

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The increasing prevalence of osteoporosis is a major public health problem, especially in the elderly. The prevalence of osteoporosis in Korea is higher than that in most western countries1 and other Asian countries, including Japan2 and China.3 According to the 2008–2011 Korea National Health and Nutrition Examination Survey, the prevalence of osteoporosis is 38% in women and 7.3% in men aged 50 years and older, and the prevalence has been increasing annually.4 Osteoporosis was the third leading cause of quality-adjusted life-year loss in Korean women, following hypertension and arthritis.5
Bone mineral density (BMD) is associated with several serum inflammatory markers, including C-reactive protein (CRP)6 and T-cell derived cytokines, tumor necrosis factor-alpha (TNF-α) and interleukin (IL)-1.7 These studies suggested that an inflammatory response induces osteoclast formation, thereby leading to early bone loss and osteoporosis.67
Long pentraxin 3 (PTX3) is a novel inflammatory marker that belongs to the same superfamily of acute-phase reactants as CRP. PTX3 is thought to be associated with several inflammation-related diseases, including cardiovascular disease (CVD).8 Osteoporosis shares risk factors, such as aging, smoking, physical inactivity, alcohol intake, early menopause, and postmenopausal status, with the CVD.9 Common pathogenic traits, including inflammatory processes, might play a role in the development or progress of the diseases. There are genetic risk factors that are common to both CVD and osteoporosis.10 It can be hypothesized that the plasma PTX3 levels is associated with both osteoporosis and CVD. However, the association between PTX3 and BMD has not been evaluated epidemiologically. Therefore, we investigated the possible association between BMD and the plasma PTX3 levels in middle-aged and elderly Koreans who participated in a community-based cohort study.
METHODS
Subjects
The Dong-gu Study is an ongoing prospective study of the prevalence, incidence, and risk factors for chronic disease in Korean urban populations. Details of the study subjects and measurements have been published previously.11 Between 2007 and 2010, a total of 9,260 urban dwellers participated in the baseline examination. From these participants, a subcohort of 2,000 subjects (1,000 men and 1,000 women) was randomly selected for this analysis. After excluding 217 subjects (126 men and 91 women) who had incomplete BMD measurement data or a history of severe chronic disease, including myocardial infarction, stroke, and cancer, and 285 subjects who had history of regular calcium intake (82 men and 203 women), a total of 1,440 participants (757 men and 683 women) were included in the final analyses.
PTX3 assay
The plasma PTX3 concentration was determined using an enzyme-linked immunosorbent assay kit (Quantikine R&D International, Minneapolis, MN, USA), according to the manufacturer's protocol. This assay is a quantitative sandwich enzyme immunoassay technique. The assay was performed using plasma that had been stored frozen at −70°C and the PTX3 levels were all measured at the same time using reagents with the same lot numbers to reduce the measurement variability. According to the protocol, the intra-assay coefficient of variation (CV) was 3.93% and the inter-assay CV was 5.06% according to the protocol. The minimum detectable dose (MDD) of human PTX3 ranged from 0.007–0.116 ng/mL and the mean MDD was 0.025 ng/mL.
Measurements of BMD and other variables
BMD was measured in g/cm2 at the lumbar spine and femoral neck using dual-energy X-ray absorptiometry (Prodigy; GE, Madison, WI, USA). The lumbar spine BMD was calculated as the average BMD of L1–L4, and femoral neck as the average BMD of left and right femoral neck. For quality control, daily phantom scans were performed before the measurements. All BMD scans were performed by well-trained examiners using standardized procedures following the manufacturer's recommended protocols. The intra-scanner reproducibility of repeated measurements, expressed as the CV, was less than 1%. Details of the BMD measurement have been published previously.1213
Demographic factors, health habits (smoking status, alcohol consumption, and regular exercise), menopausal status, and calcium medication history for osteoporosis were assessed with a questionnaire survey. Details of the height and weight measurements have been described previously.11 Hemoglobin A1c (HbA1c) levels were analyzed by high-performance liquid chromatography using the VARIANT II system (Bio-Rad, Hercules, CA, USA). Fasting glucose, lipid profiles, and bilirubin were analyzed using enzymatic assays with an automatic analyzer (Hitachi-7600; Hitachi, Tokyo, Japan). High-sensitive serum CRP (hs-CRP) was measured by latex-enhanced nephelometry using a high-sensitivity assays analyser (Behring Nephelometer II; Dade-Behring Diagnostics, Marburg, Germany). The MDD of the assay for hs-CRP was 0.175 mg/L.
Statistical analysis
Differences in the demographic and clinical characteristics among the subjects were evaluated by χ2 or t-tests according to whether the variables were categorical or continuous. The standardized beta coefficient of the univariate linear regression was used to analyze associations with BMD involving continuous variables, including age, body mass index (BMI), waist-to-hip ratio (WHR), hs-CRP, white blood cell count (WBC), HbA1c, total cholesterol, triglyceride, high-density lipoprotein (HDL)-cholesterol, uric acid (UA), and total bilirubin. Multiple linear regression was used to evaluate the association between the plasma PTX3 levels and BMD. Conventional factors which were significantly associated with BMD in univariate model were all inserted into the multivariate model, including age, BMI, WHR, HbA1c, HDL-cholesterol, UA, and regular exercise. To correct the potential false positive error by the multiple comparison test, a P value < 0.025 was considered statistically significant in the multivariate model because we tested two sites of BMD simultaneously. The statistical analyses were performed using SPSS version 21 (IBM, Armonk, NY, USA).
RESULTS
The baseline characteristics of the 1,440 subjects are presented in the Table 1. The mean age was 66.0 ± 8.1 years for men and 63.7 ± 7.9 years for women. Among the 683 women subjects, most were menopaused (96.0%) and never smoker (95.6%). The respective mean BMIs, hs-CRPs, and WBCs were different (23.8 ± 2.7 kg/m2, 0.17 ± 0.46 mg/dL, and 6.07 ± 1.61 × 103/μL for men and 24.7 ± 2.9 kg/m2, 0.12 ± 0.24 mg/dL, and 5.62 ± 1.63 × 103/μL for women). The levels of total cholesterol, HDL-cholesterol, UA, and total bilirubin were also different between sexes. The mean BMD (g/cm2) at the lumbar spine and femoral neck was significant higher in men (1.157 ± 0.198 and 0.880 ± 0.127) than in women (0.998 ± 0.171 and 0.796 ± 0.125; P < 0.001). However, no difference was found in PTX3 levels (Table 1). PTX3 levels was significantly correlated with the other inflammatory markers, such as hs-CRP and WBC count (Table 2).
Table 1
Demographic and clinical characteristics of the subjects (n = 1,440)
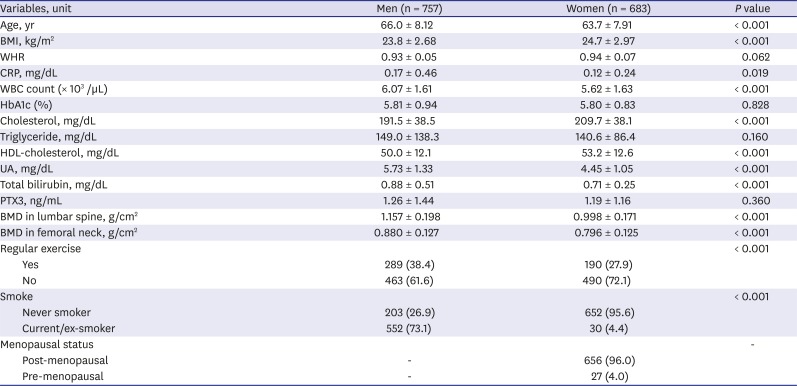
Table 2
Correlation of PTX3 with CRP and BMDs (n = 1,440)

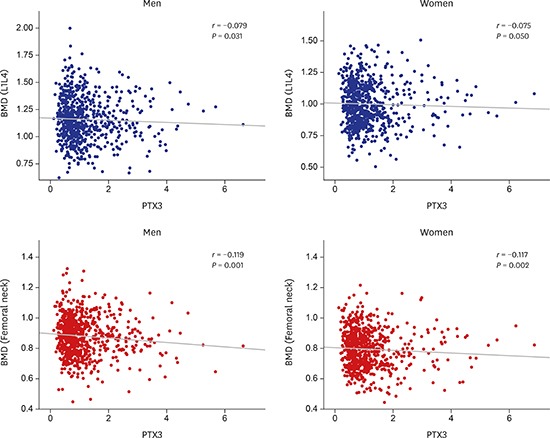
Table 3 shows the association of BMDs with continuous variables, including PTX3 levels, based on the linear regression. The BMDs in both sites were positively associated with BMI, WHR, and HbA1c for men and with BMI and UA for women (all P < 0.05). The BMD in either region was inversely correlated with the HDL-cholesterol and PTX3 in men. The WHR inversely associated with the femoral neck BMD for women (Table 3).
Table 3
The linear regression for the association between BMD and various clinical factors including PTX3
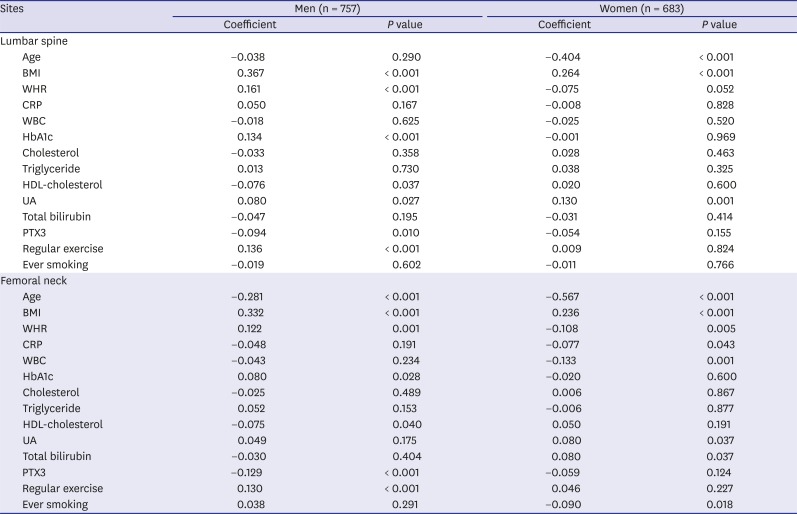
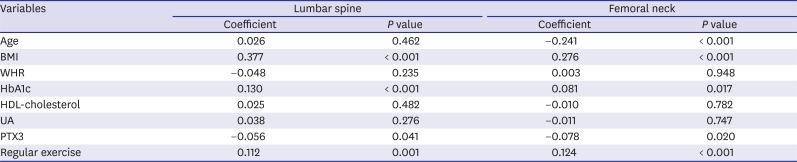
Table 4 shows the association between BMD and the PTX3 levels after adjusting for other factors by lumbar spine and mean BMD of right and left femoral necks for men. Significant inverse association was maintained for femoral neck after adjustment for multiple comparison test (P = 0.020). For women, no significant association was in both sites (Table 4). When we stratified the women by menopausal status, no significant association between BMD and the PTX3 levels was found in pre- or post-menopausal women (data not shown).
Table 4
The multivariate linear regression for the association between BMD and PTX3 levels in men subjects
DISCUSSION
This study evaluated the association between plasma PTX3 levels and BMD in a Korean population. To our knowledge, this is the first study to investigate the relationship between BMD and plasma PTX3 levels in a general population. We found a significant association between the PTX3 levels and the BMD in men, but no significant association was found in women.
PTX3, the prototype protein of the long pentraxin group, is an essential component of innate immunity that is produced by immune and vascular cells in response to pro-inflammatory signals. A homeostasis-related function of PTX3 in tissue repair and matrix remodeling has also been recognized.14 Persistent elevation of PTX3 levels is associated with disease severity and increased morbidity in diverse clinical pathological conditions, including atherosclerosis and cancer.15 A multiethnic cohort study found that PTX3 was associated with both CVD-related and all-cause mortality.8 However, the presence of PTX3 in bone-related cells and the role of PTX3 in bone-related diseases have not been elucidated.
Inflammation is a major cause of the bone homeostasis imbalance that results in excessive bone resorption. Some studies suggest that an inflammatory response induces the formation of osteoclasts, thereby leading to early bone loss and osteoporosis.16 Tumor necrosis factor-stimulated gene-6 (TSG-6), also known as TNFIP6, can regulate the expression of various molecules that have important roles in the control of inflammation.17 TSG-6 also interacts with a wide spectrum of glycosaminoglycan and protein ligands, including PTX3.18 This protein is induced by a number of signaling molecules, such as TNF-α and IL-1,19 and inhibits osteoclast activity by interacting with osteoprotegerin in bone.20 Therefore, PTX3 can potentially disrupt the function of TSG-6 and consequently promote bone loss in inflamed bone. It is also possible that PTX3 is secreted from osteoblasts and induces receptor activator of nuclear factor-κB ligand (RANKL) expression and production, thereby promoting osteoclast differentiation in the bone environment.
Therefore, we hypothesized that the serum PTX3 levels is associated with the BMD in the general population and analyzed the association between PTX3 and BMD using a community-based subcohort. Although, we found a correlation between PTX3 and BMD in lumbar spine and femoral neck, no significant association between PTX3 levels and BMD in women was observed in multivariate model. Furthermore, the association observed between PTX3 and BMD in lumbar spine in men was no longer statistically significant after multiple comparison adjustment. Several factors might explain the discrepancies by sex and site. First, Menopausal status has a dominant impact on BMD and could mask the effect of the PTX3 levels in postmenopausal women. For men, there is no dominant determinant of BMD like menopause for women. Second, effect of inflammation on bone formation may be influenced by skeletal load and protective effect of estrogen produced by adipose tissue. The gender difference in the association between inflammatory markers and BMD may relate to different interaction with these potential mediators in the causal pathway between inflammation and BMD across the sexes. In our data, PTX3 was reversely associated with BMI in men, but not in women subjects. This gender difference in the association of inflammatory marker with BMD is consistent with data from a previous study,21 but inconsistent with the findings from other studies.2223 Third, measurement errors are more common for the lumbar BMD than the femoral neck BMD because of severe osteolytic change or osteophyte body compression in elderly subjects.24 This osteoarthritis with osteophyte formation may mask bone loss in lumbar spine.25 As a result, the femoral neck has better validity for BMD measurements than the lumbar spine. Consequently, an association between BMD and PTX3 was found only in men and only for the femoral neck. It is necessary to increase the number of samples or to measure premenopausal women. The association of inflammatory markers with risk of osteoporotic fracture has been also evaluated in many studies, but the findings were still inconsistent with discrepancies between different population or genders or markers.2126272829 In our study, the proportion of subjects who reported their non-traumatic fracture history is significantly increased with higher PTX3 levels (data not shown). The finding suggests that the PTX3 levels may be associated with the risk of non-traumatic fracture but cannot confirm the causation due to the uncertainty of the temporal relationship.
The main strengths of this study are that the subjects were selected randomly from participants in a large community-based cohort. Consequently, the findings are more generalizable than findings from hospital-based studies. We measured the plasma PTX3 levels using same reagent lot numbers, which should reduce the PTX3 measurement error. This study also has several limitations. First, the age distribution of the study subjects was skewed to the elderly. Because most of the women studied were postmenopausal (96%), the characteristics of premenopausal women were not reflected in the findings. Second, residual confounding might have affected the main results and contributed to the relatively weak levels of significance because the results were not adjusted for all potential confounders, such as family history of osteoporosis or alcohol cirrhosis, dietary habits, and use of osteoporosis medication. Third, this study cannot be used to determine negative causal relationships because of its cross-sectional design and low statistical power due to relatively small sample size, especially in multivariate analyses.
In conclusion, there was inverse correlation between plasma PTX3 levels and BMD both in the lumbar spine and femoral neck in men, but the associations were weakened in the multivariate model, especially for the region of lumbar spine. Further prospective studies with large study subjects need to confirm the association between PTX3 and BMD, or examine the functional and clinical relevance of the plasma PTX3 levels and BMD.
 XML Download
XML Download