

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Synovial chondromatosis of the hip is a benign proliferative disease of synovium. It is characterized by many osteochondral loose bodies around the synovium.1234) While the pathogenesis of synovial chondromatosis is unknown,5) this condition presents with pain, mechanical locking, and stiffness of the involved joint.678) Furthermore, if untreated, mechanical damage of the articular cartilage leads to degenerative osteoarthritis of the hip.910) Therefore, surgical intervention is recommended for symptomatic patients with synovial chondromatosis of the hip. Surgical treatment is achieved either by open or arthroscopic removal of loose bodies.11) Open surgery allows for complete access to the joint12) for removal of loose bodies and complete synovectomy. However, open surgery has a risk of complications such as avascular necrosis of the femoral head, iatrogenic femoral neck fracture, and prolonged rehabilitation.1113141516)
Recently, arthroscopic surgery has been introduced to treat intra-articular pathologies including synovial chondromatosis of the hip. Compared to open surgery, arthroscopic surgery was associated with less invasiveness, decreased hospital stay, less postoperative pain, less surgical complications, and faster recovery.101718) Meanwhile, incomplete removal or recurrence is the concern of arthroscopic surgery because complete synovectomy is technically difficult.1119) When loose bodies remain, reoperation is possibly required for patients with persistent symptoms after the surgery.11520) However, there has been no study on the natural course of remaining loose bodies due to incomplete removal after arthroscopic surgery.
The purposes of this study were to evaluate the results of arthroscopic synovectomy and loose body removal for synovial chondromatosis of the hip and to present radiographic changes of the remaining loose bodies due to incomplete removal after arthroscopic surgery.
METHODS
We retrospectively reviewed 13 patients in whom synovial chondromatosis of the hip were treated with arthroscopic synovectomy and removal of loose bodies at Seoul National University Bundang Hospital between 2008 and 2016. The diagnosis of synovial chondromatosis of the hip was confirmed by magnetic resonance imaging in patients who had characteristic appearance in radiography including numerous intra-articular radiopaque bodies and the absence of substantial arthritic changes.21)
Of the 13 patients, three patients were lost to follow up before a minimum follow-up of 1 year after the operation. The remaining 10 patients (10 hips) were available for complete clinical and radiographic analysis. There were eight males and two females with a mean age of 35.4 years (range, 21 to 58 years) at the time of hip arthroscopy. The mean body mass index was 23.0 kg/m2 (range, 18.3 to 25.9 kg/m2). The mean duration of follow-up was 3.8 years (range, 1 to 6.8 years).
Surgical Technique
All patients were placed in a supine position on a fracture table with the affected limb in traction. Under general anesthesia, gentle and sufficient traction was applied to the affected limb to distract the joint by 10–12 mm using an image intensifier. During traction, the hip was placed in approximately 5° of abduction and 20° of internal rotation such that the femoral neck was parallel to the ground. All hip arthroscopies were performed by one surgeon (YKL) via three portals (anterior, anterolateral, and posterolateral portals) using 70° angled 5.5-mm arthroscopes. For initial inspection of the hip joint, a 70° angled 5.5-mm arthroscope was inserted through the anterolateral portal, which was created 1 cm distal and 2 cm anterior to the tip of the greater trochanter. The posterolateral portal was placed 1 cm distal and 2 cm posterior to the tip of the greater trochanter. The anterior portal was placed at the intersection of a sagittal line drawn distally from the anterior superior iliac spine and a transverse line drawn from the tip of the greater trochanter. A banana knife or electrocautery was used to enlarge each portal to facilitate maneuvering of the instruments. After establishing the three portals, each portal kept the arthroscopic sheath for rapid interchanging of the arthroscope, various arthroscopic instruments, and an inflow cannula between portals. To obtain a more precise view, 1 mL 0.1% epinephrine solution mixed with every 3,000 mL irrigation fluid was injected via a 5.5-mm inflow cannula, and using a 4.2-mm motorized shaver, electrocautery was performed to resect the torn labrum.
An anterior capsulotomy was made between anterior and anterolateral portals to assess the central compartment. Mainly using a 70° angled arthroscope in the viewing portal, arthroscopic loose body removal and synovectomy were performed through the working portal, the anterior capsulotomy opening. After the traction was released, the arthroscope was moved toward the peripheral compartment through an anterior or anterolateral portal while the hip joint was flexed by around 45°. Then arthroscopic loose body removal and synovectomy were performed. When there were lesions in the medial anteroinferior region or posteroinferior region, anterior capsulotomy was more extended distally to remove any lesions as completely as possible. Most loose bodies could be removed using a probe or grasper, and smaller loose bodies were removed by lavage. In cases where the loose bodies were too large and thus could not be completely removed, the anterior capsule was more excised to get the loose bodies out of the extracapsular space. However, in cases where loose bodies were located at the posterior or posterolateral region of the peripheral compartment in the joint and thus fixed by the synovium, the loose bodies could not be removed. To allow the remaining loose bodies to flow out, the excised capsule was not repaired after the arthroscopic procedure. The removed loose bodies and synovium were sent for histopathological examination. Tolerable range of motion of hips and weight bearing were permitted immediately after surgery.
Clinical Outcomes
Routine objective follow-ups were performed at 6 weeks and 3, 6, 9, and 12 months after discharge. We asked all patients about pain, and visual analogue scale scores were used to measure pain. University of California Los Angeles (UCLA) activity scale scores were evaluated at each visit. All patients were assessed using a modified Harris hip score (HHS) preoperatively and at the final follow-up.22) This modified score excluded items of deformity (4 points) and range of motion (5 points) from the original HHS because neither of these is a principle indication for hip arthroscopy. Therefore, the modified HHS included only the pain (44 points) and function (47 points) portions of the original HHS and was adapted to evaluate outcomes of hip arthroscopy as described elsewhere.22) A multiplier of 1.1 provides a total possible score of 100.
Radiological Outcomes
Plain radiographs were reviewed for all the patients preoperatively, immediately postoperatively, and at the final follow-up. The preoperative plain radiographs were the anteroposterior views of the hip joint and frog-leg lateral views. We checked for the existence and locations of radiopaque loose bodies preoperatively, immediately postoperatively, and at the final follow-up. The degree of osteoarthritis was evaluated according to the Tönnis classification.23)
Statistical Analysis
Descriptive analysis was used in this study. To compare pre- and postoperative clinical scores, the Wilcoxon signed-rank test was used to analyze statistical significance. A p < 0.05 was considered statistically significant. Statistical analyses were conducted using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). We conducted this study in compliance with the principles of the Declaration of Helsinki. The protocol and design of this study were approved by the Institutional Review Board of Seoul National University Bundang Hospital (IRB No. B-1810-499-106), which waived informed consent.
RESULTS
Preoperative radiographs demonstrated radiopaque loose bodies in nine of the 10 hips (90%). According to the Tönnis radiographic classification of hip osteoarthritis, four hips were grade 0, and six were grade 1. Magnetic resonance imaging confirmed intra-articular loose bodies in all 10 hips. All 10 patients underwent arthroscopic procedures including extensive capsulectomy as well as loose body removal. The mean operation time was 144 minutes (range, 75 to 185 minutes). No major complications including neurovascular injury occurred after the arthroscopic procedures. There was one patient with skin problem at the perineum after traction for 2 hours, which healed spontaneously.
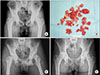
The clinical outcomes such as modified HHS, UCLA score, and Western Ontario and McMaster Universities Osteoarthritis Index score improved at the time of the latest follow-up (Table 1). Among nine hips with preoperative radiopaque loose bodies, seven hips had the remaining loose bodies even after arthroscopic surgery. However, the remaining loose bodies disappeared in five hips (71.4%, 5/7) at the last follow-up (Fig. 1). Any osteoarthritic progression was not observed in all hips for the mean follow-up of 3.8 years (range, 1 to 6.8 years). There was no recurrence of synovial chondromatosis.
DISCUSSION
This study demonstrated that arthroscopic procedures including extensive capsulectomy as well as loose body removal can be effective for synovial chondromatosis of the hip in spite of some remaining loose bodies.
In the treatment of synovial chondromatosis of the hip, removal of loose bodies is essential to relieve pain, prevent recurrence, and delay progression or secondary joint arthritis.10111924) Traditionally, open surgery has been considered as the optimal treatment for synovial chondromatosis of the hip.25) Although arthroscopy has been introduced to treat this disorder, there has been some concern about the feasibility of radical synovectomy, high recurrence rates, and the frequent necessity of reoperation due to remaining loose bodies.18)
The recurrence rates after open surgical treatment for synovial chondromatosis ranged from 0% to 22%.141826) The recurrence rates after arthroscopic treatment for synovial chondromatosis ranged from 7.1% to 16.7%.1519) Although almost all regions of the synovium can be identified during the arthroscopic procedure, it is difficult to remove loose bodies located at the medial portion of the hip joint, as an arthroscope cannot easily reach this area.141527) To completely remove loose bodies, the arthroscopic procedure might require a prolonged traction time, which results in traction-related complications including neuropraxia of the pudendal nerve and perineal skin problems as in one of our patients.28) The mean operation time (144 minutes) in this study might be longer than that of open hip arthrotomy.
In this study, we arthroscopically removed loose bodies and performed synovectomy as completely as possible. To avoid remaining loose bodies, we additionally made an extensive opening at the anterior capsulotomy site. Inaccessible loose bodies located in the medial region could be effectively removed through the opening of the anterior capsulectomy site after surgery; five of seven hips (71.4%) with the remaining loose bodies did not have any loose bodies at the final follow-up. We could not explain the exact reason for disappearance of the remaining loose bodies at the final follow-up. The extensive capsulectomy and wide opening of the anterior capsule might have allowed the loose bodies to be out and absorbed in the extra-articular space. Recently, it has been recommended that the excised capsule be repaired after an arthroscopic procedure to reduce the risk of anterior instability of the hip.29) Fortunately, there was no patient with instability in this study.
There were some limitations in this study. First, this is a retrospective study and the number of patients is too small; however, synovial chondromatosis of the hip is rare condition. Second, we did not have any comparison with an open surgical procedure and arthroscopy with not-extensive capsulectomy. Despite these limitations, considering the reduced risk of serious complications and faster return to daily activities of life, hip arthroscopic procedures including extensive capsulectomy and loose body removal can be useful to treat synovial chondromatosis of the hip.
 XML Download
XML Download