

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Management of chronic kidney disease (CKD) is difficult, often involving specific diets and/or fluid restrictions depending on disease status.1 Various studies have shown that the non-adherence rate of hemodialysis patients is as high as 80% depending on the definition of non-adherence.2 There are many consequences of non-adherence, including higher rates of hospital admission,3 increased financial burden, and increased mortality.4 Although many demographic factors have been associated with non-adherence in CKD, such as younger age, male gender, and low education, psychological factors have also been shown to play a role.56
A coping strategy (CS) is a method of investing one's conscious efforts to resolve personal and interpersonal problems to overcome, diminish, or endure stress and conflict.7 CSs are known to be one of the key psychological factors that affect treatment non-adherence, together with other factors such as depression, low self-efficacy, low social support, and low perceived autonomy.8 Although there are differences between studies depending on the types and definitions of CS, problem-focused CS and support-seeking CS are generally categorized into an active CS category, whereas emotion-focused CS, avoidant CS, and hopeful-thinking CS are generally categorized into a passive CS category.910 Many studies have investigated the link between CS and non-adherence in chronic diseases. Kidney transplantation patients with non-adherence to immunosuppressive medication showed a tendency to use more passive (or palliative) than active CSs compared with adherent groups.11 In patients with type 2 diabetes mellitus (DM), support-seeking CS and avoidant CS were associated with better medical adherence.12 Also, human immunodeficiency virus (HIV) patients that used an avoidant CS had greater non-adherence to medication while undergoing highly active antiretroviral therapy.13
Many CS studies have been conducted on patients undergoing hemodialysis. In hemodialysis patients, a positive reappraisal CS was most frequently employed among various strategies that included confronting, distancing, self-controlling, and support-seeking.14 A study that examined Jordanian hemodialysis patients found that various CSs were used by the patients, although it should be noted that the study did not use any kind of verified scales to determine the CS, but rather an interview based on thematic questions.15 More recently, a prospective cohort study on hemodialysis patients in Japan showed that patients using a problem-focused CS had higher survival rates and better physical and mental health than those using an emotion-focused CS.16
Comorbid conditions are also a problem in hemodialysis patients and are known to be associated with mortality.17 One study using the Korean national population-based registry database found that only 23.7% of hemodialysis patients had no comorbidities,18 and the most common comorbidities were end-organ damage (42.7%), chronic pulmonary disease (16.3%), and ulcer (14.9%).18 With so many comorbidities and CKD itself being a chronic illness, the importance of CSs to help patients living with a chronic illness is increasingly being emphasized.19
In this study, we investigated how major CSs for hemodialysis patients influenced treatment non-adherence and evaluated the association between the major CS used and the severity of comorbid conditions. We also aimed to investigate the correlation between CS and psychological status, such as level of depressive mood, stress, somatic symptoms, and life satisfaction. Based on previous study results, we hypothesized that hemodialysis patients employing passive CSs would have higher treatment non-adherence and more severe comorbid conditions compared with patients who utilized an active CS. Additionally, we hypothesized that level of depressive mood, stress, and somatic symptoms would be positively correlated with subscale scores for passive CSs. Lastly, we hypothesized that life satisfaction score would be positively correlated with the subscale scores for active CSs.
METHODS
Study participants
We recruited hemodialysis patients from the Division of Nephrology, Department of Internal Medicine, at Chung-Ang University Hospital through an advertisement in hospital bulletins from April to June 2017. Inclusion criteria were diagnosis with end-stage renal disease (ESRD) and currently receiving maintenance hemodialysis. Exclusion criteria were a major neurocognitive disorder or intellectual disability. Among a total of 81 patients who were undergoing hemodialysis at the hemodialysis unit of Chung-Ang University Hospital, 51 were initially recruited for this study. Two patients were excluded because they had a major neurocognitive disorder (Alzheimer's disease); therefore, 49 patients were finally enrolled and completed the survey.
Assessments and processing
After enrollment screening, demographic data, laboratory data, psychological data including CS and other psychological characteristics, and medication adherence data were collected from every participant.
Demographic data
Demographic variables collected were age, sex, years of education, etiology of CKD (DM/glomerulonephritis/hypertensive nephropathy/cystic disease), duration of CKD, duration of hemodialysis, and comorbid conditions including hypertension, DM, cerebrovascular disease, malignancy, and mental disorders. Using the comorbidity data, the age-adjusted Charlson comorbidity index (CCI) was calculated for each participant. The CCI has been well validated in populations with various chronic diseases, including dialysis patients and ESRD patients.1718
Psychological data: CS
A Korean version of the Ways of Coping Questionnaire (K-WCQ) was provided for assessment of participants' CSs. Based on a 67-item questionnaire developed by Folkman and Lazarus,9 the 62-item K-WCQ was revised for Koreans and validated by Lee et al.10 The K-WCQ includes 21 items regarding problem-focused CS, six items regarding support-seeking CS, 23 items regarding emotion-focused CS, and 12 items regarding hopeful-thinking CS. Individuals respond to each item on a 4-point Likert scale, indicating the frequency with which each strategy is used (from 0 = “does not apply” to 4 = “used a great deal”). Problem-focused CS refers to a strategy that tries to deal with the cause of the problems (e.g., items included in the K-WCQ are “I just concentrated on what I had to do next-the next step” or “I tried to analyze the problem in order to understand it better”). Support-seeking CS refers to a strategy that involves seeking support from family members or friends (e.g., “I talked to someone to find out more about the situation” or “I accepted sympathy and understanding from someone”). Emotion-focused CSs emphasize internal emotional management accompanied by stress awareness over specific actions toward the external world (e.g., “I turned to work or another activity to take my mind off things” or “I told myself things that helped me feel better”). Hopeful-thinking CSs are those that involve believing and making decisions based on what might be pleasing to imagine rather than verifying the evidence and using rational thinking (e.g., “I wished that the situation would go away or somehow be over with” or “I prayed”).
In this study, we used the relative scores and calculated the average score for the items in a given CS category by dividing the sum of the ratings for the category by the number of items in that category. We used the relative scores per se to assess the correlations between psychological scale scores and the subscale score for each category of the K-WCQ among the study participants. More importantly, based on the subscale that received the highest relative score on the K-WCQ, responders were divided into four CS categories according to dominant strategy: problem-focused CS, support-seeking CS, emotion-focused CS, or hopeful-thinking CS. We compared demographic, laboratory, and psychological characteristics and treatment non-adherence among these four groups.
Other psychological data
The Patient Health Questionnaire-9 (PHQ-9) is a nine-item instrument designed to screen for the presence and severity of depression in a primary-care setting.20 The Perceived Stress Scale (PSS) is a commonly used 10-item instrument that was developed to measure the degree to which a responder feels stress.21 The Symptom Check List-90-R (SCL-90-R) evaluates various symptoms of psychopathology.22 Among the questions, the somatization subscale (SCL-90R-SOM) includes 12 items rated on a five-point Likert scale that measure distress arising from perceptions of physical complaints including body systems with autonomic control and muscle pain.23 The Satisfaction with Life Scale (SWLS), the most widely used measure of life satisfaction, includes five items rated on a seven-point Likert scale.24
Medication adherence
The eight-item Morisky medication adherence scale (MMAS-8), a self-reported questionnaire, was used to measure level of treatment adherence of the participants.25 The MMAS-8 consists of seven yes-or-no questions and one item rated on a five-point Likert scale. We did not include adherence to hemodialysis in our statistical analyses because none of our participants missed any hemodialysis treatments over the entire study period.
Statistical analysis
According to the major CS as measured by the K-WCQ, we intended to divide participants into four categories: problem-focused CS, support-seeking CS, emotion-focused CS, and hopeful-thinking CS. However, because there were no participants who reported emotion-focused CS as their major CS, participants were divided into three groups: a problem-focused (PRO) group, a support-seeking (SUP) group, and a hopeful-thinking (HOP) group. Demographic, laboratory, and psychological characteristics of the three CS groups were examined by analysis of variance (ANOVA). To assess the influence of the major CS on treatment non-adherence and severity of comorbid conditions, analysis of covariance (ANCOVA) was conducted after adjusting for hemodialysis duration. Post hoc comparisons were carried out using the Bonferroni correction. The influence of the major CS on treatment non-adherence, as measured by SPL and IDWG, was calculated using the χ2 test. Correlations between psychological scale scores and the subscale score for each category the K-WCQ within the PRO group, SUP group, and HOP group were also estimated. Statistical significance for all analyses was set a priori at α = 0.05 (two-sided). We conducted all analyses using STATA/SE 12 software (StataCorp LP, College Station, TX, USA).
RESULTS
Demographic and clinical characteristics of the patients
The characteristics of the study population are summarized in Table 1. Twenty-four participants (49.0%) had a non-DM etiology of CKD, and 25 participants (51.0%) had DM as the CKD etiology. The mean duration of CKD was 104.3 ± 11.0 months, and the mean duration of hemodialysis was 73.3 ± 9.8 months. Based on the major SC reported, seven participants (14.3%) were in the PRO group, 12 (24.5%) were in the SUP group, and 30 (61.2%) were in the HOP group. No participants reported mainly using emotion-focused CSs.
Table 1
Demographic and clinical characteristics of the study population

Data are shown as mean ± standard deviation or number (%).
CKD = chronic kidney disease, DM= diabetes mellitus, HD = hemodialysis, CCI = age-adjusted Charlson comorbidity index, Problem = problem-focused, Support = support-seeking, Emotion = emotion-focused, Hope = hopeful thinking.
aNon-DM: glomerulonephritis/hypertensive nephropathy/cystic disease; bMental disorder: one patient with insomnia, one patient with alcohol dependence.
![]()
Differences in demographic and clinical characteristics among the study groups
Dialysis vintage was longer in the SUP group (117.0 ± 99.1 months) than in the PRO (42.7 ± 40. 9 months) and HOP (64.6 ± 53.5 months) groups (F [2, 46] = 3.540, P = 0.037, Table 2). There were no significant differences in age, sex, years of education, CKD etiology, or CKD duration among the three CS groups.
Table 2
Differences in demographic and clinical characteristics among the study groups allocated by major coping strategy

Demographic and clinical characteristics were analyzed using analysis of variance and χ2 test. Post hoc comparisons were carried out using the Bonferroni correction. Data are presented as mean ± standard error. Bold font indicates statistically significant group differences.
CKD = chronic kidney disease, HD = hemodialysis, DM = diabetes mellitus, PRO (P) = problem-focused coping strategy, SUP (S) = support-seeking coping strategy, HOP (H) = hopeful-thinking coping strategy.
aNon-DM: glomerulonephritis/hypertensive nephropathy/cystic disease.
![]()
Differences in psychological scale scores among the study groups allocated by major CS
There were no significant differences in the psychological scale scores among the study groups (Table 3).
Table 3
Differences in psychological characteristics among the study groups allocated by major coping strategy

Psychological characteristics were analyzed using the analysis of variance test. Post hoc comparisons were carried out using the Bonferroni correction. Data are presented as mean ± standard error.
PHQ-9 = Patient Health Questionnaire-9, PSS = Perceived Stress Scale, SCL-90R-SOM = Symptom CheckList-90-Revised-Somatization, SWLS = Satisfaction With Life Scale, PRO (P) = problem-focused coping strategy, SUP (S) = support-seeking coping strategy, HOP (H) = hopeful-thinking coping strategy.
![]()
Influence of major CS on treatment non-adherence and severity of comorbid conditions
The mean MMAS-8 score was higher in the PRO group (7.2 ± 0.5) than in the HOP group (5.2 ± 2.0; F [2, 46] = 4.045, P = 0.024, Table 4). The mean age-adjusted CCI score was lower in the PRO group (5.0 ± 1.8) than in the HOP group (7.2 ± 2.1; F [2, 46] = 4.440, P = 0.017). There was no significant difference in the number of participants with non-adherence according to SPL > 5.5 mmol/L and IDWG ≥ 2.5 kg among the PRO group, SUP group, and HOP group.
Table 4
Influence of major coping strategy on treatment adherence and severity of comorbid conditions

Analysis of covariance was conducted after adjusting for duration of hemodialysis as a covariate. Post hoc comparisons were carried out using the Bonferroni correction. Data are presented as mean ± standard error or number (%). Bold font indicates statistically significant group differences.
PRO (P) = problem-focused coping strategy, SUP (S) = support-seeking coping strategy, HOP (H) = hopeful-thinking coping strategy, MMAS-8 = 8-item Morisky medication adherence scale, CCI = age-adjusted Charlson comorbidity index, SPL = serum phosphate level, IDWG = interdialytic weight gain, η2P = partial Eta squared.
aInfluence of major coping strategies on treatment non-adherence was measured according to biochemical parameters. Pre-dialysis SPL > 5.5 mmol/L and IDWG ≥ 2.5 kg were calculated using the χ2 test.
![]()
Correlation analyses between psychological scale scores and the subscale score for each K-WCQ category
In the HOP group, the SCL-90R-SOM score was positively correlated with the subscale score for the emotion-focused CS category (r = 0.39, P = 0.029) and the subscale score for the hopeful-thinking CS category (r = 0.38, P = 0.036; Fig. 1). Additionally, the SWLS score was positively correlated with the subscale score for the problem-focused CS category (r = 0.398, P = 0.027) in the HOP group. The other groups showed no correlations between psychological scale scores and the subscale scores for each K-WCQ category.
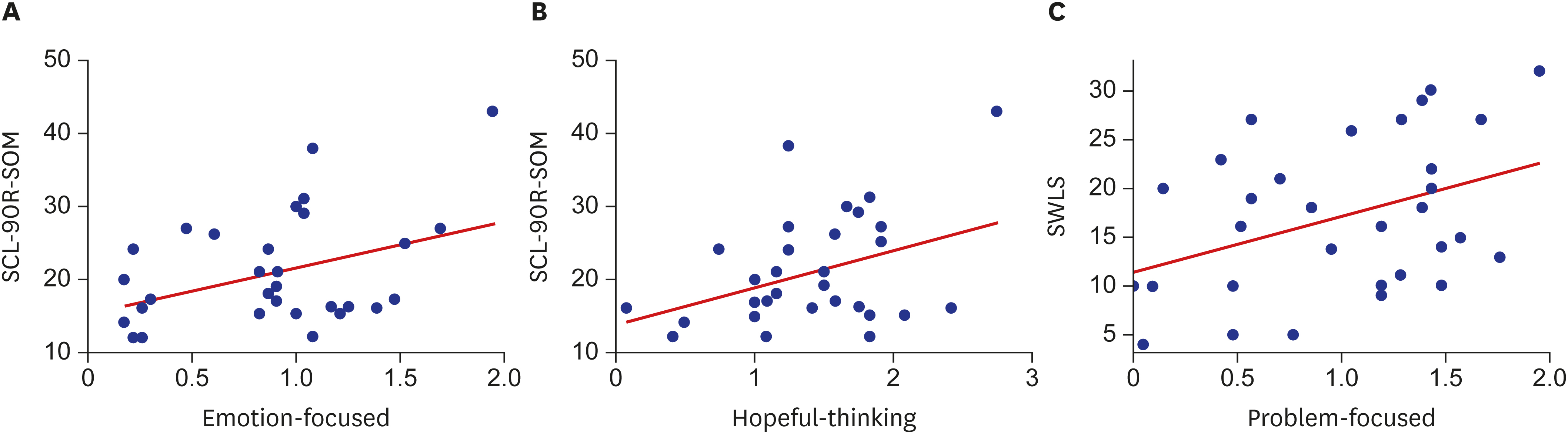 | Fig. 1Correlation analyses between psychological scale scores and the subscale score for each category of K-WCQ in the HOP group. Correlation analyses between psychological scale scores in the HOP group were conducted. The X-axis represents the relative score of each CS category of K-WCQ. (A) SCL-90R-SOM vs. Emotion-focused CS subscale: r = 0.39, P = 0.029. (B) SCL-90R-SOM vs. Hopeful-thinking CS subscale: r = 0.38, P = 0.036. (C) SWLS vs. Problem-focused CS subscale: r = 0.40, P = 0.027.K-WCQ = Korean version of the ways of coping questionnaire, HOP = hopeful-thinking coping strategy, SCL-90R-SOM = Symptom CheckList-90-Revised-Somatization, SWLS = Satisfaction With Life Scale, CS = coping strategy.
|
DISCUSSION
In this study, non-adherence to medication was more common in the HOP group than in the PRO group, and comorbid conditions were less severe in the PRO group than in the HOP group. There was no significant difference in the number of participants with treatment non-adherence when measured as a biochemical parameter. In the HOP group, the severity of somatic symptoms was positively correlated with the use of emotion-focused CSs and hopeful-thinking CSs. Furthermore, the level of life satisfaction was positively correlated with the use of problem-focused CSs in the HOP group. To our knowledge, this is the first study to investigate the influence of major CS on both treatment non-adherence and severity of comorbid conditions in hemodialysis patients.
We found that non-adherence to medication was greater in the hemodialysis patients who used hopeful thinking as their major CS compared with those who used problem-focused CSs. This is consistent with previous studies that found that patients using an active CS were more likely to have higher adherence than patients using passive, emotional, or evasive CSs.111326 Both passive and active CSs were important for dealing with stress, in that they play complementary roles in controlling stress.27 However, CSs based on problem solving can help patients adapt better to their long-term illness because the patient deals directly with the stressor, which in this case involves following their medical regimen rather than avoiding it.1128 Our study results are consistent with a previous study in which having superior knowledge about one's illness and a sense of personal control were associated with increased treatment adherence.26 Thus, physicians should pay more attention to the major CS used by patients and provide interventions to promote problem-focused CSs that focus on illness knowledge and an enhanced sense of personal control, especially for nonadherent patients who mainly employ a hopeful-thinking CS.
In this study with hemodialysis populations, one or more comorbid condition was present in 87.8% of the study population. Comorbidities are highly prevalent in dialysis patients and are related to increased mortality and high socioeconomic costs.1718 Both age and CCI score strongly predicted mortality in dialysis patients, and age-adjusted CCI was a stronger predictor of mortality than age or CCI alone.1718 The most commonly reported comorbidities among Korean hemodialysis patients were diabetes with end-organ damage (42.7%), chronic pulmonary disease (16.3%), and ulcer (14.9%).1829 All comorbidities except ulcer were significant predictors of mortality in Korean hemodialysis patients, with metastatic solid tumor being the strongest predictor of mortality and chronic pulmonary disease the weakest predictor.18 We found that the severity of comorbid conditions was greater in hemodialysis patients who used hopeful-thinking CSs as their major strategy compared with those who used problem-focused CSs. The reason for this might be the same as the explanation for treatment non-adherence; that is, patients who use problem-focused CSs are better able to actively deal with their comorbid diseases by following their treatment regimen rather than disregarding it.1128 Thus, providing interventions to promote problem-focused CSs, especially for patients with more comorbidities who rely more heavily on hopeful-thinking CSs, could be helpful for the management of comorbid conditions and might even reduce mortality risk and reduce socioeconomic burdens.
We found that using a hopeful-thinking CS as a major strategy was associated with non-adherence to medication and more severe comorbid conditions. However, it is important to distinguish between using hopeful thinking as the major CS and having high levels of hope. Patients with serious and/or chronic illness often think that they should have a subjective plan to deal with dire statistics and maintain a hopeful state that has little to do with medical evidence. The influence of hope on psychological adjustment to chronic medical illness has been extensively studied.303132 In a study on patients with multiple sclerosis, higher levels of hope were associated with higher levels of psychological adjustment to illness as measured by depressive mood, positive affect, and life gratification.32 According to a previous review on the role of hope in adolescents with chronic disease, hope seems to improve health, adaptation, quality of life, drive, self-respect, resilience, and maturity of affect.31 Although previous research has suggested that high levels of hope can help patients manage their psychological symptoms, there is still a lack of studies regarding its influence on physical health outcomes. This might be mainly because the scientific literature does not use a clearly unified concept of hope.33 For future studies, a definition of hope should be systematically established to improve comparability and knowledge. We emphasize that therapists should help patients anticipate their future disease-related circumstances so that they can maintain hope and continue to receive treatment, in addition to promoting problem-focused CSs and awareness of one's illness.
In the HOP group, the severity of somatic symptoms was positively correlated with the use of emotion-focused CSs and hopeful-thinking CSs. Additionally, the level of life satisfaction was positively correlated with use of a problem-focused CS in the HOP group. In a previous systematic review of mental problems in patients with testicular cancer, poorer psychological outcomes were associated with passive CSs in addition to other factors of being single, jobless/low socioeconomic status, having comorbid disease, or worse symptoms/adverse effects from medications.34 We found no correlations between psychological scale scores and subscale scores for any CS category. These results might be due to the small study population in the PRO and SUP groups.
This study has several limitations. First, the sample size was too small when divided into three groups; therefore, further studies with a larger number of participants are necessary to ensure the generalizability of our results. In particular, the small sizes of the PRO group (n = 7) and SUP group (n = 11) made it difficult to observe linear correlations between psychological scale scores and subscale scores from each CS category of K-WCQ. Second, we found no significant differences across study groups in the number of participants with treatment non-adherence as measured by the biochemical parameters SPL > 5.5 mmol/L and IDWG ≥ 2.5 kg. This is probably because various factors influence SPL and IDWG, including hemodialysis adequacy, residual renal function, dietary phosphate intake, medications such as oral phosphate binders and vitamin D, and hyperparathyroidism.135 Third, due to the cross-sectional nature of this study, it is not possible to determine a causal relationship between major CS and treatment non-adherence or severity of comorbid conditions in hemodialysis patients; therefore, future studies with a longitudinal design are needed to understand the directionality of these associations.
Based on our results, we conclude that physicians should pay more attention to the major CS used by hemodialysis patients and provide interventions to promote problem-focused CSs that focus on knowledge about one's illness and enhance a sense of personal control, especially for nonadherent patients with high comorbidities who mainly use hopeful-thinking CSs. Additional studies are needed to explore whether these findings are corroborated by larger samples and to determine whether working with patients to improve problem-focused coping skills results in better treatment adherence and less severe comorbidities.
 XML Download
XML Download