

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Depression and anxiety are perhaps the two most common psychological symptoms and they often coexist.1 In fact, depressive and anxiety disorders are the most common comorbid psychiatric illnesses in both general and clinical populations.23 The US National Comorbidity Survey reported 51% of patients with major depression also suffered from any anxiety disorders in the past 12 months and the lifetime prevalence was similar (58%), indicating chronicity of the comorbid anxiety condition.4 In a Dutch report, prevalence of anxiety disorder in depressed patients was 67% in the past year and 75% in their lifetime; vice versa, rates of depressive disorder in patients with anxiety disorder was 63% and 81%, respectively.3 Clinical data also replicated these results: in a large clinical cohort of anxiety disorders, 64% had current diagnosis of major depressive disorder.5 It was also found that comorbid prevalence rate of a mood disorder varies across individual anxiety disorders ranging from 15% in simple phobia to 66% in obsessive compulsive disorder.6 The negative impact of anxiety-depression comorbidity is also noteworthy: patients with these conditions have a more severe clinical condition and increased suicidal attempts and risk, implying a more negative course and more negative outcomes.1
Despite this high coexistence of anxiety and depressive disorders, there is controversy as to whether these two constructs have a single basic underlying dimension or if they are two distinct entities. Nosologically speaking, Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) considers depressive disorder and anxiety disorder different entities,7 although International Classification of Diseases, 10th revision has left one exceptional integrated zone, ‘mixed anxiety and depressive disorder,’ when anxiety or depression are concurrent but neither of them are dominant and fall short of independent diagnoses.8 Another area that needs to be understood is the co-occurrence of anxiety and depressive symptoms. For example, difficulty concentrating, insomnia, and fatigue are common symptoms both generalized anxiety disorder and major depressive disorder.7 Self-rating instruments of anxiety and depression in adults have been known to have poor discriminant validity although clinical ratings tend to better distinguish between anxiety and depression.9
One approach to determine the nature of constructs of anxiety and depression is to combine items from validated measures for anxiety and depression and to explore pertinent factor solutions. In this context, several studies have been conducted for both clinical and general population without convincing evidence as to whether anxiety and depressive symptoms are of two separate constructs or if general distress (negative affectivity) is simply a common dimension of the two ailments.
Feldman re-examined four published data sets (three undergraduate populations and one psychiatric population) that included self-reported anxiety and depressive scales and ran confirmatory factor analysis (CFA) for one- and two-factor models.10 Consequently, no differences in goodness-of-fit indices were found between the two models indicating that these anxiety and depression scales measure general negative mood rather than each symptom per se. However, Hewitt and Norton conducted an exploratory factor analysis (EFA) for 42 items from the Beck Anxiety Inventory (BAI) and the Beck Depression Inventory (BDI) in a diverse sample of 291 psychiatric patients.11 In contrast to the previous study, a two-factor solution surfaced in which anxiety and depression were separate.
Following studies with larger sample size have demonstrated both common and specific dimensions of anxiety and depression that is in line with the tripartite model12: common negative affectivity (NA), anxiety (physiological hyper-arousal), and depression (low positive affectivity). A major common factor and separate anxiety and depression has been derived from a study after analyzing 844 psychiatric outpatients and 420 college students using the BAI and BDI items.13 The two studies that follow have also reported a major common factor as well as separate anxiety and depression factors from large psychiatric populations by combining the BAI and BDI-II items.1415 Finally, results from a CFA with 137 outpatients with major depressive disorder were analyzed; a unidimensional one-factor model had a good fit, but a multidimensional two-factor model had a better fit.16
Results from the literature are inconclusive and their limitations include heterogeneous clinical diagnoses rather than a focus on anxiety and depressive disorders as well as lack of cross-cultural replication. Our previous study using EFA of Zung's self-rating anxiety and depression scales extracted seven factors explaining 56% of the variance — mainly depression, mainly anxiety, common somatic symptoms, and others — providing support for the tripartite model.17 The objective of this study was to determine whether anxiety symptoms can be empirically differentiated from depressive symptoms by conducting a single EFA of the pooled items from the BAI and BDI-II.
METHODS
Study participants
The present study used data from a questionnaire survey at a psychiatric outpatient unit of Hanyang University Guri Hospital. During a two-year period, data were consecutively (first come, first served) collected from new treatment-seeking patients who had DSM-IV diagnoses and agreed to participate in the research. Inclusion criteria were 1) a current index DSM-IV diagnosis according to the Structured Clinical Interview for DSM-IV Axis I Disorders-Clinician Version,18 2) ability to read and write, and 3) age between 18 and 65; exclusion criteria were 1) acute psychotic or substance intoxicated states, 2) neurological or cognitive disorders, and 3) a severe medical condition. A psychiatric nurse or a psychiatrist explained the purpose of the study and obtained written consents from each participant. As a result, responses from 406 patients were gathered and analyzed for this study.
Measurements
BAI
The BAI is a 21-item instrument to measure the severity of anxiety symptoms.19 It asks individuals to rate symptoms of anxiety on a four-point scale (e.g., ‘heart pounding or racing’ and ‘fear of losing control’). The total score ranges from 0 to 63, with higher scores indicating more severe anxiety symptoms. We used a Korean version of the BAI20 that proved excellent internal consistency (Cronbach's alpha = 0.91) and good discriminant validity for anxiety disorders.
BDI-II
The BDI is a 21-item questionnaire designed to assess the degree of depressive symptoms present over the two weeks' period. Each item is rated on a four-point Likert-type scale ranging from 0 to 3; its total score ranges from 0 to 63, with higher scores indicating more severe depressive symptoms. The BDI was originally developed by Beck in 196121 and revised to BDI-II in 1996 in response to changes in the DSM-IV criteria for the diagnosis of depressive symptoms.22 The psychometric properties of the BDI-II among the Korean clinical population diagnosed as DSM-IV depressive disorders showed good internal consistency (Cronbach's alpha = 0.83), excellent criterion validity with other depression measures, and a good sensitivity (0.94) and specificity (0.98) profile.
SCL-90-R
The SCL-90-R is a self-administered 90-item questionnaire with a five-point Likert Scale (1, not at all; 5, extremely often) that evaluates a broad range of psychological problems and symptoms of psychopathology in both psychiatric and medical settings. The test facilitates assessment of nine primary symptom dimensions comprising somatization, obsessive-compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. The SCL-90-R has been formally standardized from general and clinical population in Korean.23
Statistical analysis
To assess the factorial validity, an exploratory common factor analysis (principal axis factoring) with Promax rotation was conducted. The number of factors was determined by the size of eigenvalues (> 1) and the variance explained by each factor, as well as the coherence and interpretability of the factors. Items allocated to a specific factor were based on a loading of more than 0.30 on the corresponding factor, and items were excluded when the difference of factor loadings was less than 0.10.
The level of significance was set at < 0.05. All of the analyses were performed with SPSS version 21.0 for Windows (IBM Inc., Armonk, NY, USA) and R 3.4.1 (R Development Core Team, Vienna, Austria, http://www.R-project.org/) with q value packages.24 A bidirectional P value < 0.05 was considered statistically significant. Analysis of false discovery rate (FDR)25 was applied to control for experiment-wise type I errors resulting from multiple comparisons by providing an adjusted overall q-value, with adjusted P values. The FDR threshold was set to 0.05.
RESULTS
General characteristics
The demographic data of 406 participants are summarized in Table 1. Their mean age was 40.7 years (standard deviation [SD] = 15.0); over half were women (n = 232, 57.1%) and religious (n = 229, 56,4%); half were married (n = 203, 50.0%) and high school graduates (n = 206, 50.7%). Anxiety disorder (n = 185, 45.6%) and depressive disorder (n = 123, 30.3%) comprised more than three-fourths of the sample. The mean scores of the BAI and BDI-II were 23.7 (SD = 14.7) and 26.2 (SD = 12.9), respectively.
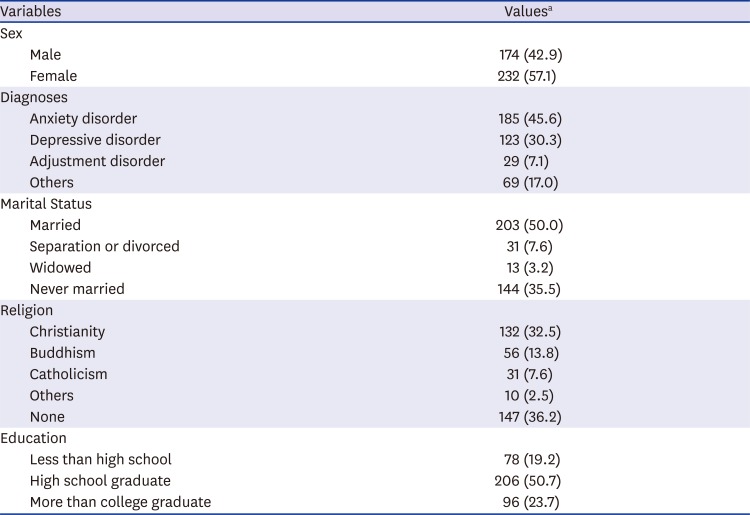
Table 1
General descriptions of participating psychiatric outpatients (n = 406)
![]()
Exploratory factory analysis
Six factors with eigen values greater than one were extracted from the combined BDI-II and BAI scales, however the last factor was ignored because it had only two items with one cross-loaded.26 The final five factors accounted for 56.2% of the total variance (Table 2). The Kaiser-Meyer-Olkin measure (0.95) and Barrett's test of sphericity (P < 0.001) have indicated that the factor structure was appropriate.
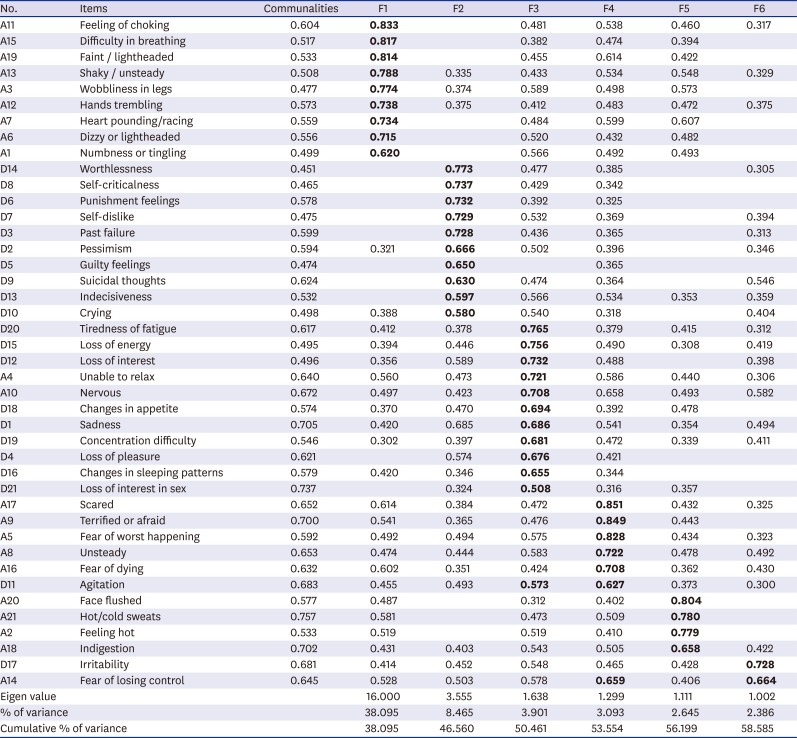
Table 2
Factor structure and loadings of 42 items from BAI & BDI-II in psychiatric outpatients (n = 406)
Salient loading values are printed in bold. Rotation method: Promax with Kaiser-Meyer-Olkin normalization. Loadings greater than 0.30 are shown. KMO = 0.950, Bartlett's χ2 = 8604.204 (P < 0.001). Factor 6 with D17 and A14 was discarded.
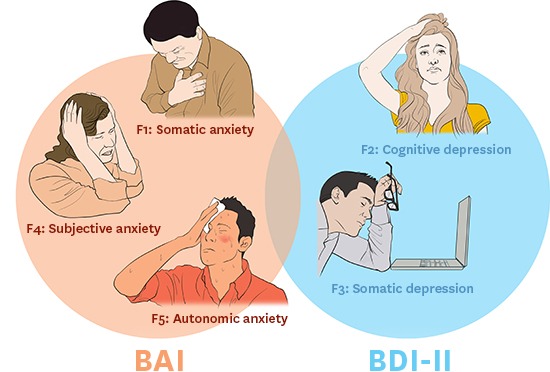
BAI = Beck Anxiety Inventory, BDI = Beck Depression Inventory, A = BAI item, D = BDI item, F1 = somatic anxiety, F2 = cognitive depression, F3 = somatic depression, F4 = subjective anxiety, F5 = autonomic anxiety.
![]()
Factor 1 (F1, somatic anxiety) consisted of nine items of the BAI associated with neurophysiological and panic-like symptoms explaining 38.1% of the total variance. It contained respiratory, skeletal, circulatory, and neurological symptoms of anxiety. Factor 2 (F2, cognitive depression) consisted of 10 items on the BDI and accounted for 8.5% of the total variance. This factor was comprised of the BDI items worthlessness, negative attitude toward self, self-criticalness, pessimism, guilt, suicidal thoughts, and indecisiveness. Factor 3 (F3, somatic depression) consisted of 11 items (nine items from the BDI and two items from the BAI) accounting for 3.9% of the total variance. Items from the BAI included were ‘unable to relax’ and ‘being nervous’; the latter cross-loaded on the following fourth factor. Factor 4 (F4, subjective anxiety) consisted of six items and explained 3.1% of the total variance. This factor was comprised of five items from the BAI and ‘agitation’ from the BDI and was also loaded on somatic depression. Factor 5 (F5, autonomic anxiety) consisted of four items: facial flush, hot/cold sweats, hot sensation, and indigestion on the BAI and accounted for 2.6% of the total variance.
Correlation analysis
Pearson's correlation analyses showed that there were significant positive correlations among these five factors (Table 3). In particular, F4 (subjective anxiety) was composed of all the BAI items except one and had the strongest positive correlation with F1 (somatic anxiety), which was composed of only BAI items (r = 0.721, P < 0.010). F5 (autonomic anxiety) was composed of only the BAI items and showed the second highest positive correlation with F1 (r = 0.698, P < 0.010). There was a significant correlation between the BAI and BDI-II (r = 0.677, P < 0.010).

Table 3
Correlation among extracted factors of BAI and BDI-II in psychiatric outpatients (n = 406)
| Factors | F1 | F2 | F3 | F4 | F5 |
|---|---|---|---|---|---|
| F1 | 1 | - | - | - | - |
| F2 | 0.422a | 1 | - | - | - |
| F3 | 0.624a | 0.701a | 1 | - | - |
| F4 | 0.721a | 0.571a | 0.671a | 1 | - |
| F5 | 0.698a | 0.428a | 0.595a | 0.612a | 1 |
BAI = Beck Anxiety Inventory, BDI = Beck Depression Inventory, F1 = somatic anxiety, F2 = cognitive depression, F3 = somatic depression, F4 = subjective anxiety, F5 = autonomic anxiety.
aCorrelation is significant at the 0.01 level (2-tailed).
![]()
There were significant correlations among all factors and nine subscales of the SCL-90-R (P < 0.010) (Table 4). Particularly, the somatization subscale of the SCL-90-R had the highest correlation with somatic anxiety (r = 0.800, P < 0.001). Cognitive depression was positively correlated with the depression subscale of the SCL-90-R (r = 0.734, P < 0.010) while F4 (subjective anxiety) was positively correlated with the anxiety subscale of SCL-90-R (r = 0.438, P < 0.010).
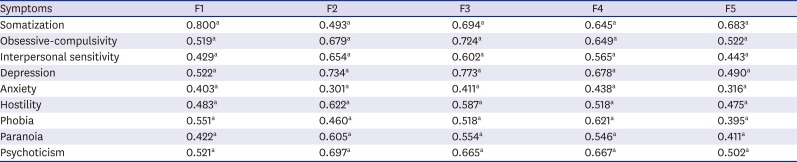
Table 4
Correlation among extracted factors of BAI and BDI-II and subscales of SCL-90-R
BAI = Beck Anxiety Inventory, BDI = Beck Depression Inventory, SCL-90-R = Symptom Checklist-90-Revised, F1 = somatic anxiety, F2 = cognitive depression, F3 = somatic depression, F4 = subjective anxiety, F5 = autonomic anxiety.
aCorrelation is significant at the 0.01 level (2-tailed).
![]()
Differences according to disease group
The depressive disorder group showed significant higher scores for all BDI items (Supplementary Table 1 and Fig. 1). When adjusted for multivariate analysis, 12 of 21 items on the questionnaires had significance (items 1, 2, 3, 5, 7, 8, 9, 10, 12, 13, 18, and 21). Some BAI items (items 4, 8, 10, 14, 18, and 20) showed higher mean scores in the depressive disorder group than those in the anxiety disorder group. When adjusting for multivariate analysis, six BAI items (items 6, 7, 11, 15, 16, 19) showed significantly higher scores in the anxiety group than those in the depressive disorder group.
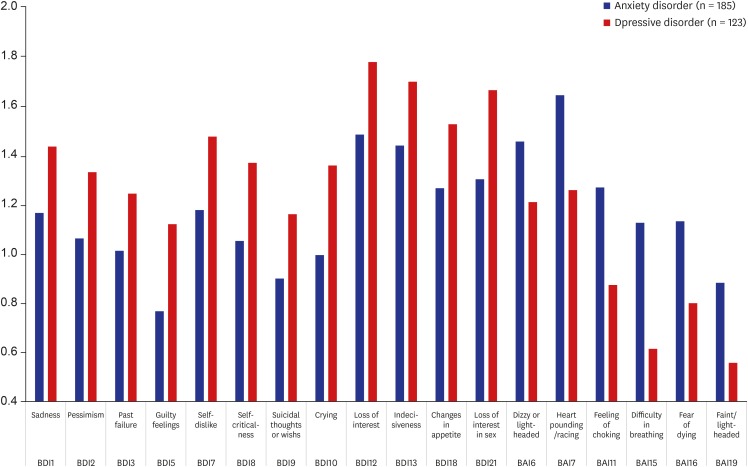
In comparison of factor score, factor 1 score was significantly higher in anxiety disorder group than depressive disorder group. Whereas, factors 2 and 3 were higher in depressive disorder group (Supplementary Table 2).
DISCUSSION
The EFA of the pooled items from the BAI and BDI, the most widely used self-report assessment tools of anxiety and depression, respectively was performed to identify the relationship between anxiety and depression. As a result, five factors were obtained: three related to anxiety (somatic, subjective, and autonomic) and two related to depression (cognitive and somatic). Two BAI items (unable to relax and being nervous) belonged to somatic depression and one BDI item (agitation) was loaded in subjective anxiety. However, being nervous and agitation had cross-loadings whose differences were smaller than 0.1. Moreover, correlations between the factors showed stronger association among factors of anxiety and among those of depression. Overall, a model of separate anxiety and depression was supported by our results.
Hewitt and Norton's EFA on psychiatric patients with mixed diagnoses11 and Enns et al.'s CFA on patients with depressive disorder16 had similar findings as ours. In contrast, Feldman's CFA on four published datasets supported one common factor of anxiety and depression.10 This discrepancy may in part be explained by exclusion of BAI among various anxiety and depression measures in the four sets of data; in fact, the data was accumulated before introduction of the scale. As such, our previous study using EFA on psychiatric patients using Zung's Self-rating Anxiety and Depression Scales yielded one common factor and others representing anxiety and depressive symptoms, respectively.17 An initial goal of developing the BAI was to establish a self-questionnaire that accurately differentiates anxiety symptoms (emotional, cognitive, and physical) from depression and the BAI displayed better discriminant validity than the other anxiety measures.19
The findings may indicate that the tripartite model should be tested in the future by comparing the goodness-of-fit in each model of the Korean clinical population. First, there exist significant correlations between factors of anxiety and depression (r = 0.4–0.7) and between the total scores of the BDI-II and BAI (r = 0.677). Second, several items cross-loaded on anxiety and depression factors and some items in BDI-II had higher scores for those with anxiety disorder. However, F1 and F5 consisted of physiological hyperarousal items, F2 was low positive affect items, and F3 and F4 were negative affect items, respectively. This study was exploratory (i.e., common factor analysis) because this is the first attempt to examine combined factor structure of the BAI and BDI measures in a sample of Korean clinical participants.
In this study, cognitive aspects of anxiety and depression emerged as separate factors, which is in line with the cognitive specificity theory of anxiety and depression by Beck.27 The theory emphasizes that cognition in depression focuses on past failure and loss while cognition tends to overestimate harm and danger in anxiety.
It is noteworthy that most items on the BDI-II that were significantly higher in depressive disorder compared to anxiety disorder were included in F2 (cognitive depression), consistent with one study on cognitive affective domains to distinguish depressive symptoms of depressive disorders from those of anxiety disorder.28 On the other hand, statistically significant BAI items die anxiety disorder all belonged to F1 (somatic anxiety).
The cognitive domain in depressive disorders and the physical domain of anxiety disorders can be key points to distinguish depression and anxiety.
Although depression and anxiety have distinct elements, they also have some common causes. Indeed, discrimination of anxiety and depression using the corresponding self-report questionnaire has limitations because the scales are highly correlated with each other.29 This study also found that two BAI items — unable to relax and nervous — loaded on F3 (somatic depression). The presence of non-discriminatory items not being characteristics of the disease suggests that a spectral approach is needed to understand commonalities in depressive and anxiety symptoms.30
Some limitations of this study are as follows. First, our sample was diagnostically mixed although 75% had either depressive or anxiety disorder and all were recruited from an outpatient unit of a single center of university-affiliated training hospital. Thus, our participants did not represent diverse groups of patients with anxiety and depression and, particularly, more severe and less economically disadvantaged patients may be under-represented. Second, only index diagnosis was considered in this study and comorbid conditions were not accounted for; our participants' disease diagnosis was based on clinical diagnosis rather than structured interviews. In addition, coexisting diseases were not considered. Third, the severity of the disease was not reflected. In the case of BDI, it is known that discrimination between anxiety disorder and depressive disorder is effective when the severity of the disorder is mild.31
Nevertheless, a strength of this study was that it integrated the evaluation of anxiety and depression from a relatively large number of clinical subjects using the widely used BDI-II and BAI questionnaires. This study supported cross-equivalence of BDI-II and BAI in that different language versions measure two separate constructs of anxiety and depression. Compared to our previous study using other tools,17 in these results also confirmed that the cognitive domain in depression and the physical domain in anxiety disorder could contribute to the differentiation of depression and anxiety characteristics. Korean psychiatric patients tend to appeal to the conflict of mind as somatic symptoms. In Korean depression patients, there were many physical symptoms and hypochondriasis such as digestive and cardiovascular symptoms.32 In our study, the inclusion of physical symptoms as major factors (F1, F3) may reflect these cultural characteristics.
To reaffirm the results of this study, CFA will be needed to use for individuals with anxiety disorder, depressive disorder, and comorbid anxiety and depressive disorders.
In conclusion, this study reported a meaningful factor solution using EFA of the Korean versions of the BAI and BDI-II among psychiatric outpatients, providing additional evidence for the differentiation of anxiety and depressive symptoms. Among them, F1 (somatic anxiety) was expressed well in anxiety disorder, F2 (cognitive depression) and F3 (somatic depression) were expressed in depressive disorder. In the future, specialized pharmacological or psychological treatments should be tailored for each symptom.
 XML Download
XML Download