

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The incidence of atrial fibrillation (AF), the most common type of clinically significant cardiac arrhythmia, has increased over the last decade.1 AF is associated with high medical costs, as well as an increased risk of ischemic stroke and death.2 Although the precise mechanisms involved in AF are not well understood, a growing body of evidence indicates that inflammation and the autonomic nervous system are involved in the pathogenesis of AF.345 Clinical and experimental studies have suggested that AF triggers and drivers in the pulmonary veins and left atrial wall are at least partially modulated by the autonomic nervous system.6
Herpes zoster (HZ) is caused by reactivation of the latent varicella-zoster virus (VZV) in the cranial nerve, dorsal root, or autonomic ganglia with spread of the virus along the sensory nerve to the dermatome producing radiculoneuritis and cutaneous manifestations. Unvaccinated persons over 85 years of age have a 50% risk of developing HZ.78 HZ may result in serious neurologic or inflammatory sequelae and severe cases often require hospitalization (up to 3% of HZ cases).9 The neurologic sequelae of HZ is well-known, and can result in autonomic dysfunction1011 The vagus nerve or its ganglia can be involved in HZ, resulting in dysphagia, nausea, vomiting, gastric upset, or cardiac irregularities.12
According to the pathogenesis of the two diseases, AF can occur as a complication of HZ, but the relationship between AF and HZ has not been studied widely. We hypothesized that HZ may be associated with AF development.
METHODS
Study population
From the Korean National Health Insurance Service (NHIS) database, we used a random multistage representative sample of 1,034,777 people. Consequently, a total of 738,559 subjects were selected for analysis after patients less than 20 years of age and patients who had been treated for either AF or HZ during the screening period (2002–2004) were excluded. Newly diagnosed HZ patients (n = 30,685) were identified using health insurance claims data from 2005 to 2011. We defined the date on which each patient was first diagnosed with HZ as the index date. On the same index date, four age- and sex-matched non-HZ control subjects (n = 122,740) were selected for each HZ patient. A flowchart of the patient enrollment process is shown in Supplementary Fig. 1. Follow-up data was obtained up to 2013.
Database
Records from the NHIS database included patients' sociodemographic information, their use of inpatient and outpatient services, and pharmacy dispensing claims. The majority (97.1%) of the Korean population (approximately 50 million people) is covered by the mandatory NHIS. Diagnoses were confirmed using the International Classification of Disease, Tenth Revision, Clinical Modification (ICD-10-CM) codes. In the present study, multistage sampling was performed, and we used a random sample of one million people selected from the NHIS database. The staff of the NHIS confirmed that the study cohort was a representative sample of the general Korean population for the period 2002 to 2013.13
Definition
Instances of newly diagnosed AF (I480–I484, I489) identified during follow-up were analyzed as in our previous studies1415 and the HZ and non-HZ group were compared. Patients who were diagnosed with mitral stenosis (I050, I052, and I059) or those who had mechanical heart valves (Z952–Z954) implanted from 2002 to 2013 were excluded from the analysis.
The presence and severity of HZ was determined on the basis of diagnostic and procedure codes recorded during the study period from 2005 to 2011. A HZ patient was identified by the diagnostic code for HZ (B02) and received either oral anti-viral medication for at least five days, or an anti-viral injection more than once. Hospitalization due to HZ was obtained from the database. A newly diagnosed HZ patient requiring simultaneous hospitalization was defined as a severe HZ case. The remaining HZ patients, who were treated as outpatients, were considered mild HZ cases. The epidemiology of HZ in Korea has been previously reported using NHIS database records.16
Statistical analysis
Baseline characteristics are presented as mean and standard deviation, or numbers and percentages. The differences between continuous values were assessed using an unpaired two-tailed t-test for normally distributed continuous variables and a Mann-Whitney rank-sum test for skewed variables. The χ2 test was used for the comparison of nominal variables. We used risk set sampling for selection of the age- and sex-matched control subjects. Incidence rates were described as the number of events per 1,000 patient-years (PTPY). Hazard ratios (HRs) and the corresponding 95% confidence intervals (CIs) were calculated using Cox proportional hazard models. Comparison of cumulative event rates between HZ and non-HZ groups was based on Kaplan-Meier censoring estimates and performed with the log-rank test. Crude risks were analyzed in the overall cohort, and adjusted results were subsequently calculated with the multivariable Cox regression analyses. Subgroup analyses of multiple cardiovascular risk factors were subsequently performed. The level of statistical significance was set at P < 0.05, and all statistical analyses were performed using SAS version 9.3 (SAS Institute, Cary, NC, USA) and SPSS (IBM® SPSS® Statistics version 22; IBM Corp., Armonk, NY, USA).
RESULTS
Baseline characteristics
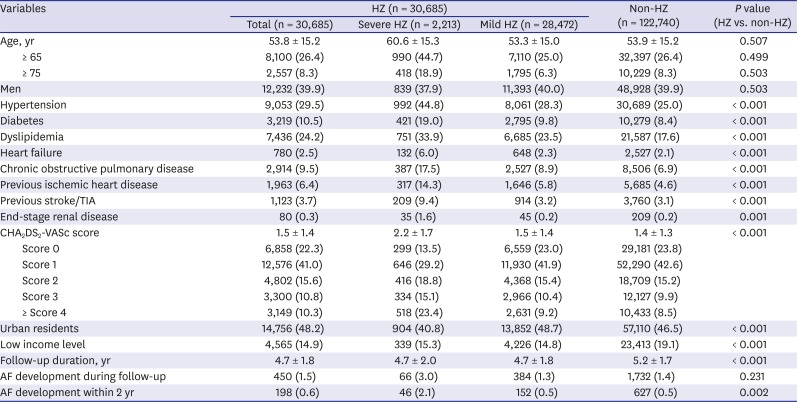
A total of 153,425 adults (aged over 20) with no history of AF or HZ were analyzed. The baseline characteristics and demographic features of patients according to HZ severity are described in Table 1. The mean age of the total study population was 53.8 ± 15.2 years, and 60.1% of the patients were female. The HZ group had significantly more comorbidities than the non-HZ group, and the severe HZ group had the highest CHA2DS2-VASc score of all three groups. A total of 2,204 (1.4%) patients were diagnosed with new AF, and among them 825 (0.5%) patients were diagnosed within two years of their index (diagnosis) date.
Table 1
Baseline characteristics of patients with or without HZ
Relative risk of AF development according to HZ severity
The HZ group showed a higher incidence of AF than the non-HZ group. The number of events, calculated incidence rates, and unadjusted and adjusted HRs for AF and stroke according to HZ severity are described in Table 2. Those with severe HZ were at significantly higher risk of developing AF (n = 66, 6.4 per 1,000 PTPY) compared to those with mild HZ (n = 384, 2.9 PTPY) and the non-HZ group (n = 1,732, 2.7 PTPY) (Fig. 1A). In a landmark analysis (Fig. 1B), the risk of developing AF was significantly greater for severe HZ cases in the two-year period following HZ diagnosis; however, after the two-year period, the relative risk of developing AF did not differ significantly in the three groups.
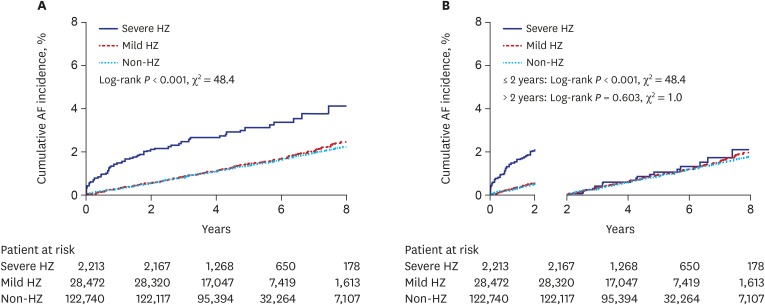
Table 2
Association between HZ severity and AF
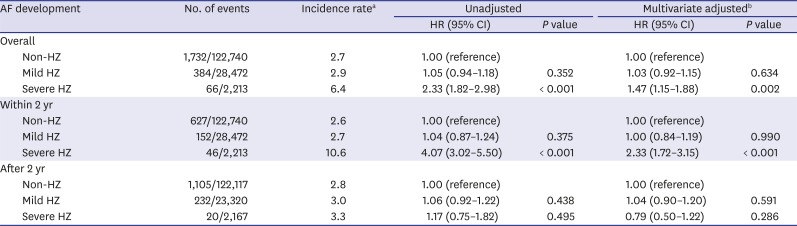
HZ = herpes zoster, AF = atrial fibrillation, HR = hazard ratio, CI = confidence interval.
aIncidence rates were calculated per 1,000 patient-years, within the population who were over 20 years old and not previously diagnosed with AF; bMultivariate adjusted hazard ratios were calculated by Cox regression models, including income level, resident area, CHA2DS2-VASc score as covariates.
Severe HZ vs. mild HZ or non-HZ patients
We re-grouped the patients into two groups: a severe HZ group and a control group (mild HZ plus non-HZ patients). We did this because the overall incidence of AF was not significantly different for mild HZ patients and the non-HZ group. The baseline characteristics of the two groups are described in Supplementary Table 1. The overall cumulative incidence of AF in the severe HZ group and in the control group within the two-year period following HZ diagnosis, was 3.0% and 1.4%, respectively (HR, 2.30; 95% CI, 1.81–2.95; P < 0.001). Analysis after adjustment for CHA2DS2-VASc score and socio-economic status (income status and residence) showed the same results as the original analysis (HR, 1.46; 95% CI, 1.14–1.87; P = 0.003 in the severe HZ group). The detailed data is shown in Supplementary Table 2 and Supplementary Fig. 2. The risk of AF development was more pronounced in the two-year period following HZ diagnosis in the severe HZ group.
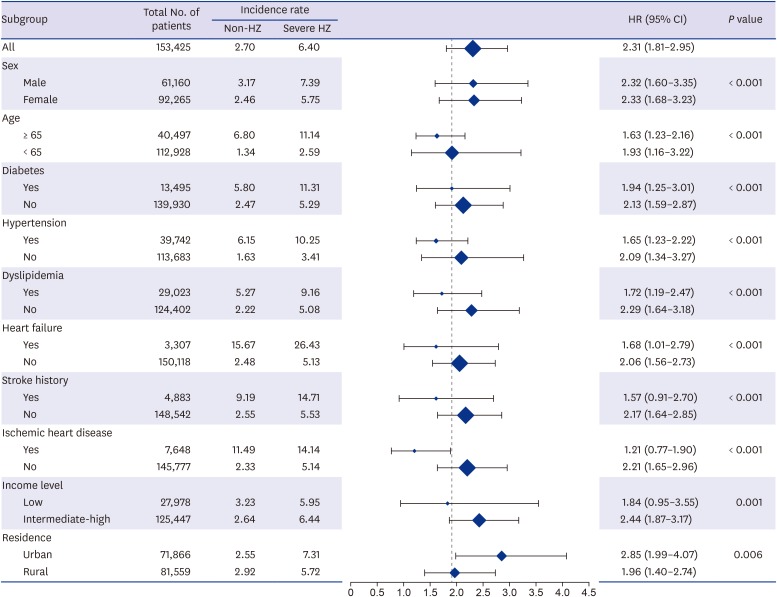
Subgroup analyses
Formal testing for interactions showed that the overall AF development rates in the severe HZ group and the control group were consistent across multiple subgroups (Fig. 2). Across the two subgroups defined by CHA2DS2-VASc (cut-off score of 3), the risk of AF development was significantly higher in the severe HZ group (Supplementary Tables 3 and 4). The relationship between AF and HZ was strong in the first two years after diagnosis.
Propensity score matched analysis
Although age and sex were matched between HZ and non-HZ group, the patients with HZ had more comorbidities. Therefore, we performed 1:2 propensity score matching, and the demographic features of matched population is demonstrated in Supplementary Table 5. A comorbidity and socioeconomic status (hypertension, diabetes, dyslipidemia, previous stroke/transient ischemic attack [TIA], heart failure, end-stage renal disease, chronic obstructive pulmonary disease, previous ischemic heart disease, low income level, and urban residence) in addition to age and sex between HZ and non-HZ group were matched. Kaplan-Meier curve from the propensity score matched cohort according to HZ severity are presented in Supplementary Table 6 and Supplementary Fig. 3. In accordance with overall cohort analysis, the risk of AF development was more obvious 2 years after HZ diagnosis, while the relative risk of AF after 2 years from index date among three severity groups were not significantly different.
DISCUSSION
In our nationwide case-control cohort study, we found an association between HZ and the development of AF. The main finding was that patients with severe HZ requiring hospitalization have an increased risk of incident AF within the two-year period following HZ diagnosis.
Inflammatory process is a well-established pathogenic process in exacerbated atherosclerosis. Many studies have supported a close link between AF and inflammatory processes. A high incidence of AF in patients after cardiac surgery, a well-known state of intense inflammatory process was reported.1718 Furthermore, an elevated serum C-reactive protein level has been reported to be related to AF development, increased AF burden, and higher recurrence rates after catheter ablation and electrical cardioversion for AF.19 Previous studies have demonstrated that a higher interleukin (IL)-6 level is associated with a higher risk of incident AF following coronary artery bypass graft surgery20 and a higher AF recurrence rate following cardioversion.21 The nationwide population based study on Herpes simplex infection reported that the viral inflammatory disease could be associated with an increased risk of AF.22 Bacterial infections such as Helicobacter pylori and Chlamydia pneumoniae have also shown an association with the occurrence of AF.23 However, there has been no population-based epidemiology study on the association between VZV and AF. Given that HZ involves a chronic latent inflammation, there is a strong possibility that it is associated with AF.
The intrinsic cardiac autonomic nervous system plays a critical role in the initiation and maintenance of AF, and sympathovagal discharges are common triggers for paroxysmal AF.24 There are many ganglionic plexuses around the atria, which is markedly influenced by cholinergic as well as sympathetic innervation.25 Changes in autonomic tone before the onset of paroxysmal AF have been reported, suggesting autonomic dysfunction may lead to the development of AF.26 HZ can involve nerve ganglia, resulting in autonomic dysfunction. Alternatively, VZV reactivations may cause the neuritis of the sympathetic and autonomic ganglia. HZ is reported to affect the autonomic nervous system of the colon due to the centripetal spread of the virus from the dorsal ganglion.27 In addition, the vagus nerve or its ganglia can be involved in HZ, resulting in cardiac irregularities.12 The reactivation may involve multi-loci, including dermatome and symptomatic ganglia that innervate the heart, leading to cardiovascular disease. The immune response has been shown to play an important role in the ganglia during VZV reactivation. Unfortunately, we could not find direct evidence that HZ involves cardiac ganglionic plexuses. Based on the literary evidence cited above, we assumed that HZ might lead to AF development via cardiac autonomic nervous system involvement.
To our knowledge, this is the first report to prove an increased risk of developing AF in the early period after a particular infection. The development of AF shortly after infection may be associated with HZ. In our cohort, about two percent of patients developed newly diagnosed AF within two years of HZ diagnosis, and this difference made the overall risk difference. AF can be asymptomatic and delayed diagnosis is common in real world clinical situations, thus the risk of incident AF may actually be higher within the short-term period following HZ diagnosis.
Because of the increasing incidence of AF and the ever-increasing public health burden it produces, significant efforts have been made recently in both risk factor identification and modifications for AF prevention. A number of traditional risk factors for AF have been identified, many of which are also associated with cardiovascular diseases, and the common preventive strategies focus on conventional modification of cardiovascular risk factors such as obesity, glucose control, blood pressure control, etc.
Furthermore, given that HZ is an inflammatory disease involving the nervous system, it can be prevented with vaccination.28 A significant proportion of AF cases could be prevented by HZ vaccination, and this has potential to dissipate the medical socio-economic burden.
One of the highlights of this study is the large comparison cohort stratified by age and gender. The effects of diabetes, hypertension, and hyperlipidemia on cardiovascular diseases were able to be adjusted according to the Cox proportional hazards. Subgroup analyses were performed to ensure the consistency of the results. However, several limitations of the present study remain. First, personal information such as smoking habits, physical activity, and body mass index were not available from this registry database. In addition, echocardiographic parameters, such as left atrial dimension and left ventricular ejection fraction, or electrocardiographic results were absent. Therefore, we were not able to control effectively for all potential confounders, although we have tried to adjust for important comorbidities in the Cox regression model. Second, HZ was diagnosed using ICD-10-CM codes and was not confirmed by molecular biological detection. The accuracy of HZ diagnosis could not be fully ascertained. Third, selection bias due to hospitalization might affect the detection rate of AF. Routine ECG screenings during hospitalization might increase the chance of detection of AF, so hospitalized severe HZ patients would have more chance to detect AF than non-hospitalized control group. However, we found that the incident AF occurred consistently during 2 years after diagnosed with HZ, and there is little chance to admit for 2 years due to HZ. Although there might be selection bias during early admission period in severe HZ patients, consistent occurrence of AF during 2 years of follow-up after HZ development would support our final conclusion. Lastly, while we reported a significant association between AF and HZ, these results were derived from an observational database. As we were not able to conclude whether HZ was the direct cause of the increased AF incidence, a further prospective and large-scale trial is necessary to confirm the findings of the present study.
Our results suggest that severe HZ requiring hospitalization is a possible risk factor for AF, and that AF incidence is greater for severe HZ patients in the two-year period following HZ diagnosis.
 XML Download
XML Download