

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Inflammatory bowel disease (IBD) is a heterogeneous, chronic relapsing disorder of unknown etiology that consists of Crohn's disease (CD) and ulcerative colitis (UC). IBD is more common in Western countries and relatively rare in Asia; however, it is rapidly increasing worldwide and increasing steadily in Asia and Korea.123
Since approximately one-quarter of all IBD patients are diagnosed during childhood and the number of patients is rapidly increasing, the clinical significance of IBD has gradually increased in the pediatric area. However, there is a lack of research into the prevalence of pediatric IBD, regional epidemiologic characteristics and clinical features in Korea.
This study aimed to investigate the characteristics of pediatric patients diagnosed with IBD at a university hospital in Daegu-Kyungpook province in Korea. Multicenter studies that represent pediatric IBD in a specific region are of great significance since they are the first in Korea. Therefore, here we investigated the epidemiologic and phenotypic features of pediatric IBD in Daegu-Kyungpook province in Korea.
Go to : 
METHODS
Patients
We included 122 Korean children < 18 years of age who were initially diagnosed with IBD at the Department of Pediatrics in one of four university hospitals (Daegu Catholic University School of Medicine, Keimyung University School of Medicine, School of Medicine, Kyungpook National University, Yeungnam University School of Medicine) in Daegu-Kyungpook province in Korea between July 2010 and June 2016.
Methods
The diagnosis was based on conventional clinical, endoscopic, radiologic, and histopathologic criteria. The data were retrospectively collected from the patients' medical records. Patients were excluded from the study if they were transferred from another hospital during treatment.
Annual number of children newly diagnosed with IBD and annual pediatric population (< 18 years of age) in Daegu-Kyungpook province were investigated to obtain the incidence.
Baseline patient demographic and clinical information, including sex, date of birth, date of diagnosis, disease location, disease behavior, severity, and growth change at diagnosis were retrospectively investigated. The patients' clinical characteristics at diagnosis were compared by Paris classification.4
Statistical analysis
An incident case was defined as children newly diagnosed with IBD in the corresponding year, and incidence was defined as the number of incident cases in the corresponding year per 106 using the resident population on the last day of every year.
Testing for uniform distribution (the probability of each event was exactly the same) according to each clinical characteristic or outcomes was performed using the chi-square goodness of fit test. All analyses were performed using IBM SPSS Statistics 19.0 (IBM Corp., Armonk, NY, USA), and P values < 0.05 were considered significant.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board (IRB) of Daegu Catholic University Medical Center (CR-17-095). And this study protocol was approved by each center's IRB, too. They were following as Kyungpook National University Hospital (KNUCH 2017-09-015), Yeungnam University Hospital (YUMC 2017-08-004), Dongguk University Hospital (110757-201708-04-01), and Keimyung University Hospital (2017-09-011-001).
Go to :
RESULTS
Baseline characteristics
We included a total of 122 children, 98 with CD (80.3%) and 24 with UC (19.7%). The mean age of diagnosis (mean ± standard deviation) was 13.5 ± 3.0 years for IBD, 13.7 ± 2.9 for CD and 12.9 ± 2.7 for UC. There was no significant difference between patients with CD and UC at the time of diagnosis.
Incidence
During the 6-year study period, there has been a steeply increasing trend in the number of children newly diagnosed with IBD. In 2010, when the survey was first initiated, 9 children were new diagnosed with IBD; by 2016, the number increased to 30. This temporal trend of an increasing number of patients was observed more prominently in CD than in UC. On the other hand, the population of Daegu-Kyungpook province is decreasing. The mean ratio of newly diagnosed CD:UC ratio is 4:1 (Table 1).

Table 1
Annual number of newly enrolled pediatric IBD patients and annual population in Daegu-Kyungpook province
![]()
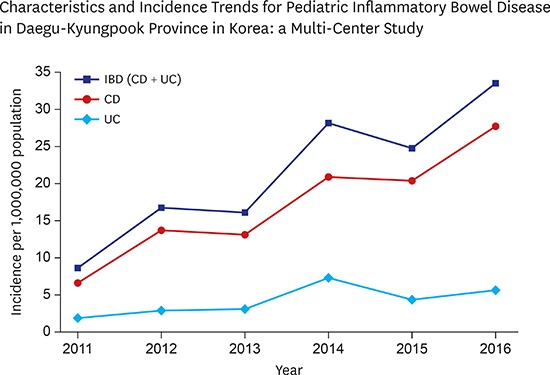
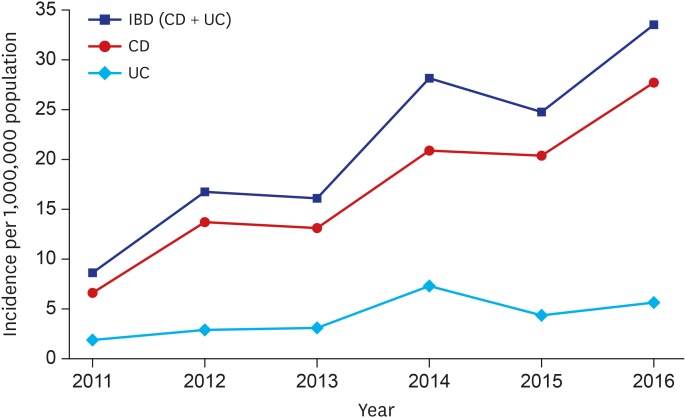
Incidence of pediatric IBD patients is shown in Fig. 1. The incidence also shows an increasing trend. The incidence for IBD from 2011 to 2016 was 8.6 to 33.3 per 106 and for CD was 6.7 to 27.8 per 106 and for UC was 1.9 to 5.6 per 106.
Clinical characteristics of CD patients
With respect to CD, there was a significant male predominance (74 boys, 24 girls; P < 0.001). The age distribution at diagnosis showed A1a in 5 (5.1%), A1b in 88 (89.8%), and A2 in 5 (5.1%) patients. Most of the patients (94.9%) were diagnosed after 10 years of age. The disease activity sites by Paris classification were L1 in 10 (10.2%), L2 in 12 (12.2%), L3 in 76 (77.6%), and L4 in 16 (16.3%). Notably, the most common location was L3, indicating ileocolonic involvement as the major type. The disease behaviors by Paris classification were that 87 patients (88.8%) had non-stricturing/non-penetrating lesions (B1) and 11 patients (11.2%) had strictures or penetrating lesions, including B2 (stricturing) in 7 (7.2%), B3 (penetrating) in 2 (2.0%), and B2B3 (both penetrating and stricturing) in 2 (2.0%). Perianal disease was noted in 43 patients (43.9%) and weight loss in 60 (61.2%). The mean Pediatric Crohn's Disease Activity Index score at the time of diagnosis was 41.4. The data of patients with CD are summarized in Table 2.
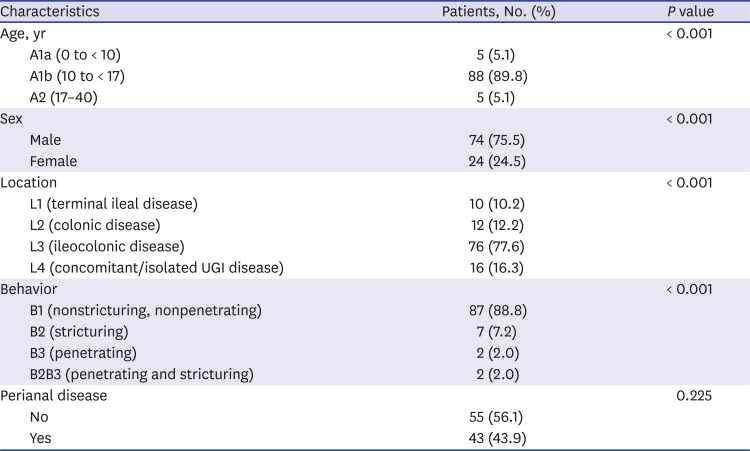
Table 2
Clinical characteristics of CD by Paris classification
![]()
Clinical characteristics of UC patients
In UC, the male to female ratio was 1:1.2 without statistical significance (11 boys, 13 girls; P < 0.683). Most patients with UC (22 patients, 91.7%) were diagnosed after 10 years of age, while only 2 (8.3%) were diagnosed prior to 10 years of age. The disease activity sites by Paris classification were E1 (proctitis) in 5 (20.8%), E2 (left-sided) in 3 (12.5%), E3 (extensive) in 2 (8.3%), and E4 (pancolitis) in 14 (58.4%), indicating pancolonic involvement as the major type. The mean Pediatric Ulcerative Colitis Index score at the time of diagnosis was 41.8. Disease severity by Paris classification was S0 (never severe) in 17 patients (70.8%) and S1 (ever severe) in 7 (29.2%). The data of patients with UC are summarized in Table 3.
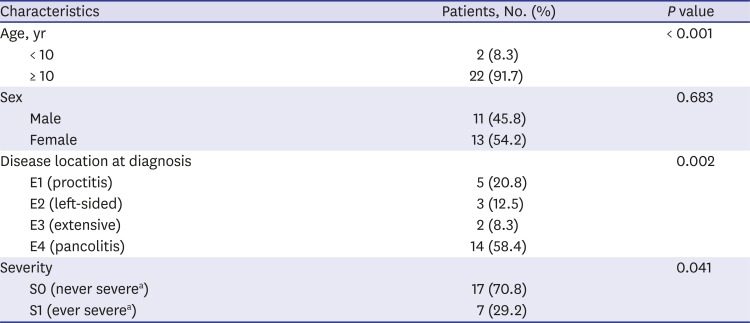
Table 3
Clinical characteristics of UC by Paris classification
UC = ulcerative colitis.
aSevere defined as a Pediatric Ulcerative Colitis Activity Index score ≥ 65.
![]()
Go to :
DISCUSSION
The prevalence and annual incidence of IBD in the Korean pediatric population have not been elucidated. Recent single-center studies proved that the number of newly diagnosed pediatric patients with CD has increased since 2000.25 In Western countries, many studies have shown the increasing incidence of pediatric IBD.67 It is the first study in Korea to validate the incidence and phenotypic characteristics of pediatric IBD in a specific area.
A total of 122 children were included (85 males, 37 females) in our study, and the number of newly diagnosed IBD patients has been rapidly increasing each year over the last 6 years. Using the population statistics data, we validated the annual incidence of IBD in Daegu-Kyungpook province has been increasing during the enrollment period (2011–2016) (Fig. 1).
The age of most CD patients at diagnosis (89.8%) was 10–17 years, while 20 of 22 (91.7%) UC patients were older than 10 years. These results are similar to those of a study in the USA in which the highest incidence of IBD was observed among 10–14-year-old for both CD and UC.8 Our study revealed that approximately 5% of IBD patients were < 10 years of age. However, a recent study in Canada emphasized the increased incidence in children younger than 10 years of age as well as those 10–19 years of age.9 Considering the worldwide increasing incidence of IBD in children and adolescents, a healthcare policy for the early detection of IBD seems necessary.10
The male to female distribution of CD patients was 3.1:1 (74 boys, 24 girls) in this study, similar to the results of other pediatric IBD studies in Korea.211 In our study, there was a significant male predominance in CD (P < 0.001), and this tendency became more evident than that in a previous single-center study in which the male to female ratio was 2.2:1.2 In Korea, a marked male predominance in adult CD patients was proven by a population-based study. Data of Asian adults seem to support a male preponderance for CD but an equal or slight male preponderance for UC.112 In Western studies, however, few conflicting results of the sex distribution in pediatric patients with CD have been reported. The EUROKIDS study reported no sex-difference in incidence, but another study conducted in North America reported a female predominance.1314 Another Western study reported a male predominance, especially in pediatric CD.1516 The conflicting results of pediatric CD in western countries may be due to both environmental effects and the diverse ethnic profiles in Europe and America. However, the reasons for male predominance in Korean CD patients are not known; thus, we focused on the sex composition of our study area during the enrollment period (2010–2016). According to Korea National Statistical Office data, the number of males exceeds that of females in Daegu-Kyungpook province throughout all age groups (range, 0–18 years). The difference becomes more prominent as age increases, especially in adolescents. To validate the cause of male predominance in pediatric CD, several factors such as sex and fast food consumption require consideration.
Conversely, the sex distribution of UC patients was quite different from that of CD patients. Our data revealed no sex-based difference in UC patients. In adults, one population-based study already revealed that the male to female ratio was equal in UC patients in Korea.1 A similar study conducted in North America also reported no sex differences in pediatric patients with UC.17 However, two previously published Korean pediatric studies of IBD reported a male predominance and a female predominance, respectively.211 The reason for the conflicting results of sex distribution in pediatric UC may be due to the relatively small cohort size.
In our study, the proportion of ileocolic disease (L3 phenotype) among CD types exceeded 70%. Colonic disease (L2) and terminal ileal disease (L1) comprised 12.2% and 10.2%, respectively. A mild L2 predominance was observed, but the difference was negligible compared with the result of the EUROKIDS study, in which L2 (27%) was predominant to L1 (16%).13 Other Korean studies reported an L1 predominance over L2, while a previously published single-center study reported an equal L1 (ileal) to L2 (colonic) ratio.21118 Thus, a large-scale population-based study seems necessary to validate the clinical features of pediatric IBD patients in Korea.
The rate of perianal disease was 43.9%, higher than that noted in Western children (9%–15%).131920 In Korea, other single-center studies have already reported that about 50% of CD patients had a perianal fistula or abscess at the time of the diagnosis.221
Our data show that a high proportion of children with UC had pancolitis, which corresponds with the results of the EUROKIDS study and other Korean studies.22 However, the ratio of the E1 phenotype was 18.2%–21% in Korean children, similar to our findings (20.8%); this is higher than that in Western countries, where the ratio was < 5%.2111922
Our study has some limitations. First, our data were obtained from 4 referral centers in the study area but may be insufficient since some patients were referred to other centers outside the study area. Second, we used the Paris classification, which can be more sophisticated for examining pediatric patients; however, we could not collect complete information in some cases because of the retrospective nature of the study.
Although this was not a population-based study, it is the first study in Korea to validate the incidence and phenotypic characteristics of pediatric IBD in a specific area. In the previous single-center study, more than half of the IBD patients were from other districts; thus, the results could not precisely reflect the characteristics of the study area.2 Additionally, since the CD patients were assessed with the Montreal classification, the possibility of a detailed evaluation was limited.
In conclusion, we found that the number of pediatric patients with IBD is increasing rapidly in Daegu-Kyungpook province in Korea. Our study also revealed that the characteristics of pediatric IBD in our province differ somewhat from those of pediatric IBD in Western countries.
Go to :
 XML Download
XML Download