

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Computed tomographic angiography (CTA) offers excellent visualization of small vascular details, enabling the detection of small aneurysms.12 However, after treatment such as surgical clipping or endovascular coil embolization, the evaluation of intracranial vessels is hampered by beam-hardening and photon starvation artifacts caused by the metallic implants.345 Beam-hardening is caused by the increase in mean energy transmitted when the beam passes through an object due to preferential absorption of lower-energy protons. Photon starvation refers to the decreased number of photons that reach the detector due to the attenuation of the X-ray beam after passing through high-atomic-number materials such as metal or bone.4 The combination of these two artifacts produces streak artifacts, observed as alternating dark bands obscuring the surrounding area on computed tomography (CT) images.
To manage this issue, adjustments of CT scan parameters, such as increasing the tube voltage and current, reducing the collimation and field-of-view, and the application of a dedicated reconstruction kernel, may be helpful.67 Surgical clips positioned perpendicular to the scan plane produce fewer artifacts.7 In addition, several techniques have been proposed to reduce the metal artifact on CT, including the monoenergetic processing of dual-energy CT data; sinogram inpainting methods; and iterative, statistical, and filtering methods.89 Several studies have found that metal artifact reduction (MAR) is useful for CTA or flat-panel detector CT in patients with intracranial metallic implants.10111213
The metal artifact reduction for orthopedic implants (O-MAR; Philips Healthcare, Best, the Netherlands) is a commercial iterative reconstruction method intended to reduce metal artifacts on conventional CT.14 The O-MAR is based on an iterative algorithm that generates a metal-only image from the metal sinogram and subtracts it from the original input image. This process is repeated until no large clusters of metal pixels are present in the resulting image. To date, several studies have evaluated its ability to reduce the metallic artifacts in various target lesions.1516171819 However, to the best of our knowledge, no study has investigated the effectiveness of the O-MAR in patients with intracranial metallic implants. The purpose of this study was to qualitatively and quantitatively evaluate the effects of the O-MAR on brain CTA images in patients with aneurysm clips and coils.
Go to : 
METHODS
Subjects
Thirty-six consecutive patients (14 men and 22 women; mean age, 58.0 years; range, 38–80 years) who underwent brain CTA scanning after undergoing surgical clipping or endovascular coil embolization for intracranial aneurysm from December 2013 through January 2016 were enrolled in this study.
Image acquisition
All CTA images were obtained with a 128-channel multidetector CT scanner (Ingenuity; Philips Healthcare). The following CT parameters were used: tube voltage, 120 kVp; effective tube current-time product, 50–300 mAs; detector configuration, 0.625 mm; pitch, 1.172; rotation time, 0.4 s; matrix, 512 × 512; slice thickness, 0.9 mm; reconstruction interval, 0.45 mm. CT images were obtained in the unenhanced and arterial phases. All patients received 100 mL of Optiray 350 (Ioversol; Mallinckrodt, Hazelwood, MO, USA) followed by a 30-mL saline flush injected at a rate of 4.5 mL/s using a power injector. All CT images were reconstructed with an iterative reconstruction algorithm at level 2 (iDose2). The iDose2 images were processed without the O-MAR (hereafter referred as non-O-MAR images) or with the O-MAR (hereafter referred to as O-MAR images).
Image analysis
Two qualified neuroradiologists (L.S. and S.W.P.) of 8 and 23 years of clinical experience, respectively, independently reviewed the images. The axial non-O-MAR images and O-MAR images were reviewed while displayed side-by-side.
Qualitative analysis
The images were evaluated for the degree of streak artifacts and the confidence in the depiction of the surrounding vessels for each metallic implant. In addition, the presence of new streak artifacts on O-MAR images was assessed. The degree of streak artifacts was graded using the following scale: 1) no streak artifact; 2) mild streak artifact that does not interfere with the depiction of adjacent structures; 3) moderate streak artifact that mildly impairs the depiction of adjacent structures; and 4) severe streak artifact that significantly impairs the depiction of adjacent structures. The confidence of the surrounding vessel depiction was evaluated on the following 3-point scale: 1) no loss of adjacent vessel density; 2) some loss of adjacent vessel density, but diagnostic; and 3) significant impairment of adjacent vessel interpretation.
The reviewers also evaluated the presence of new artifacts on the following scale: 1) no new streaks; 2) new streaks that do not interfere with the interpretation of adjacent structures; and 3) new streaks that impair interpretation. To assess the influence of two or more metallic objects on the same axial plane, the number of cases with overlapping objects and the presence of new artifacts in each case were recorded.
Quantitative analysis
Circular regions of interest (ROIs) approximately 25 mm2 in size were manually placed in both non-O-MAR and O-MAR images at the following areas: immediate vicinity of the clip or coil mass, adjacent brain parenchyma, bilateral temporalis muscle, and air outside the cranium at the level of metallic implant (Fig. 1). ROI for immediate vicinity of the clip or coil mass was placed within 5 mm distance from the metallic object, where the streak artifact was severest. For clips, the ROI was placed at the areas just next to the head or tail portions of the clip along its long axis. ROI for adjacent parenchyma was placed at the nearby brain parenchyma, farther than 10 mm from the metallic object. The mean CT number and the standard deviation (SD) (i.e., image noise) of each ROI were recorded.
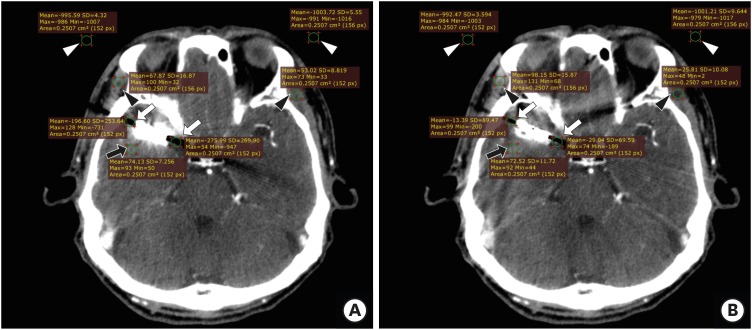 | Fig. 1Locations of the ROIs used for image analysis. Circular ROIs approximately 25 mm2 in size were placed on (A) non-O-MAR images and on (B) O-MAR images at the following areas: immediate vicinity of the clip or coil mass (white arrows), adjacent brain parenchyma (black arrows), bilateral temporalis muscle (black arrowheads), and the air outside the cranium at the level of the metallic implant (white arrowheads).
ROIs = regions of interest, O-MAR = metal artifact reduction for orthopedic implants.
|
Statistical analysis
The qualitative and quantitative variables of the non-O-MAR and O-MAR images were compared using a Wilcoxon signed rank test. The frequency of the variables was compared using a Fisher's exact test. Kappa (κ) statistics with linear weighting and intraclass correlation coefficients (ICCs) were used to assess interobserver agreement. The κ and ICC values of < 0, 0–0.20, 0.21–0.40, 0.41–0.60, 0.61–0.80, or > 0.81 indicated negative, positive but poor, fair, moderate, good, or substantial agreement, respectively. Statistical analyses were performed using MedCalc (version 17.6; MedCalc Software, Mariakerke, Belgium). P values < 0.05 were considered significant.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Seoul Metropolitan Government-Seoul National University Boramae Medical Center (approval No. L-2014-165). The requirement for informed consent was waived.
Go to :
RESULTS
Subject characteristics
A total of 47 treated aneurysms (42 clips and 5 coils) of 36 patients were analyzed. The locations of the aneurysms were the distal internal carotid artery (including the origins of the posterior communicating artery, superior hypophyseal artery, and anterior choroidal artery; n = 8; 19.0%), anterior cerebral artery (n = 13; 27.7%), and middle cerebral artery (n = 26; 55.3%). Twenty-seven patients had a single aneurysm, seven patients had double aneurysms, and two patients had triple aneurysms. The clips of known types were titanium and were 3–9 mm in length. Ten patients who had undergone surgery at an outside hospital had clips of unknown types. All coils were made of platinum.
Qualitative analysis
The results of the qualitative analysis are summarized in Table 1. The degree of streak artifact and the confidence in the surrounding vessel depiction were not significantly improved with the use of the O-MAR. The overall interobserver agreements were good to substantial.

Table 1
Comparison between qualitative variables of O-MAR and non-O-MAR images
O-MAR = metal artifact reduction for orthopedic implants, CI = confidence interval.
aValues in parentheses are interquartile ranges.
![]()
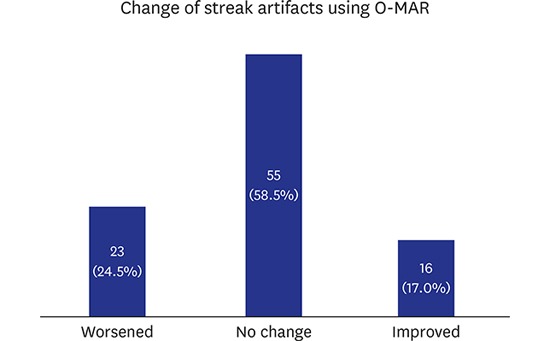
Improvement of implant-induced streak artifacts was noted in 8 objects (17.0%, 8/47). However, streak artifacts were aggravated in 11 objects (23.4%, 11/47), and adjacent vessel depiction was worse in 8 objects (17.0%, 8/47). New streak artifacts were noted in 32 objects (68.1%, 32/47). Of 94 interpretations by the two reviewers, 27 objects (28.7%, 27/94) were accompanied by impaired interpretation. All coils (n = 5) on non-O-MAR images showed extensive streak artifacts. However, improvements in the streak artifacts were noted in 60% (6 of 10 interpretations) of the coils, and none showed aggravation of streak artifacts. Overall, a significant difference was observed between the clips and coils regarding streak artifact improvement (P = 0.002) (Figs. 2 and 3).
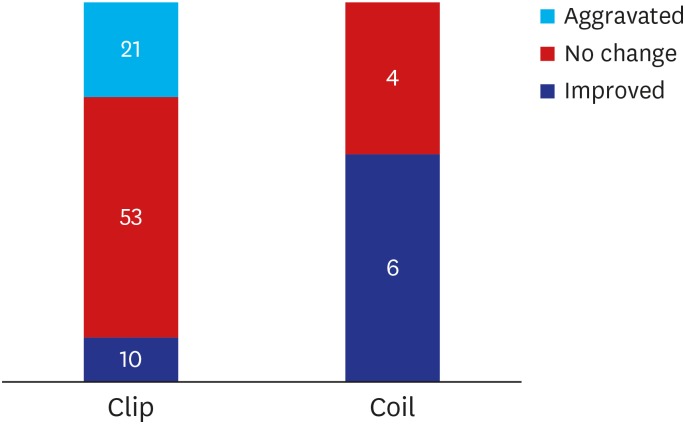 | Fig. 2Streak artifact improvement in clips and coils using O-MAR. The streak artifact improvement was significantly more evident in clips compared to coils (P = 0.002).
O-MAR = metal artifact reduction for orthopedic implants.
|
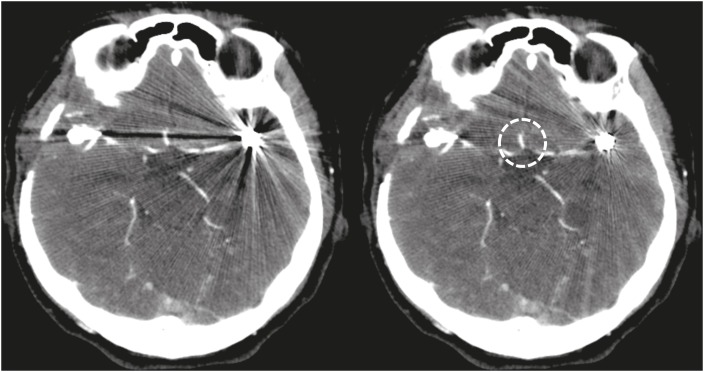
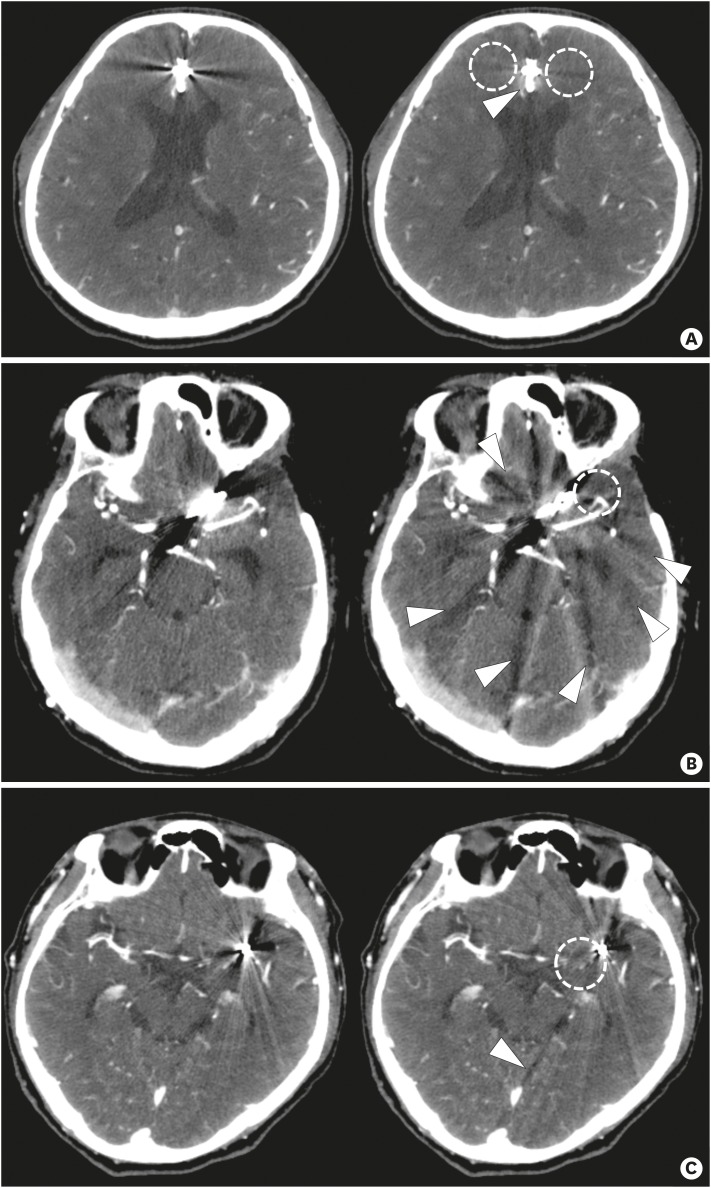 | Fig. 3Non-O-MAR (left) and O-MAR (right) images in the representative cases. (A) A surgical clip at right A2/3 junction in a 71-year-old male patient. The O-MAR image shows improved streak artifact (dashed circles), although a vessel is slightly less clearly depicted (arrowhead). (B) A 68-year-old male patient who underwent surgical clipping for an anterior communicating artery aneurysm. The O-MAR image shows multiple bands of worsened streak artifacts (arrowheads), while there is a focal area with improved streak artifacts (dashed circle). (C) A 73-year-old male patient who underwent coil embolization for an aneurysm at the left middle cerebral artery bifurcation. The streak artifacts are slightly improved on the O-MAR image (particularly in the dashed circle area), but there is a focal aggravation of streak artifact (arrowhead).
O-MAR = metal artifact reduction for orthopedic implants.
|
In addition, we noted that 2 or more metallic implants were present in one axial image in 21 patients (58.3%, 21/36). New streak artifacts were significantly more prevalent in these cases than in cases without coexistent metallic objects in one axial image (P = 0.018) (Table 2). Of note, in 2 cases in which a clip and a coil mass were coexistent on an axial image, the O-MAR improved the streak artifact and the depiction of the vessels (Fig. 4).

 | Fig. 4Non-O-MAR (left) and O-MAR (right) images of a 48-year-old female patient who underwent coil embolization and surgical clipping. The clip at the right middle cerebral artery bifurcation and the coil mass at the left middle cerebral artery bifurcation are present on the same axial image. The streak artifact is markedly improved on the O-MAR image. In addition, a branch of the anterior cerebral artery is more clearly depicted using the O-MAR (dashed circle).
O-MAR = metal artifact reduction for orthopedic implants.
|
Table 2
Effect of coexistent metallic implants on the same axial plane
| Grade of new streak artifact | No coexistent objects (n = 15) | Two or more coexistent objects (n = 21) | Total (n = 36) |
|---|---|---|---|
| Grade 1 | 7 | 2 | 9 |
| Grade 2 | 7 | 11 | 18 |
| Grade 3 | 1 | 8 | 9 |
New streak artifacts were graded on a 3-point scale: 1) no new streaks; 2) new streaks that did not impair the interpretation of adjacent structures; and 3) new streaks that impaired interpretation.
![]()
Quantitative analysis
The results of the quantitative analysis are presented in Table 3. For all ROI locations (immediate vicinity of the metallic implant, adjacent parenchyma, temporalis muscle, and extracranial air), the median CT number was not significantly different between the non-O-MAR and O-MAR images. In contrast, the image noises (SD of the ROI) in the immediate vicinity of the metallic implant and the extracranial air were significantly lower in O-MAR images than in non-O-MAR images in both the precontrast and postcontrast phases (all, P = 0.001 or P < 0.001). In addition, the image noise of the temporalis muscle was only significantly lower for the postcontrast phase of O-MAR images compared to non-O-MAR images (P = 0.015). The image noise in the adjacent parenchyma was not significantly different between non-O-MAR and O-MAR images. The ICC values of areas near the metallic implants ranged from 0.82 to 0.99, suggesting substantial agreement. The interobserver agreements of all but one remaining values were good to substantial; the exception was the image noise of the extracranial air, which ranged from fair to moderate.
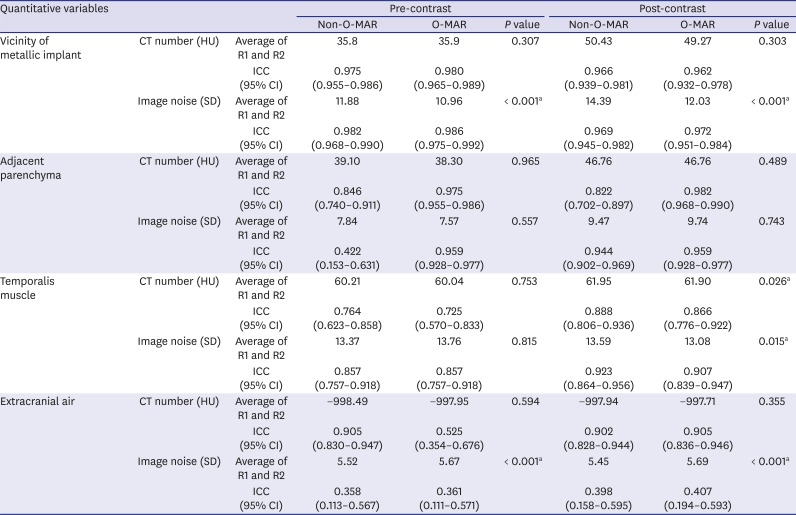
Table 3
Comparison of the quantitative variables in O-MAR and non-O-MAR images
O-MAR = metal artifact reduction for orthopedic implants, CT = computed tomography, HU = Hounsfield unit, SD = standard deviation, ICC = intraclass correlation coefficient, CI = confidence interval, R1 = reviewer 1, R2 = reviewer 2.
aStatistically significant results.
![]()
Go to :
DISCUSSION
In the present study, image noise, represented by the SD of the ROI, was significantly reduced on O-MAR compared to non-O-MAR images in the immediate vicinity of the metallic object. Reduced streak artifacts were noted in 17.0% of the metallic implants when O-MAR was applied. However, the overall degree of the streak artifacts and the confidence of the surrounding vessel depiction were not significantly improved on O-MAR images. The appearance of new streak artifacts that impaired interpretation was noted in 28.7% of the objects using the O-MAR. Overall interobserver agreements between the two reviewers were good-to-substantial, except for the image noise of extracranial air.
Several studies found that the O-MAR reduces metallic artifacts.1516171819 Kidoh et al.15 demonstrated that the O-MAR improved the depiction of oral cavity structures by reducing dental metallic artifacts. Jeong et al.16 found that the O-MAR significantly improved metallic artifacts due to spinal and hip prostheses. Recently, Shim et al.19 also observed an improvement in image quality using the O-MAR in patients who had undergone reverse total shoulder arthroplasty, although they reported some image degradation and new artifacts such as a pseudocemented appearance and scapular pseudonotching.
Previous studies that used other MAR algorithms to evaluate intracranial metallic implants on CTA or flat-panel detector CT images observed significant improvement in the interpretation of surrounding structures.10111213 Prell et al.10 found improved brain tissue modeling and implant visibility using an interpolation-based 3D correction algorithm for MAR; that algorithm was further modified by Psychogios et al.,11 who achieved a significant reduction of artifacts around metallic implants and improved delineation of the surrounding structures.
In our study, although we also observed a significant reduction in image noise near metallic objects, the overall image quality determined by qualitative assessment was not significantly improved by the O-MAR. This was supported by the high overall interobserver agreement by the two reviewers. However, this disagreed with previous studies that used the O-MAR in other body parts. We postulate that the discrepant results may be due to the fact that the O-MAR was optimized to reduce streak artifacts caused by orthopedic implants, which tend to be large.14 Huang et al.20 evaluated 3 commercially available MAR methods including the O-MAR and found that MAR methods generally did not successfully reduce the artifacts caused by dental fillings, where small metallic implants are located in a heterogeneous environment that includes the teeth and air cavities. Thus, relatively small intracranial metallic objects may not be accurately recognized and removed from the sinogram. In addition, target lesions containing 2 or more metallic objects on the same axial plane seemed to have significantly impacted the image quality. Thus, the inadvertent inclusion of many lesions treated with multiple clips in our study may have resulted in an apparent poor outcome when using the O-MAR compared to previous studies. A future study using a phantom to validate these findings would be valuable.
Interestingly, the image quality for the combination of a coil mass and a clip in 2 cases in our study was improved by the O-MAR (Fig. 4). It is generally known that CTA is better for the evaluation of patients who underwent aneurysm clipping,21 whereas MR angiography is better for patients who underwent embolization using platinum alloy coils for an aneurysm.22 Titanium clips generally produce less severe streak artifact than platinum coils, because titanium has a lower mass attenuation coefficient.2324 If the patient underwent both surgical clipping and coil embolization for aneurysms, selection of the most appropriate imaging modality would be problematic. Our results suggest that in such cases, it may be helpful to perform a CTA with the O-MAR. Although more time-consuming, a side-by-side comparison of non-O-MAR and O-MAR images can provide more information about the surrounding structures, as recommended by the vendor.14
The CT numbers in the various structures were not significantly different between non-O-MAR and O-MAR images except for temporalis muscle on postcontrast scan. Although there is no plausible explanation for this result, new streak artifact generated by O-MAR might have affected the CT number in the distant structures. Image noises in the temporalis muscle on postcontrast scan and extracranial air both on pre- and post-contrast scans were also significantly different between non-O-MAR and O-MAR images. The lower density of extracranial air compared to other structures might have contributed to the significant difference.
In addition to the retrospective design, several limitations of this study should be considered. First, sources of aggravating streak artifacts other than overlapping metallic objects on the same axial plane could not be systematically analyzed. The size of the coil mass, length and orientation of the surgical clips, and location of the metallic implants were not considered in the analysis. A phantom study is necessary to focus on various factors that may influence O-MAR performance. Second, we did not compare the O-MAR to other MAR algorithms, so we could not evaluate its added value compared to others. Because MAR algorithms can be applied during post-processing of raw CT data, the algorithms can be compared without an additional CT scan. Third, the reviewers interpreted both O-MAR and non-O-MAR images side by side without blinding, both because the effect of the O-MAR was evident, and because the reviewers were asked to assess the presence of new artifacts after applying the O-MAR.
In conclusion, the use of the O-MAR in patients with metallic implants significantly reduces image noise near the implant. However, the degree of the streak artifacts and surrounding vessel depiction were not significantly improved on O-MAR images.
Go to :
 XML Download
XML Download