

 PDF
PDF Citation
Citation Print
Print



A 54-year-old female, who had a 12-year history of end-stage renal disease on hemodialysis, was referred to our clinic for aggravating dyspnea (January 23, 2018). Although parathyroidectomy was recommended due to secondary hyperparathyroidism 3 years ago, the patient refused surgery at diagnosis and parathyroidectomy was performed 1 month before admission to our clinic.
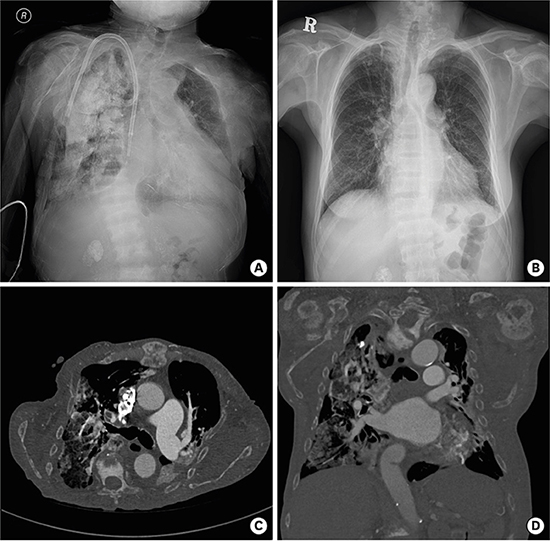
Chest radiography showed diffuse fluffy opacities in right lung (Fig. 1A). Diffuse osteosclerotic and osteolyitic changes were noted in the thorax. Review of an old chest radiography obtained two years ago showed multiple small dense calcified nodules in right apex (Fig. 1B). These chest radiographic findings were suggestive of progressive pulmonary calcification.
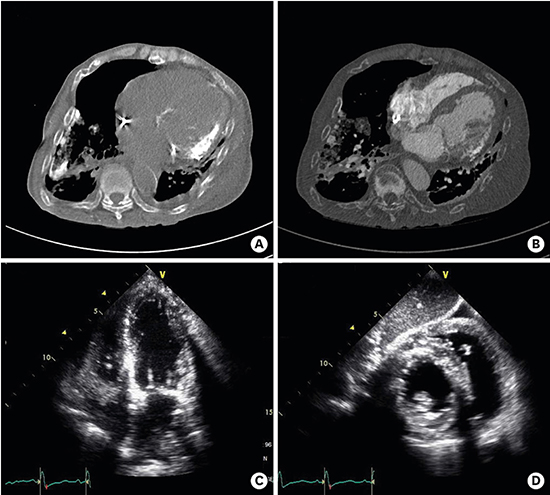
Chest computed tomography (CT) revealed diffuse fluffy ground-glass centrilobular opacities with calcifications in the right lung. The thorax, both shoulder joints and vertebrae showed diffuse osteosclerotic and osteolyitic changes (Fig. 1C and D). Extensive bone growth with demineralization was noted on the mandible, suggesting uremic leontiasis ossea. Lateral wall and basal septum of left ventricle (LV) were radio-opaque, suggesting calcified myocardium (Fig. 2A and B).
Echocardiography revealed decreased LV systolic function with regional wall motion abnormalities. The regional wall motion abnormalities were not correlated with coronary territories. Hypokinetic segments, basal interventricular septum, anterior walls and posterolateral walls of LV, showed diffusely hyperechoic with scattered densities. Acoustic shadowing were present distal to hyperechoic myocardium (Fig. 2C and D). To rule out myocardial ischemia, coronary angiography was performed and revealed normal coronary arteries. Fluoroscopy showed a radio-opaque myocardium.
Vascular and cardiac valve calcification are common in patients with end-stage renal disease.12 In patients with end-stage renal disease, alteration in calcium and phosphorus metabolism and persistent elevations in plasma parathyroid hormone are thought to be additional contributors for cardiovascular calcification. Optimal treatment for secondary hyperparathyroidism could diminish the progression of cardiovascular calcification.3 Myocardial calcification is an extremely rare, but possible case in patients with uncontrolled secondary hyperparathyroidism. To our knowledge, this case of myocardial calcification in a patient with end-stage renal disease is the first in the literature. Owing to delayed treatment of secondary hyperparathyroidism, extensive calcification including myocardial involvement developed in the present case.
In the present case, uncontrolled secondary hyperparathyroidism resulted in calcified LV myocardium. For preventing cardiovascular complications, close monitoring and optimal treatment for secondary hyperparathyroidism are also needed in patients with end-stage renal disease.
 XML Download
XML Download