

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hepatitis B virus (HBV), a DNA virus with a human-only reservoir, is a serious global health concern. The worldwide prevalence of HBV infection is estimated to be 3.61%, and it is similar in rheumatoid arthritis (RA) patients.12 Coexistence of RA with hepatitis B makes the treatment of RA risky because some disease-modifying antirheumatic drugs (DMARDs) such as methotrexate and leflunomide may cause hepatotoxicity and some drugs that affect immune response can lead to reactivation of HBV.3456 Consequently, RA treatment may differ according to hepatitis B status and this could lead to different arthritis outcomes.
Previous studies of RA patients with concomitant hepatitis B tended to focus on the safety of arthritis medications and reactivation of hepatitis.7891011 Only a small number of studies addressed differences in disease characteristics and treatment patterns of RA in relation to hepatitis B status.12 However, whether hepatitis B affects treatment outcomes such as RA disease activity remains unclear.
In this study, we investigated potential variation in changes in disease activity markers upon treatment between RA patients based on their concomitant hepatitis B status. We employed hepatitis B virus surface antigen (HBsAg) as a serological marker of HBV infection.
METHODS
Study population
A retrospective medical chart review was performed by two rheumatologic fellows using single center data, from 1 January 2000 to 31 March 2015. Patients with overlapping autoimmune diseases, liver diseases other than hepatitis B, or other comorbidities that could affect RA treatment (e.g., cardiovascular diseases, chronic kidney diseases, interstitial lung disease, diabetes, or previous malignancy within five years) were excluded. Forty patients with HBsAg-positive RA were finally enrolled in the study. We included a control group that comprised 112 age-matched, sex-matched, and entry-time-matched RA patients with negative HBsAg and negative hepatitis B core antibody (HBcAb) using propensity score matching.
Collection of study data
Baseline and longitudinal data of each participant were retrospectively collected at all visits from the date of entry to 31 March 2015. An electronic standardized abstraction form was used for data collection. Baseline data included demographic data, date of RA symptom onset, presence of erosions, and previous medication use. The modified Sharp/van der Heijde (mSvH) scoring system was used to quantify radiologic damage.13 Because X-ray data were insufficient, only hand X-rays at baseline were used in the assessment. Rheumatoid factor (RF) was measured by immunoturbidimetric assay (Roche/Hitachi Modular P. Roche Diagnostics, Mannheim, Germany; positivity ≥ 15 IU/mL). Anti-cyclic citrullinated peptide antibodies (ACPA) were detected using a chemiluminescent microparticle immunoassay (Architect, Abbott Laboratories, Abbott Park, IL, USA; positivity ≥ 5 U/mL). The disease activity score for 28 joints with three variables (DAS28-3), tender joint counts, swollen joint counts, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), liver function test as measured by alanine aminotransferase (ALT) in units/liter, and RA medication prescription were collected at baseline and updated at every visit. Because patient global assessment data were not collected, DAS28-3 was used as a disease activity marker.1415
In HBsAg-positive RA patients, prescription of antiviral agents for hepatitis B, purpose of antiviral use (prophylactic or therapeutic), HBsAg positivity, and HBV DNA data were collected from follow-up visits. Characterization of hepatitis B was done at baseline and at every visit to the hepatology clinic. The “inactive HBsAg carrier state” is characterized by HBsAg positivity for > 6 months, serum HBV DNA titer of < 20,000 IU/mL in HBeAg-positive patients or of < 2,000 IU/mL in HBeAg-negative patients and persistently normal ALT levels. “Chronic hepatitis B (CHB)” is characterized by HBsAg positivity for > 6 months, serum HBV DNA titer of > 20,000 IU/mL in HBeAg-positive patients or of > 2,000 IU/mL in HBeAg-negative patients, and persistent or intermittent elevation in ALT levels.16 Development of hepatocellular carcinoma and reactivation of hepatitis B were also assessed. HBV reactivation was defined by a > 10-fold (1 log10 IU/mL) rise in HBV DNA level when compared with the baseline value.17
Statistical analysis
For selection of control group, propensity score matching was performed using age, sex, and entry time, with a 1:3 case-control ratio. The Kolmogrov-Smirnov and Shapiro-Wilk tests were used to check normality of metric data. For data with a normal distribution, the mean ± standard deviation (SD) is shown, and we applied Student's t-tests for comparisons. For non-normally distributed data, we indicate the median (interquartile range) and used the Wilcoxon rank sum test. Categorical variables were compared using χ2 or Fisher's exact tests. Paired t-test for normally distributed data and Wilcoxon signed rank test for non-normally distributed data were used to compare RA disease activity markers and ALT level at the end of follow-up with those at study entry. Generalized estimating equations (GEEs) were used to assess the association between HBsAg positivity and RA disease activity markers/medication use over time. In GEE models, data were adjusted for visit date and further adjusted for age, sex, and duration of RA. All statistical analyses were performed using SAS, version 9.4 (SAS Institute Inc., Cary, NC, USA).
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Samsung Medical Center (IRB No. 2015-09-069). The requirement for informed consent was waived since the study involved a minimum risk to the enrolled patients in this retrospective study and no identifiable information was used.
RESULTS
The study sample consisted of 40 patients with HBsAg-positive RA and 112 patients with HBsAg-negative RA. A description of patient characteristics at baseline is provided in Table 1. Median age was 43 (interquartile range [IQR], 37–53) years, and women constituted 76.3% of the total study population. There were no significant differences between groups with regard to demographics RA disease characteristics including RF positivity, ACPA positivity, and the presence of erosions; instruments reflecting RA disease activity; or previous medication use at baseline. Methotrexate tended to be less frequently prescribed for HBsAg-positive patients, but the difference was not statistically significant. Leflunomide, cyclosporine, azathioprine, and biologic agents including tumor necrosis factor α (TNF-α) inhibitors were less commonly used in the study population, and there were no significant differences in the use of these medications between groups at baseline.
Table 1
Baseline characteristics of HBsAg-positive and HBsAg-negative RA patients

Data are presented as median with IQR or number (%).
HBsAg = hepatitis B virus surface antigen, RA = rheumatoid arthritis, RF = rheumatoid factor, ACPA = anti-cyclic citrullinated peptide antibodies, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, DAS28-3 = disease activity score for 28 joints with three variables, DMARD = disease-modifying antirheumatic drug, ALT = alanine aminotransferase, IQR = interquartile range.
aData were available for 33 and 100 patients in the HBsAg-positive group and the HBsAg-negative group, respectively; bPatients who had already been diagnosed and treated with RA at another hospital.
At baseline, the HBsAb-positive rate was significantly higher in the HBsAg-negative group than the HBsAg-positive group (49.1% vs. 7.5%; P < 0.001). No differences were noted in the level of ALT. In HBsAg-positive patients, the positive rate for HBcAb was 96.9% (n = 31) and that for HBeAg was 19.4% (n = 7). HBV DNA data were available in 35 patients (87.5% of HBsAg-positive patients); HBV DNA positivity was 37.1% (n = 13). Ten percent of HBsAg-positive patients received antiviral treatment (n = 4). Among 40 patients who had HBsAg, 28 patients were classified as inactive carriers and 9 patients were classified as having CHB. Three patients had been diagnosed with liver cirrhosis.
The median number of visits per subject was 28 (IQR, 19–61) in the HBsAg-positive group and 27 (IQR, 16–45) in the HBsAg-negative group (P = 0.175). The median follow-up duration per subject was 2,361 (IQR, 1,462–4,326) days in the HBsAg-positive group and 1,863 (IQR, 1,133–3,659) days in the HBsAg-negative group, was similar between these groups (P = 0.119).
We used GEE regression analysis to determine the effects of time and HBsAg-positivity on RA disease activity markers and ALT (Table 2). All RA disease activity markers were negatively associated with time (P < 0.05 for all models). Swollen joint count was the only instrument that showed a significant interaction between time and HBsAg-positivity in both unadjusted and adjusted models (β-estimate, 8.18; 95% confidence interval [CI], 1.40–14.96; P = 0.018 in the unadjusted model; β-estimate, 7.91; 95% CI, 1.41–14.41; P = 0.017 in the adjusted model). We observed a significant effect of HBsAg-positivity on the relationship between time and DAS28-3 (β-estimate, 2.79; 95% CI, 0.18–5.57; P = 0.026), but this interaction did not remain significant after adjustment for age, sex, and duration of RA. For tender joint count, ESR, and CRP levels, there were no interaction between time and HBsAg-positivity. ALT levels did not change significantly with time or with HBsAg-positivity.
Table 2
Regression analysis (GEE) of the effects of time and HBsAg-positivity on disease activity markers and ALT, adjusting for within-subject correlations

GEE = generalized estimating equation, HBsAg, hepatitis B virus surface antigen, ALT = alanine aminotransferase, CI = confidence interval, DAS28-3 = disease activity score for 28 joints with three variables, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, RA = rheumatoid arthritis.
aModel A adjusted for time only; bModel B adjusted for time, age, sex, and duration of RA; cThe HBsAg-negative group was coded as 0 and the HBsAg-positive group was coded as 1; dTime × HBsAg refers to the interaction term between time and HBsAg positivity.
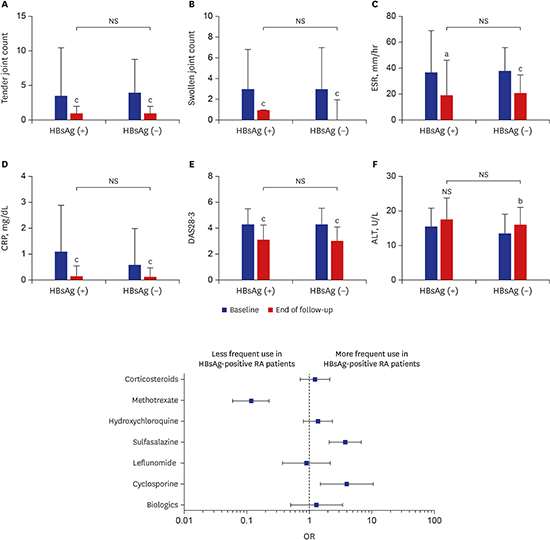
At the end of follow-up, disease activity markers were improved compared with baseline (Fig. 1). There were no significant differences in disease activity markers between HBsAg-positive and HBsAg-negative patients.
Fig. 1
RA disease activity markers and liver function test of HBsAg-positive and HBsAg-negative RA patients at baseline and at the end of follow-up; (A) Tender joint count, (B) Swollen joint count, (C) ESR, (D) CRP, (E) DAS28-3, and (F) ALT.
The P values > 0.05 marked NS.
RA = rheumatoid arthritis, HBsAg = hepatitis B surface antigen, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, DAS28-3 = Disease Activity Score for 28 joints with three variables, ALT = alanine aminotransferase, NS = not significant.
aP = 0.01–0.05, bP = 0.001–0.01, cP < 0.001.

When all study visits were analyzed, methotrexate was less frequently used in HBsAg-positive patients (odds ratio [OR], 0.09; 95% CI, 0.04–0.19; P < 0.001; Fig. 2). HBsAg-positive patients were more likely to be prescribed sulfasalazine (OR, 3.67; 95% CI, 1.94–6.95; P < 0.001) and cyclosporine (OR, 3.57; 95% CI, 1.33–9.54; P = 0.011). On unadjusted analysis, tacrolimus was more frequently used in HBsAg-positive patients, but after adjusting for age, sex, and duration of RA, this difference was not significant. Hydroxychloroquine was prescribed somewhat more often in HBsAg-positive patients, but this difference was not statistically significant. With regard to corticosteroids, leflunomide, and biologic agents including TNF-α inhibitors, there were no significant differences. Combination therapy with conventional DMARDs was significantly more frequently applied in HBsAg-positive patients than HBsAg-negative patients (OR, 2.22; 95% CI, 1.19–4.14; P = 0.012); however, there was no significant difference in the use of combination therapy with biologic agents between the two groups (OR, 0.76; 95% CI, 0.14–4.14; P = 0.755). The frequency of intraarticular injection of corticosteroids was higher in HBsAg-positive patients than HBsAg-negative patients (median 2, IQR, 1–8 vs. 1, IQR, 0–3; P = 0.001) during the study period.
Fig. 2
Adjusted OR and 95% CIs (lines) for use of RA medications over all study visits. An OR > 1 represents more frequent use in HBsAg-positive patients.
OR = odds ratio, CI = confidence interval, RA, = rheumatoid arthritis, HBsAg = hepatitis B surface antigen.

Among 40 patients with HBsAg-positivity, 15 patients (37.5%) received antiviral treatment. The purpose of antiviral treatment was prevention of hepatitis reactivation in 8 patients and therapy for hepatitis or cirrhosis in 7 patients. During the study period, one patient with CHB at baseline was newly diagnosed with liver cirrhosis and another patient who was an inactive carrier at baseline was newly diagnosed with CHB (Fig. 3). Two incident cases of hepatocellular carcinoma were observed.
Fig. 3
Changes in hepatitis B status during the study period. (A) Status changes in all HBsAg-positive RA patients (n = 40). (B) Status changes in HBsAg-positive RA patients receiving antiviral agents (n = 15). Antiviral drugs were used for prophylaxis (broken line) and for therapy (solid line). Black circles (●) indicate reactivation of hepatitis B. One patient who had received previous antiviral agent therapy and showed poor adherence to the drug regimen (as indicated by a zigzag line) experienced reactivation.
HBsAg = hepatitis B surface antigen, RA = rheumatoid arthritis.

Hepatitis reactivation occurred in 4 HBsAg-positive RA patients (10%, Table 3). One patient was an inactive carrier, and the other patients had CHB at baseline. Among the patients who experienced HBV reactivation, only one patient had received previous antiviral treatment at baseline, but the patient exhibited lower adherence to drug. The HBV DNA level decreased below the detection limit after antiviral treatment in three of these patients except one patient lost to follow-up. There were no cases of hepatic failure or death.
Table 3
Characteristics of patients who experienced HBV reactivation

HBV = hepatitis B virus, RA = rheumatoid arthritis, CHB = chronic hepatitis B, HBsAb = hepatitis B surface antibody, HBeAg = hepatitis B envelope antigen, HBeAb = hepatitis B envelope antibody, ALT = alanine aminotransferase, HCQ = hydroxychloroquine, SSZ = sulfasalazine, PD = predinosolone, MTX = methotrexate, TAC = tacrolimus, LC = liver cirrhosis, HCC = hepatocellular carcinoma.
DISCUSSION
In this study, we investigated the differences in disease characteristics, treatment patterns and changes in disease activity according to concomitant HBV infection. Although previous studies have described disease activity in RA with HBV infection, these studies were carried out at a single time point, examined use of specific drugs, or did not include a control group.181920 In translational research on patients with RA and concomitant hepatitis B infection, the functional activity of complement was further reduced in patients with hepatitis, and levels of complement were associated with the course of RA.21 Therefore, we conducted this study to determine whether HBV infection affects RA disease activity. To the best of our knowledge, this is the first study comparing differences in disease activity markers and treatment pattern according to HBsAg-positivity in RA patients using long-term follow-up data.
One study reported that HBV infection did not have any significant association with disease activity or joint destruction in RA.16 Similarly, our analysis of baseline disease activity data revealed no differences between HBsAg-positive and HBsAg-negative patients. On regression analysis of longitudinal data, RA disease activity had a significant negative correlation with time, which likely resulted from effective RA treatment during the study period. Of the markers representing disease activity, tender joint counts, ESR, and CRP levels showed no significant differences between groups, while swollen joint counts were significantly different. Although joint counts are used as the primary measure of disease activity of RA, a number of limitations of joint counts have been described in several publications.22 Joint counts may have more noise and more instability than would be expected due to poor reducibility.2324 Furthermore, joint counts showed relatively lower efficiency than global estimates and physical function in comparing active and control treatments in clinical trials.25 Thus, variation in swollen joint counts, without observed differences in any other measures, was not considered to indicate a meaningful difference in RA disease activity between HBsAg-positive and HBsAg-negative patients.
When all study visits were analyzed, methotrexate was prescribed significantly less frequently for HBsAg-positive patients. Such results were interpreted as reflecting real-world practice based on the ACR guidelines, in which methotrexate is contraindicated for CHB.2627 Sulfasalazine was used more frequently in HBsAg-positive patients because it was considered relatively safer than other DMARDs. Hydroxychloroquine was prescribed for almost all HBsAg-positive patients, but was also frequently prescribed for HBsAg-negative patients, and thus there was no significant difference between groups. The observed difference in combination therapy with conventional DMARDs according to HBsAg-positivity is likely related to the difference in drugs frequently used, as demonstrated in this study. Sulfasalazine and hydroxychloroquine are frequently used as a combination therapy because these drugs are thought to have less disease-modifying effects than methotrexate monotherapy. The use of systemic corticosteroids was similar in both groups, whereas the frequency of intraarticular corticosteroid injection was higher in the HBsAg-positive group. Intraarticular corticosteroid injection may have systemic effects, but the risk of HBV reactivation is substantially less than 1% of cases.2829 For this reason, local control using intraarticular corticosteroids seems to have been preferred in cases where systemic immunosuppressants are difficult to use, such as hepatitis B carriers.
The results of this study did not show any differences in the use of biologic agents based on the presence of HBsAg. However, since the number of patients included in the study was small, further studies are warranted on the effects of HBsAg positivity on biologic treatment. Recent retrospective studies have reported that biologic DMARDs are not significantly different from conventional DMARDs in terms of HBV reactivation with no significant differences in clinical outcomes even after HBV DNA reactivation.3031 However, one review did classify biologics such as TNF inhibitors as a high-risk group for HBV reactivation, so further large-scale studies are needed to confirm the effects of biologic agents on HBV reactivation.32
There were no statistical differences in serum transaminase level, according to HBsAg-positivity. These results suggest that safe treatment of RA is possible in patients with concomitant chronic HBV infection, if close monitoring of liver function and frequent assessment of hepatitis state are combined with treatment modification.
HBV reactivation was reported in 4 patients who were positive for HBV DNA at baseline. A high level of baseline HBV DNA is a risk factor for HBV reactivation after immunosuppressive therapy.173334 Previous studies demonstrated that preemptive antiviral therapy was effective in HBsAg-positive patients.63536 Current guidelines recommend that HBsAg-positive patients should receive preemptive antiviral administration during immunosuppressive therapy regardless of HBV DNA levels.373839 In this study, 37.5% of patients received antiviral therapy, lower than the expected proportion. There are two possible explanations for this situation. First, there is the problem of the expense of antiviral treatment, because Korean national health insurance does not cover preemptive use of antiviral agents. Second, in some patients, drugs with low hepatotoxicity, like hydroxychloroquine and sulfasalazine, were sufficient for control of disease activity and prophylactic antiviral medication was not necessary.
Among the 15 patients receiving antiviral agents, one patient experienced HBV reactivation. The patient who experienced reactivation while taking an antiviral agent showed poor compliance with the prescribed regimen, whereas no patients experienced HBV reactivation during adequate antiviral therapy. These results support previous publications, which described the increased HBV reactivation risk after discontinuation of antiviral agents.40 To maximize the effect of antiviral agent, medication adherence must be monitored and interventions to improve adherence should be considered.
Our study has several limitations that should be considered. First, since we conducted the study in a retrospective manner, the duration of follow-up and the interval of visits were quite variable, and some data were missing. For the detection of relationships, regression analysis using GEE models was conducted. GEE has several advantages in the analysis of longitudinal data, including that it allows the use of all available data. Second, patient-reported outcomes and global assessments were not included in analysis due to insufficient information. Differences in patient-reported outcomes according to concomitant HBV infection need to be addressed. Third, because this study was conducted at a single center and exclusion criteria were strictly applied, there are limitations with respect to generalizability. Nonetheless, the effect of chronic HBV infection itself was forcefully evaluated by excluding other comorbidities that may affect the treatment of RA.
In conclusion, our findings suggest that HBsAg-positivity affected the selection of medication to treat RA, but did not show a clear association with changes in disease activity. In RA patients with concomitant hepatitis B infection, safe and effective treatment of RA is possible through medication adjustment and close monitoring of liver function and disease activity.
 XML Download
XML Download