure was analyzed as compared with the corresponding one described in the literature. To identify correlations of measurements with height and BMI of the patients, both a correlation analysis and a linear regression analysis were performed. Statistical analysis was performed using the IBM SPSS ver. 20.0 (IBM Corp., Armonk, NY, USA). Statistical significance was set at p < 0.05.
Go to : 
RESULTS
Baseline and Clinical Characteristics of the Patients
The clinical series consists of 44 male (68.7%) and 20 female (31.3%) patients with a mean age of 31.8 years (range, 17 to 65 years). The operated side was left in 34 patients (53%) and right in 30 patients (47%).
Outcome Measures
The mean length of femoral tunnel was 29.2 mm (range, 27 to 30 mm). The mean length of tibial tunnel was 33.7 mm (range, 28 to 40 mm). The mean inter-tunnel distance was 23.9 mm (range, 22 to 29 mm). The mean total length of tunnels was 86.8 mm (range, 80 to 96 mm) (Table 1). The mean length of patellar tendon was 43.5 mm (range, 37 to 51 mm). The mean length of patellar bone block was 23.4 mm (range, 22 to 25 mm). The mean length of tibial bone block was 23.9 mm (range, 22 to 25 mm). The mean length of BPTB graft was 90.7 mm (range, 82 to 98 mm) (Table 2).

Table 1
Mean Length of Tunnels in Modified Transtibial Anterior Cruciate Ligament Reconstruction
![]()

Graft-Tunnel Length Mismatch
There were 52 cases (81.3%) of graft-tunnel length mismatch with a mean length of 3.9 mm (range, 0 to 8 mm) (Table 3).

Optimal Length of Bone Block
The optimal length of bone block was 21.7 mm (range, 19.5 to 23.5 mm). When the length of femoral tunnel was assumed as 25 mm and 30 mm, the optimal length of bone block was calculated as 19.6 mm (range, 17 to 21.5 mm) and 22.1 mm (range, 19.5 to 24 mm), respectively (Table 4 and Fig. 2).
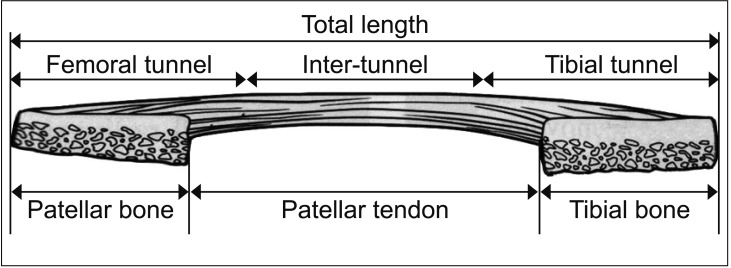 | Fig. 2Ideal length of patellar bone block and tibial bone block of bone-patellar tendon-bone graft in anterior cruciate ligament reconstruction: [total tunnel length (femoral tunnel + inter-tunnel distance + tibial tunnel) − patellar tendon length] / 2.
|

Correlations of Patients' Height and BMI with the Length of Tibial Tunnel, Inter-tunnel Distance, the Length of Patellar Tendon, and the Extent of Graft-Tunnel Length Mismatch
On linear regression analysis, patients' height had a significant correlation with the length of tibial tunnel (p = 0.003), inter-tunnel distance (p = 0.014), and length of patellar tendon (p < 0.001). But it had no significant correlation with the extent of graft-tunnel length mismatch (p = 0.753). Patients' BMI had no significant correlation with the length of tibial tunnel (p = 0.271), inter-tunnel distance (p = 0.219), length of patellar tendon (p = 0.936), and the extent of graft-tunnel length mismatch (p = 0.856).
Go to :
DISCUSSION
The results of the study can be summarized as follows: (1) The mean length of tibial tunnel was 33.7 mm (range, 28 to 40 mm), which is significantly shorter that of the traditional TT technique (42.1 mm9) and 51.62 mm13)). (2) The total mean length of tunnels was 86.8 mm, and the mean length of BPTB graft was 90.7 mm. The mean length of patellar and tibial bone blocks was 21.7 mm. (3) The graft-tunnel length mismatch was a mean of 3.9 mm.
Based on the above results, it can be inferred that graft-tunnel length mismatch can be prevented by adjusting the length of patellar and tibial bone blocks for the modified TT technique using the BPTB graft. We therefore propose that when the length of the femoral tunnel is 30 and 25 mm, the length of patellar and tibial bone blocks should correspond to 22.1 and 19.6 mm, respectively.
To date, various measurement techniques and mathematical formulas have been used to avoid the graft-tunnel length mismatch. These include “graft − 50” formula, “patellar tendon + 2” formula, and “patellar tendon + 7°” rule.141516) But each of these methods has its own merits and demerits: “graft − 50” formula can make an unacceptable tunnel length; “patellar tendon + 2” formula is technically difficult and may require measurement of proposed tibial tunnel length and adjustment before the selection of the optimal angle for the placement of the guide; and “patellar tendon + 7°” rule may result in an unacceptable steep tibial tunnel with a tibial guide angle of > 55°. Moreover, the “patellar tendon + 7°” rule cannot be used to appropriately place the guide pin on the femoral footprint because its angle is relatively steeper. It would, therefore, be mandatory not only to create anatomical tibial and femoral tunnels but also to harvest the BPTP graft of an appropriate length. The BPTP graft is usually harvested before the creation of tunnels in ACL reconstruction. This makes it possible to adjust the length of BPTP graft by cutting the patellar and tibial bone blocks with optimal length.
To date, several attempts have been made to allow bitunnel interference screws and thereby to avoid graft-tunnel length mismatch. These include recession of the femoral bone plug,17) free bone block placement,18) flipping of the tibial bone plug,19) use of soft tissue interference screws,20) and rotation of graft.21) The disadvantages include poor biomechanical stability and technical errors, which can be resolved with use of the BPTB graft with an appropriate length. In our series, the length of patellar tendon was 43.1 mm, shorter than that in previous reports (48.4 mm,9) 45.48 mm,13) and 52.6 mm22)). Presumably, this might arise from differences in the morphotype and ethnicity.
Recent efforts have been made to preoperatively avoid graft-tunnel length mismatch, according to which not only patient-related factors,23) such as height and weight, but also preoperative imaging studies of the patellar tendon24) should be considered in identifying the appropriate length of the overall graft construct. Indeed, both patients' height and the length of patellar tendon measured on magnetic resonance imaging scans are closely associated with the overall length of the graft. In the current study, we found that the patients' height had a significant correlation with the length of tibial tunnel (p < 0.01), inter-tunnel distance (p < 0.05) and length of patellar tendon (p < 0.001).
There are some limitations of the current study. First, we performed the modified TT technique with the tibial guide placed in an oblique position (50°) based on intra-articular references of the PCL, medial tibial spine, and anterior horn of lateral meniscus as well as offset femoral aimer depending on the direction of tibial tunnel. Despite successful outcomes, it has been suggested that the aperture of the tibial tunnel be displaced posterior to the intra-articular references in the native ACL footprint. This may shorten inter-tunnel distances.25) Second, we analyzed the position of the tunnel based on CT scans rather than assessment of the native ACL footprint in a poor resource setting. The method that evaluates the native ACL footprint requires magnetic resonance images of the contralateral knee and their 3D reconstruction, but this is considered to be practically impossible in current clinics.
In conclusion, our results indicate that it would be mandatory to determine the optimal length of tibial tunnel in the modified TT technique for ACL reconstruction using the BPTB graft. Further large-scale, multi-center studies are warranted to establish our results.
Go to :
 XML Download
XML Download