

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
Cardiovascular disease (CVD) is the main cause of morbidity and mortality in type 2 diabetes. Compared with non-diabetic patients, diabetic patients have a 3-fold higher risk of CVD and a poorer clinical outcome.1 Atherosclerotic CVD in type 2 diabetes has multiple mechanisms involving interactions between immune, dyslipidemia, hemodynamic, genetic, and environmental factors.
Cytokines from the adipose tissue are involved in lipid and glucose metabolism, blood pressure (BP), coagulation, feeding behavior, angiogenesis, and vascular endothelial growth.2 It plays a pivotal role in the development of CVD.
Adiponectin, an adipocyte-specific protein, has been thought to be a key adipokine in the regulation of insulin action and the metabolism of glucose and lipid.345 It has potential anti-atherosclerogenic and anti-inflammatory properties through a direct effect on the endothelium, while also inhibiting vascular smooth muscle cell proliferation and the production of tissue necrosis factor-α (TNF-α).678 Furthermore, the plasma adiponectin levels are inversely associated with the risk of CVD.9
It is thought that there is a possible significant relationship in adiponectin with both type 2 diabetes and CVD. Serum adiponectin levels may be influenced by physical activity and food intake as well as genetic variations. The adiponectin gene contains 3 exons and 16 single nucleotide polymorphisms (SNPs) localized on chromosome 3q27.10 Some reports suggest the possible relationship between adiponectin polymorphisms and CVD in type 2 diabetes.1112 Among the SNPs of adiponectin, 45T/G has been reportedly associated with an increased risk of insulin resistance or type 2 diabetes.13 However, it is uncertain whether the adiponectin 45T/G polymorphism is a relevant marker of diabetic cardiovascular complications in type 2 diabetes.
This study evaluated the associations between adiponectin 45T/G polymorphism and cardiovascular complications in type 2 diabetes in Koreans.
METHODS
Subjects
The study was designed as a case-control study, wherein 758 patients with type 2 diabetes enrolled in Chungbuk National University. The inclusion criteria included the following:
1) age ≥ 30 years at the time of diagnosis of diabetes; 2) known diabetes duration of ≥ 5 years; and 3) no historical evidence of ketoacidosis. Diabetes was diagnosed based on the World Health Organization (WHO) criteria. All patients underwent biochemical testing and their history was documented. Cardiovascular complications (history of chronic angina, unstable angina, myocardiac infarction, and intervention of coronary artery disease) were assessed according to the available medical records. We evaluated the clinical characteristics and cardiovascular complications according to the adiponectin 45T/G genotype. We also compared cerebrovascular complications, peripheral artery disease, and diabetic nephropathy according to adiponectin 45T/G genotype as well.
Determination of adiponectin 45T/G genotype
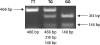
Peripheral leukocytes were isolated from ethylenediaminetetraacetic acid (EDTA)-treated whole blood obtained from each patient, and genomic DNA was extracted for polymerase chain reaction (PCR) amplification of adiponectin. The following primers were used for amplification: forward 5′-AGACTCTGCTGGATGGACGGAGTCC-3′ and reverse 5′-CCCCAAATCACTTCAGGTTGCTTATGG-3′. The PCR premix consisted of PCR buffer (10 mM), dNTP (0.2 mM), MgCl2 (1.5 mM), each primer (0.8 pM/ll), and 1 U Taq polymerase. Cycling was done in a thermal cycler with the following program: 96°C for 3 minutes, followed by 35 cycles of 94°C for 30 seconds, 67.5°C for 1 minute, 10 seconds, and a final extension at 72°C for 5 minutes. Then the PCR product was digested using SmaI for 16 hours at 37°C with 2 μL Tango buffer and 2 μL SmaI (Fermentas, Leon-Rot, Germany). There were three genotypes: TT, which has a single band at 466 bp; TG, which has three separate bands at 318 bp, 148 bp, and 466 bp; and GG, which has two bands at 318 bp and 148 bp (Fig. 1).
Statistical analysis
Statistical analyses were performed using SPSS 20.0 (SPSS Inc., Chicago, IL, USA). The biological parameter values were reported as means and standard deviation (SD), and were compared by the Student's t-test. Categorical variables were analyzed by the χ2 test. Multiple logistic regression analyses were performed to evaluate the relationship between the prevalence of CVD and the following variables: gender, age, smoking status, body mass index (BMI), HbHbA1c, duration of diabetes. P values of < 0.05 were considered statistically significant.
RESULTS
Comparison of clinical characteristics according to the adiponectin 45T/G polymorphism
The present study included 758 patients with type 2 diabetes, comprising 401 males and 357 females. The distribution of the adiponectin 45T/G polymorphism was 3.56% (n = 27) for GG, 42.35% (n = 321) for TG, and 54.09% (n = 410) for TT in patients with type 2 diabetes. Furthermore, the genotypes deviated from Hardy-Weinberg equilibrium. The mean age of the patients was 57.43 ± 10.75 years, mean duration of type 2 diabetes mellitus was 13.31 ± 3.52 years, and mean BMI was 24.95 ± 3.52 kg/m2. The mean fasting blood sugar (FBS) level was 8.00 ± 3.05 mmol/L, mean post prandial 2 hours (PP2) was 11.47 ± 4.39 mmol/L, and mean HbHbA1c was 7.56% ± 1.37%. The clinical and biochemical characteristics of the patients are presented in Table 1.
Table 1
Clinical and biochemical characteristics of patients with type 2 diabetes according to the adiponectin 45T/G polymorphism

BMI = body mass index, DM = diabetes mellitus, FBS = fasting blood sugar, PP2 = post prandial 2 hours, HbA1c = glycated hemoglobin, TC = total cholesterol, HDL-C = high-density lipoprotein cholesterol, LDL-C = low-density lipoprotein cholesterol, BUN = blood urea nitrogen.
![]()
We divided the patients into 2 groups: GG + TG allele group and TT allele group. There were no significant differences between the 45T/G polymorphism in age, BMI, duration of diabetes, FBS, PP2, HbHbA1c, C-peptide, insulin, triglyceride, and low-density lipoprotein cholesterol (LDL-C). There was a significant difference found between two groups in the sex ratio. The gender ratio of the GG + TG group was 58.3% male vs. 41.7% female, and the TT group was 48.3% male vs. 57.3% female. The portion of males was higher in the GG + TG group than in the TT group. There was a significant difference in the lipid level between the two groups. The GG + TG group had a lower level of total cholesterol and high-density lipoprotein cholesterol (HDL-C) than the TT group.
Cardiovascular complications and adiponectin 45T/G polymorphism
The prevalence of CVD was significantly higher in subjects with the GG + TG genotype compared to those with the TT genotype (17.5% vs. 9.8%, P = 0.002) (Table 2). The G allele was associated with a higher risk of CVD (P = 0.002). The results of the single factor logistic regression analysis showed that the adiponectin 45T/G genotype (GG + TG genotype vs. TT genotype, odds ratio [OR], 1.966; 95% confidence interval [CI], 1.282–3.015; P = 0.002) and the G allele were risk factors for CVD in type 2 diabetes (G allele vs. T allele, OR, 1.472; 95% CI, 1.132–1.897; P = 0.003). After adjusting for confounding factors, including duration of diabetes, smoking, hypertension, BMI, lipid level, and HbA1c, the adiponectin 45T/G genotype and G allele continued to be risk factors for CVD in type 2 diabetes (Table 3).
Table 2
Distribution of the adiponectin 45T/G polymorphism in Korean type 2 diabetic patients with cardiovascular complications

| Genotypes | No. of patients without cardiovascular complications | No. of patients with cardiovascular complications | P value |
|---|---|---|---|
| TT | 370 (90.2) | 40 (9.8) | 0.002 |
| GG + TG | 287 (82.5) | 61 (17.5) |
![]()
Table 3
Multiple logistic regression analysis for the presence of cardiovascular disease and different variables in type 2 diabetes
OR = odds ratio, CI = confidence interval, DM = diabetes mellitus, FHX = family history, BMI = body mass index, HbA1c = glycated hemoglobin, TC = total cholesterol, LDL-C = low-density lipoprotein cholesterol, HDL-C = high-density lipoprotein cholesterol.
![]()
Diabetic macrovascular complications and adiponectin 45T/G polymorphism
We evaluated the association of the adiponectin 45T/G polymorphism and diabetic macrovascular complications, such as stroke or peripheral artery disease. There was no association between the adiponectin 45T/G polymorphism with stroke or peripheral artery disease (Table 4).
Table 4
Distribution of the adiponectin 45T/G polymorphism in Korean type 2 diabetic patients with macrovascular complications
![]()
Diabetic microvascular complications and adiponectin 45T/G polymorphism
We evaluated the association of the adiponectin 45T/G polymorphism with diabetic microvascular complications such as diabetic end-stage renal disease or peripheral neuropathy. However, there was no association between the adiponectin 45T/G polymorphism with diabetic end-stage renal disease or peripheral neuropathy (Table 5).
Table 5
Distribution of the adiponectin 45T/G polymorphism in Korean type 2 diabetic patients with microvascular complications

| Genotypes | Peripheral neuropathy | ESRD | P value | ||
|---|---|---|---|---|---|
| Without | With | Without | With | ||
| TT | 211 (51.5) | 199 (48.5) | 404 (98.5) | 6 (1.5) | 0.729 |
| GG + TG | 176 (50.6) | 172 (49.4) | 341 (98.0) | 7 (2.0) | 0.562 |
![]()
DISCUSSION
We investigated the association of the adiponectin 45T/G polymorphism with diabetic complications in type 2 diabetes. Among the 758 Korean patients that we recruited for this study, the TT genotype occurred in 410 cases (54.09%), TG genotype in 321 cases (42.35%), and GG genotype in 27 cases (3.56%). Several studies showed that the GG genotype appeared with various results (0.6% to 15.5%).14151617 The frequency of the GG genotype was lower than the TT and TG genotype.
Adiponectin is an adipose tissue-derived adipokine that is abundantly present in the human plasma with a concentration ranging from 3 to 30 μg/mL.1819 Adiponectin might play a pivotal role in the modulation of glucose and lipid metabolism in insulin-sensitive tissues in both humans and animals. The main mechanism of adiponectin in lipid and glucose metabolisms is the activation of adenosine monophosphate (AMP)-activated protein kinase and stimulation of peroxisome proliferator-activated receptor (PPAR)-α, which leads to increased glucose uptake and oxidation of fatty acids in skeletal muscle as well as decreased hepatic glucose output.20
There is increasing evidence from experimental and clinical studies suggesting that adiponectin exerts favorable effects in CVD. There are several mechanisms through which adiponectin may have a protective effect on CVD, including stimulation of angiogenesis, endothelial cell migration and differentiation, prevention of endothelial apoptosis, and reduction of the expression of TNF-α and vascular cell adhesion molecule.321
Several studies have suggested the association of low levels of adiponectin with CVD.9 Low level of adiponectinemia is defined as the 25th percentile, which was associated with a 2-fold increase in CVD prevalence in male subjects.22 Among the patients with type 2 diabetes, those with CVD have lower adiponectin levels than those without CVD. However, adiponectin levels are increased in patients with type 1 diabetes plus chronic renal failure. Hypoadiponectinemia is an independent predictor of CVD in these patients.23 A previous studied was unable to confirm the strong association previously reported between adiponectin levels and CVD. A meta-analysis of seven studies had shown only a moderate association.24 Another study in men with CVD showed reverse effects, wherein higher adiponectin levels were an independent predictor of both overall mortality and cardiac mortality.25 Currently, it remains controversial whether hypoadiponectinemia is a risk factor for CVD. Future studies are needed to further evaluate the link between adiponectin levels and CVD.
Recent studies have reported the possible correlation of adiponectin polymorphisms as risk factors for CVD in diabetic patients. A previous study evaluated the role of five SNPs within the adiponectin gene in the susceptibility to CVD among patients with type 2 diabetes.26 In a univariate and multivariate analysis, the adiponectin 45T/G polymorphism was associated with CVD. Independent classical cardiovascular risk factors including risk factors of metabolic syndrome (BMI, BP, HDL-C, and triglycerides). The GG and TG genotypes presented an increased risk of CVD as compared to the TT genotype. Similarly, the GG + TG patient group was significantly associated with a higher risk of CVD in our study.
The positive effect of the adiponectin 45T/G polymorphism has not been confirmed by subsequent studies. A previous study evaluated the possible role of two frequent SNPs (+45T>G and +276G>T) as genetic markers of CVD in a cohort of Italian patients with type 2 diabetes.12 Contrary to previous studies, they did not find any significant differences in genotype distribution at position +45 between the CVD and control subjects in a total of 376 Italian subjects with type 2 diabetes. These results were consistent with the results of another study,27 where the authors investigated the association of the adiponectin 45T/G polymorphism with adiponectin levels and cardiovascular risk in a cohort of diabetic patients. No significant association between the adiponectin 45T/G polymorphism and CVD in diabetic women was found. In this study, the genotype and allele frequencies deviated from Hardy-Weinberg equilibrium, and the proportion of males was higher in the GG + TG group than the TT group. The different characteristics of the subjects might result in opposite results.
In a non-diabetic population of 595 Caucasian individuals from Italy, no significant differences in the genotype of the adiponectin 45T/G polymorphism between patients with CVD and controls were found.28 Likewise, another study also reported a lack of association between the SNP and the presence of CVD in Korean subjects.29
This finding was in accordance with a previous report that showed no significant genotype effect of the adiponectin 45T/G polymorphism on cardiovascular risk factors including BP, anthropometric parameters, lipid profile, serum glucose, homeostasis model assessment of insulin resistance, adiponectin, plasma C-reactive protein, and urinary prostaglandin F2α concentration among 902 non-diabetic Korean subjects.30 In contrast, there were several studies that showed a significant association between the adiponectin 45T/G polymorphism and CVD in non-diabetic patients. One study reported that mutated genotypes at the adiponectin 45T/G polymorphism were significantly related with increased coronary artery disease among obese patients.31 Another meta-analysis study on 28 case-control studies, which evaluated a total of 12,378 cases of CVD with 19,368 controls, demonstrated a significant association between the adiponectin 45T/G polymorphism in the adiponectin gene and the risk of CVD.32 This meta-analysis concluded that the G allele has a significant association with risk of CVD among Caucasians but not Asians.
There were several causes such as ethnicity in genetic background, sample size, different study population, and a wide span of CVD that might have possible contributions to the various effects of the SNP on adiponectin and CVD. As mentioned above, there were mixed results based on ethnicity between the SNP of adiponectin and CVD. In addition, the mechanisms of CVD were complicated by multiple factors including environmental and metabolic factors and other genetic defects. To identify the exact action of the adiponectin 45T/G polymorphism in the adiponectin gene, a larger sample study with standardized genotyping methods, homogenous CVD, and well-matched controls is needed.
In this study, we did not measure plasma adiponectin levels, so we were unable to evaluate the association between the adiponectin 45T/G polymorphism and plasma adiponectin levels. There are several factors that can affect the plasma adiponectin level, and genetic variations in the adiponectin gene can affect circulating adiponectin levels as well. Therefore, functional involvement of the adiponectin gene in inflammatory responses can be due to altered transcriptional activity.33 Few, but not all, studies have reported that subjects with the G allele have much lower plasma adiponectin levels than those carrying the T allele.3435
We also evaluated the association between the adiponectin 45T/G polymorphism with other macrovascular complications in type 2 diabetes such as peripheral artery disease and stroke. As a result, no significant association was found with peripheral artery disease and stroke.
In the present study, the GG + TG group had lower levels of HDL-C than the TT group. This result suggested that the adiponectin 45T/G polymorphism has a possible role for the development of CVD by modulating lipid metabolism. Several studies evaluated the relationship between the adiponectin 45T/G polymorphism and plasma lipids.36 Slightly higher plasma triglyceride and insulin levels were reported in the re2241766 European G allele carriers.37
Our findings suggest that the adiponectin 45T/G polymorphism is associated with diabetic cardiovascular complication in type 2 diabetes. The adiponectin genotype could be used as a susceptibility marker to predict the risk of diabetic cardiovascular complication.
 XML Download
XML Download