

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In accordance with the popular use of bisphosphonates to prevent osteoporotic fractures,1234 atypical femoral fracture (AFF) appeared as a challenging problem.256
AFF is frequently associated with pain and it is diagnosed in the state of incomplete fracture.78 An incomplete AFF frequently progresses into a complete fracture.78 Once a complete fracture occurs, the surgery becomes challenging due to high rates of delayed union and non-union.5910 Therefore, there is consensus that prophylactic fixation should be done when a complete fracture is impending.51011
If the occurrence of complete fracture could be predicted, it would be helpful to decide whether to do a prophylactic fixation.
AFF is a fatigue fracture of the femur caused by repeated stresses over time.12 It might be difficult to detect early-stage AFF in plain radiographs, because it can be detected several weeks after the onset when the bone begins to remodel.13 Tc-99m hydroxymethylene diphosphonate (99mTc-HDP) bone scan, which reflects the activity of osteoblast, might detect incomplete AFF earlier than radiographs and might predict further progression to a complete fracture. However, there was no study to determine whether bone scan identifies impending complete fracture among incomplete AFFs.
Therefore, the purpose of this study was to evaluate the role of bone scan in detecting impending complete AFFs, which necessitate a prophylactic fixation.
METHODS
We retrospectively reviewed the medical records and radiographs of 57 patients (72 femurs) who were diagnosed as having an incomplete AFF at our hospital from January 2004 to December 2016. The inclusion criteria were: 1) bone scan at the time of diagnosis of an incomplete AFF; 2) no prophylactic fixation within 6 months after the bone scan; and 3) medical records and radiographs available until the time of developing a complete fracture or at least 6 months after the time of bone scan without developing a complete fracture.
A diagnosis of incomplete AFF was made according to the radiographic criteria defined by the Task Force of the American Society for Bone and Mineral Research12; 1) location from anywhere distal to the lesser trochanter and proximal to the supracondylar flare of the distal femoral metaphysis, 2) focal or diffuse thickening of the lateral cortex, and 3) an occasional discrete transverse lateral cortex translucency with periosteal callus formation.
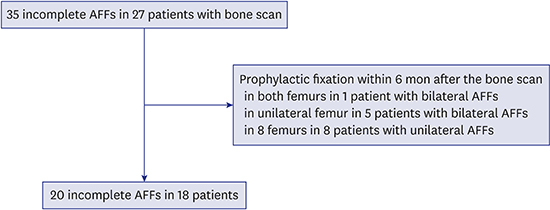
Of the 57 patients, 27 patients (35 incomplete AFFs) were studied with bone scan for the diagnostic workup. Among the 8 patients who had bilateral AFFs, 1 patient underwent bilateral prophylactic fixations, and 5 patients underwent unilateral prophylactic fixation within 6 months after the time of bone scan. Among 19 patients who had unilateral AFF, 8 patients underwent prophylactic fixation within the 6 months. The remaining 20 incomplete AFFs in 18 patients were subjects of this study (Fig. 1).
 | Fig. 1Flowchart to identify subjects who met the inclusion criteria.AFF = atypical femoral fracture.
|
All patients were women with a mean age of 73.4 years (range, 64–83 years) and a mean body mass index (BMI) of 23.8 kg/m2 (range, 17.6 to 31.6 kg/m2). In 14 patients, the mean duration of bisphosphonate treatment was 6.6 years (range, 3 to 10 years). Alendronate was used in 11 patients, and ibandronate in 3. Bisphosphonate use was stopped after diagnosis of AFF.
We defined impending fracture as a fracture that progressed to a complete fracture within 6 months after the time of bone scan.1415 The outcome for this study was defined as complete fracture or noncomplete fracture within the 6 months after the bone scan.
99mTc-HDP bone scan
Bone scanning was performed using 99mTc-HDP. Four hours prior to bone scanning, patients were injected with 30mCi 99mTc-HDP intravenously. After injection, anterior and posterior scintigrams of the pelvis, including both hips, were obtained using a gamma camera (NM/ CT670; GE Healthcare, Pittsburgh, PA, USA).
Evaluation of bone scans
Visual evaluations of radioisotope uptake in femur were performed independently by two orthopaedic surgeons, who were unaware of patient clinical information and radiological findings. Uptake in the femur on the involved lesion was classified as positive (increased uptake) and negative (normal or reduced uptake) (Fig. 2). When the two observers disagreed on the evaluation of the uptake, the final decision was made by a third observer.
 | Fig. 2An 81-year-old woman had left thigh pain for 2 months. (A) Bone scan showed hot uptake (positive finding) at the middle of femoral shaft, and (B) anteroposterior radiograph of femur revealed atypical femoral incomplete fracture. She did not have any pain or complete fracture at 11 months later.
|
Statistical analysis
To test interobserver agreement on the bone scan, the kappa value was calculated. To determine whether the bone scan could identify impending complete fracture, we calculated sensitivity, specificity, positive predictive value, and negative predictive value of bone scan. We also calculated 95% confidence interval for each value.
Statistical analysis was performed with SPSS software (version 16; Chicago, IL, USA). P values, 0.05 were considered statistically significant.
RESULTS
The kappa value was 0.780, which means a satisfactory agreement in the evaluation of uptake in bone scan. Among 20 femurs, 13 femurs had an increased uptake in bone scan, while the remaining 7 femurs had no increased uptake (Table 1).
Table 1
Qualitative evaluation of bone scan in the femur with incomplete AFF

| Bone scanning | Impending fracture | Non-fracture within 6 months | P value |
|---|---|---|---|
| Positive | 1 | 12 | 1.000 |
| Negative | 0 | 7 |
![]()
Among the 13 incomplete AFFs with the positive uptake, only 1 (7.7%, 1/13) completely fractured within 6 months (at 18 days) after the bone scan, while 4 femurs fractured from 14 to 45 months (mean, 28.8 months). Among the 7 incomplete AFFs with the negative uptake, only 1 femur completely fractured at 71 months after the bone scan.
In the remaining 14 AFFs (70%), complete fracture did not occur until a mean follow-up of 50.7 months (12 to 100 months). Thus, only one incomplete AFF was categorized as impending fracture. This incomplete AFF had increased uptake in bone scan.
In terms of bone scan as a predictor of impending complete fracture of incomplete AFFs, the sensitivity was 100% (95% CI, 2.5%–100%), specificity was 36.8% (95% CI, 16.3%–61.6%), positive predictive value was 7.7% (95% CI, 5.6%–10.5%), and negative predictive value was 100%.
DISCUSSION
Incomplete AFF usually requires prophylactic fixation when a patient has prodromal severe pain.8 To determine and predict impending fracture is very important because a reasonable prediction can not only facilitate avoidance of complete fracture, but also avoidance of unnecessary surgery. Although positive finding of bone scan can help to diagnose AFF, it does not mean the necessity of prophylactic fixation.
In our study, the sensitivity of bone scan was 100% and negative predictive value was 100% in the detection of impending complete fracture among incomplete AFFs. However, the specificity (36.8%) and positive predictive value (7.7%) were quite low. Our results showed that a positive uptake in bone scan does not mean an impending complete fracture, requiring a prophylactic fixation.
Many studies have reported that 99mTc-HDP bone scans are useful for the detection of stress fracture,16171819 and several studies used bone scans to diagnose AFF.20212223 AFFs have a characteristic appearance and can be detected on bone scan.22 Some focal thickenings of the femoral cortex, which are seen on plain radiographs, might be inactive scars after a stress reaction. These inactive lesions usually have negative findings on bone scan.13 Positive uptake in bone scan means that of radiopharmaceuticals bind to the hydroxyapatite crystals in proportion to increased local blood flow and osteoblastic activity. Therefore, positive finding of bone scan does not mean possibility of complete AFF, but it means just increased bone turnover and increased bone perfusion. Our study showed that positive uptake on bone scan did not mean an impending complete fracture, although it could be useful to diagnose AFF.
We note the limitation of our study. First, this is a retrospective study and the number of subjects was too small. However, considering incomplete AFF is a rare disease and the incidence of progression to a complete fracture is quite low, the number of our subjects was enough to calculate the sensitivity and negative predictive value. Second, we could not evaluate whether the probability of complete fracture would differ according to the degree of hot uptake (uni-cortical versus bi-cortical uptake), because of too small number of patients.
Nevertheless, our results showed that the majority of incomplete AFF with positive uptake in bone scan did not develop a complete fracture until 6 months after the bone scan. Although it is useful in the detection of incomplete AFF, bone scan showed low positive predictive value and has a limited role in identifying impending complete fracture among incomplete AFFs, while it has the perfect sensitivity (100%) and negative predictive value (100%).
 XML Download
XML Download