

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Streptococcus agalactiae (Group B streptococcus [GBS]) is a major cause of invasive diseases such as sepsis and meningitis in neonates and early infants, globally.1 GBS is classified into 10 serotypes (Ia, Ib, II, III, IV, V, VI, VII, VIII, and IX) based on the capsular polysaccharides (CPS).2 Among these, the overall global serotype prevalence of five serotypes, Ia, Ib, II, III, and V accounted for more than 85% of serotypes in all global regions (Americas 96%, Europe 93%, and Western Pacific 89%).3
A systematic review of 74 studies conducted from 2002–2011 in developed countries reported that the mean incidence of GBS infection in infants aged 0–89 days was 0.53 per 1,000 live births and the mean case fatality ratio was 9.6%.3 Moreover, reports from Southern Africa showed much higher rates of invasive diseases (> 2 per 1,000 live births) and deaths (14%–38% of cases).45
GBS is also an important pathogen in adults, especially in pregnant women, the elderly, and the immunocompromised.67 The incidence of infectious diseases caused by GBS has been increasing among the elderly worldwide, and the mortality rate due to severe GBS disease is higher in the elderly with chronic diseases such as diabetes than in the neonates.6 An 18-year population-based analysis showed that the incidence of GBS diseases increased steadily per 100,000 populations from 3.6 in 1999 to 7.3 in 2007 amongst the elderly (15–64 years old) and from 21.5 to 26.0 amongst those ≥ 65 years.8
GBS has a number of virulence factors, including adhesion factors, toxins, as well as the CPS (which is the best-studied and most important factor for the pathogenesis). Most of the protection against GBS generally involves serotype specific opsonic antibodies mediated by phagocytic cells and complement. Baker et al.9 demonstrated that placental transfer of maternal antibodies after immunization with serotype III CPS conjugate vaccine protected neonates and young infants from invasive diseases. In the DEVANI European project, a definitive correlation between high titers of maternal anti-CPS antibodies and reduced risk of neonatal diseases from serotypes Ia, Ib, and III GBS was demonstrated.10 They also showed a statistically significant difference between the serum titers of mothers of infected babies and those of mothers of healthy babies for serotypes Ia and III.10
In a previous study, we reported the opsonization indices (OIs) of GBS Ia-, Ib-, and III-specific antibodies in the sera of Korean infants and in intravenous immunoglobulin (IVIG) products, which revealed that IVIG products had functional antibodies against three GBS serotypes; however, many infants did not.11
In this study, we extended the scope of our research by investigating the OIs of GBS II-, and V-specific antibodies as well as Ia-, Ib-, and III-specific antibodies in the three age groups (infants, adults, and the elderly) to provide seroepidemiology findings and insight into further immunization strategies in these populations.
Go to : 
METHODS
Bacterial strains
Three GBS strains (serotype Ia: E-GBS 001, serotype Ib: E-GBS 002, and serotype III: E-GBS 003) are clinical isolates recovered from the blood of infants with invasive diseases.11 The GBS type II strain ATCC 13813 (NCTC818) and type V strain ATCC BAA-611 (2603 V/R) were also used. GBS were identified based on the presence of gram-positive cocci in pairs or short chains, beta hemolysis on blood agar plates, catalase-negative results, and formation of a substance (Christie-Atkins-Munch-Petersen [CAMP] factor) that enlarges the hemolysis area formed by β-hemolysin from Staphylococcus aureus. The GBS serotypes were identified using a slide latex agglutination test (Denka Seiken, Tokyo, Japan). All strains were stored at −80°C in 0.5 mL of Todd-Hewitt broth with 15% glycerol.
Sera
Sera from infants who underwent blood testing for health evaluations between 2009 and 2010 were studied.11 Based on the available sera, 89 sera from infants who were < 1 year at the time of evaluation were selected. Infants with known immune deficiencies and infants born prematurely (gestational age of < 37 weeks at birth) were excluded. Furthermore, 35 sera from healthy adults (30–50 years old) and 62 sera from the elderly (65–85 years old) were studied after receiving each subject's written informed consent.12 In the elderly, subjects with pre-existing but stable health conditions (including well controlled diabetes mellitus, cardiovascular disease, pulmonary disease, and liver cirrhosis) were included. However, subjects with immune-compromising conditions such as human immunodeficiency virus (HIV) infection, leukemia, generalized malignancy, chronic renal failure, primary or acquired immunodeficiency, and diseases requiring immunosuppressive-drug treatments were excluded.12 Collected samples were stored frozen at −70°C until testing. All sera were found to be free from antibiotics based on their inability to inhibit the growth of R36A pneumococcal bacteria, and were incubated at 56°C for 30 minutes to inactivate endogenous complement activity before our opsonophagocytic killing assay (OPA).
OPA for antibodies against GBS (the UAB GBS OPA assay)
Duplicate samples of sera (20 µL) were serially diluted (1:3) in OPA buffer B (OBB; Hanks' balanced salt solution [with magnesium and calcium] with 0.1% gelatin and 5% defined fetal bovine serum [6000; Gibco, Waltham, MA, USA]) in 96-well round-bottom plates. Frozen working stocks of each of the target strains were thawed and washed twice with OBB and centrifuged (12,000 × g for 2 minutes), and then the bacteria were prepared in OBB to an approximate concentration of 1 × 105 colony-forming units (CFUs)/mL. Ten microliters of the bacteria were added to each well, and the plates were incubated at room temperature for 30 minutes with shaking. After the incubation, 10 μL of baby rabbit complement (BRC; Pel-Freez Biological, Rogers, AR, USA) were added to the wells, except for the control A wells, which received 10 μL of heat-inactivated BRC (heated at 56°C for 30 minutes). Forty microliters of differentiated HL60 cells (containing 4 × 105 cells) were added to all wells, and the plates were incubated for 45 minutes in a 37°C/5% CO2 incubator with shaking. Afterwards, 5-μL aliquots of the reaction product from each well were spotted onto THYA-NR plates (Todd-Hewitt agar [1.5%] with yeast extract containing neutral red [30 μg/mL] and 1 M Tris solution [0.02 M]), and the plates were incubated overnight (37°C/5% CO2). After the overnight incubation, the plates were removed from the incubator and left at room temperature for 4–5 hours, which decreased the background color. The numbers of surviving colonies on the plates were enumerated using NICE colony counting software (National Institute of Standards and Technology's Integrated Colony Enumerator; National Institute of Standards and Technology, Gaithersburg, MD, USA). OIs were calculated using linear interpolation. To facilitate the data analysis, an Excel-based data processing program was used to transfer the colony counts to an “opsonization index” program (“opsotiter3” from the UAB reference laboratory). The OI value was defined as the reciprocal of the interpolated dilution of serum that killed 50% of the bacteria. If an undiluted serum sample killed 50% of the bacteria, this produced an OI value of four in our system. A detailed protocol is posted at http://www.vaccine.uab.edu/.
Statistical analysis
The geometric mean of OIs (GMIs) and associated 95% confidence intervals (CIs) were calculated for each of the serotypes. Differences in the GMIs according to age group were analyzed using the Kruskall-Wallis test and the Mann-Whitney U test. Seropositivity was defined as the presence of detectable OI (≥ 4). Pearson's χ2 tests were used to compare seropositive rates. The χ2 test for trend was used to evaluate the relationship between the seropositive rates and age groups. The linear correlations between the OIs and age for each serotype were evaluated using Spearman's correlation coefficients. Serum samples with OIs of < 4 were assigned a value of 2 for the present analyses. Differences were considered statistically significant at a P value of < 0.05. Statistical analyses were performed using SPSS statistics for windows, version 23.0 (SPSS Inc., Chicago, IL, USA).
Ethics statement
This study protocol was reviewed and approved by the Institutional Review Board of the Ewha Womans University Mokdong Hospital (EUMC 2016-01-013, 2016-02-044). The board exempted the submission of informed consent for the use of infants' sera. Written informed consent was obtained from all the adults and the elderly subjects following detailed explanation of the study.
Go to :
RESULTS
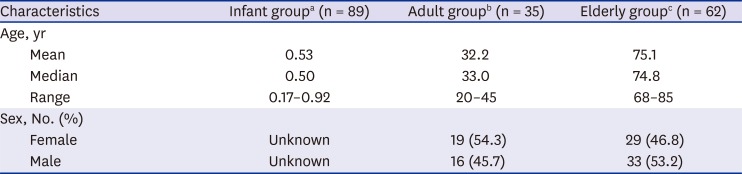
Demographic characteristics of the subjects used in this study are shown in Table 1. The mean and median age in the infant group were 0.53 years and 0.50 years, respectively. The mean and median ages in the adult group were 32.2 years and 33.0 years while those in the elderly group were 75.1 years and 74.8 years, respectively. GMIs, seropositive rate (% of subjects with OI ≥ 4) and distribution of OI in each age group against five GBS serotypes are shown in Table 2 and Fig. 1.

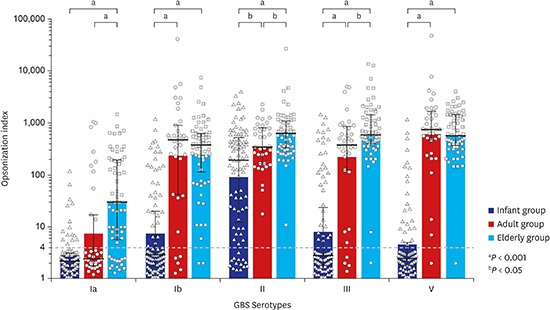
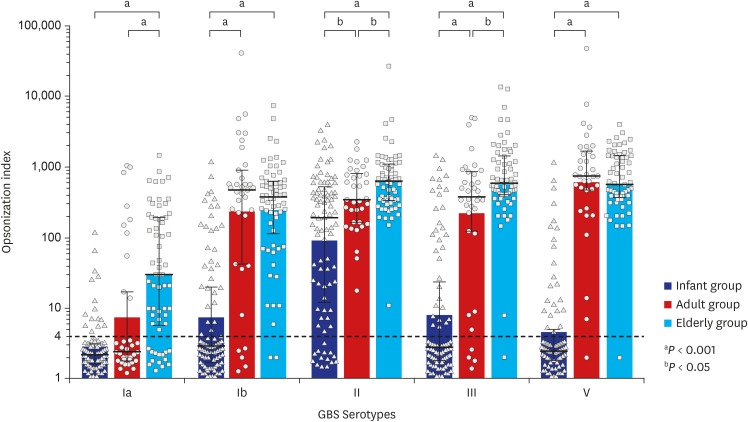 | Fig. 1Opsonization indices (OIs) against GBS serotypes by age groups. Horizontal bars represent median OIs (± interquartile range) for each age group and each serotype. Box plots indicate geometric means of OIs, while P values are for the comparison based on geometric mean differences of OIs. The lower limit of detection of OI, ‘4’ is indicated by the black dashed horizontal line.
aP < 0.001; bP < 0.05.
|
Table 1
Demographic characteristics of the subjects
![]()
Table 2
Geometric mean indices and seropositive rates of OIs against GBS serotypes by age groups
OI = opsonization index, GBS = group B streptococcus, CI = confidence interval.
aThe percentage of subjects with OI ≥ 4; bSignificantly increased according to age within each serotype (P < 0.05).
![]()
The OIs to serotype Ia GBS in the infant, adult, and elderly groups
The OIs to serotype Ia GBS ranged as follows: 2–119, 2–1,055, and 2–1,484 in the infant, adults and elderly, respectively (Fig. 1). OIs and age were moderately correlated with each other (rho = 0.55, P < 0.001). The GMIs (95% CIs) of OIs to serotype Ia GBS were 3 (2–3), 7 (3–14), and 32 (18–51) in infants, adult and elderly, respectively and significantly higher in the elderly than in the other age groups (P < 0.001) (Table 2 and Fig. 1). The seropositive rates for serotype Ia were 16.9% (15/89), 28.6% (10/35), and 77.4% (48/62) in the infants, adults, and elderly groups, respectively and significantly increased in older age groups (P < 0.001) (Table 2).
The OIs to serotype Ib GBS in the infant, adult, and elderly groups
The OIs to serotype Ib GBS ranged as follows: 2–2,486, 2–42,017, and 2–7,515 in the infant, adult, and elderly groups, respectively (Fig. 1). OIs and age were moderately correlated with each other (rho = 0.63, P < 0.001). The GMIs (95% CIs) of OIs to serotype Ib GBS were 7 (5–10), 242 (105–558), and 252 (165–383) in the infant, adult, and elderly groups, respectively and significantly higher in the adult as well as in the elderly than in the infant group (P < 0.001) (Table 2 and Fig. 1). The seropositive rates for serotype Ib were 36.0% (32/89), 85.7% (30/35), and 96.8% (60/62) in the infants, adults, and elderly groups, respectively and significantly increased in older age groups (P < 0.001) (Table 2).
The OIs to serotype II GBS in the infant, adult, and elderly groups
The OIs to serotype II GBS ranged as follows: 2–4,041, 18–2,305, and 11–17,496 in the infant, adult, and elderly groups, respectively (Fig. 1). OIs and age were moderately correlated with each other (rho = 0.50, P < 0.001). The GMIs (95% CIs) of OIs to serotype II GBS were 93 (58–149), 363 (255–516), and 676 (481–951) in the infant, adult, and elderly groups, respectively and significantly increased in older age groups (infant-adult group, P = 0.004; infant-elderly group, P < 0.001; adult-elderly group, P = 0.031) (Table 2 and Fig. 1). The seropositive rates for serotype II were 84.3% (75/89), 100.0% (35/35), and 98.4% (61/62) in the infants, adults and elderly groups, respectively and significantly increased in older age groups (P = 0.005) (Table 2).
The OIs to serotype III GBS in the infant, adult, and elderly groups
The OIs to serotype III GBS ranged as follows: 2–1,557, 2–5,063, and 11–27,185 in the infant, adult, and elderly groups, respectively (Fig. 1). OIs and age were highly correlated with each other (rho = 0.70, P < 0.001). The GMIs (95% CIs) of OIs to serotype III GBS were 8 (5–12), 212 (100–451), and 609 (471–788) in the infant, adult, and elderly groups, respectively and significantly increased in older age groups (P < 0.001) (Table 2 and Fig. 1). The seropositive rates for serotype III were 36.0% (32/89), 88.6% (31/35), and 100.0% (62/62) in the infants, adults, and elderly groups, respectively and significantly increased in older age groups (P < 0.001) (Table 2).
The OIs to serotype V GBS in the infant, adult, and elderly groups
The OIs to serotype V GBS ranged as follows: 2–1,184, 2–48,539, and 2–4,096 in the infant, adult, and elderly groups, respectively (Fig. 1). OIs and age were highly correlated with each other (rho = 0.73, P < 0.001). The GMIs (95% CIs) of OIs to serotype V GBS were 4 (3–6), 639 (346–1,181), and 610 (461–807) in the infant, adult, and elderly groups, respectively and significantly higher in the adults as well as in the elderly than in the infant group (P < 0.001) (Table 2 and Fig. 1). The seropositive rates for serotype V were 27.0% (24/89), 97.1% (34/35), and 98.4% (61/62) in infants, adults, and elderly group, respectively and significantly increased in older age groups (P < 0.001) (Table 2).
Go to :
DISCUSSION
This study was conducted to investigate the seroprevalence of functional opsonophagocytic antibodies against GBS serotypes Ia, Ib, II, III, and V in the Korean population. The seropositive rates in the infant groups were 16.9%–84.3% to five GBS serotypes, which are the lowest results in each serotype among the three different age groups. On the contrary, the elderly group showed the highest seropositivity against four serotypes. The seropositive rate against all five GBS serotypes increased significantly in older age groups.
GBS diseases cause the greatest impact in severity and incidence in the neonatal period up to the first 90 days of life.1345 Early onset (EO) GBS disease, presenting in the first six days of life, account for 60%–70% of all GBS diseases.13 Maternal carriage of GBS in the gastrointestinal and/or genital tracts is a pre-requisite for EO disease.14 In contrast, late-onset (LO) disease is acquired perinatally, nosocomially, or from community sources. Cases occurring later in infancy (age, > 90 days) are rare and generally associated with extreme prematurity.1516 In Korea, the incidence of GBS infection was not known. However, from 1996–2005, GBS was the most common pathogen of invasive bacterial infections and bacterial meningitis in immunocompetent infants younger than 3 months of age in hospital based multicenter study in Korea.1718 In the United States, the proportion of EO GBS neonatal infection cases (60%–70%)13 was higher than that of LO GBS neonatal infection cases, but in this multicenter study of Korea, the proportion of LO GBS neonatal infection cases (54.2%) was higher than that of EO neonatal infection cases (33.3%).17 GBS continued to be the common cause of invasive bacterial infection by 2013.19 In this study we found that only a limited proportion of infants have functional immunity against serotype Ia, Ib, II, III, and V GBS which confirms the vulnerability of infants to GBS infection compared to adult or elderly groups.
Furthermore, in infants, the seropositive rate for serotype II is higher than that for other serotypes, and the potential causes include transplacental antibody transfer and natural acquisition.2021 However, the seroprevalence data for GBS serotype distribution of fertile or pregnant women in Korea are inadequate. In our study, the GMIs (95% CIs) of OIs in the 19 fertile women (22–43 years old) among adult group were 6 (2–17), 172 (43–696), 360 (218–595), 261 (87–782), and 854 (395–1,847) for serotype Ia, Ib, II, III, and V, respectively (data not shown). Although the number of fertile women in our study was small to consider it as a representative of the national population, the serotype distribution of the 19 fertile women was not consistent with that of the infants. In addition, the OIs in infants were not decreased with increasing infant age; thus, it is difficult to understand with the effect of the maternal antibody. Natural acquired immunity after birth may also explain an increasing antibody pattern depending on age.21 This increasing antibody pattern should be analyzed together with epidemiological data on colonization or disease occurrence, but currently there are no domestic data available for such estimations. Further research is needed to gather epidemiological data including those on colonization of GBS and seroprevalences.
In the adult group, the seroprevalence against GBS serotype Ib, II, III, and V were high at 85.7%, 100.0%, 88.6%, and 97.1%, respectively except serotype Ia which was 28.6%. However, in the elderly group, there were high seropositive rates (96.8%–100.0%) against the above four serotypes and even a high seropositive rate against serotype Ia (77.4%). The elderly group showed significantly higher seropositive rates against serotype Ia, and III compared to the adult group. In a previous study, we reported the functional opsonophagocytic antibodies against GBS in 16 lots of IVIG products from two Korean manufacturers. The GMIs (95% CIs) were 1,018 (786–1,319) against serotype Ia, 538 (524–553) against serotype Ib, and 1,816 (1,567–2,103) against serotype III.11 However, in this study, the adult group showed GMIs (95% CIs) of OIs to serotype Ia, Ib, and III GBS as 7 (3–14), 242 (105–558), and 212 (100–451), respectively. Considering that IVIG is produced using pooled plasma from up to 100,000 donors,22 this difference in OI would be possible. In Korea, there are few systematic studies on the incidence or frequency of GBS infection in adults or elderly.23 In the USA, GBS disease incidence amongst non-pregnant adults increased significantly between 1999 and 2007, at 7.3/100,000 amongst persons aged 15–64 years and 26.0/100,000 amongst those ≥ 65 years in 2007.8 Age (adults and older age) and underlying medical conditions (such as diabetes mellitus, heart disease and malignancy) are associated with higher rates of invasive GBS disease.67824 As Skoff et al.8 suggested, we can cautiously infer that most healthy adults and the elderly may have sufficient immunity to five GBS serotypes compared to infants, however, the increasing prevalence of chronic medical conditions among adults and the elderly might enhance their vulnerability to GBS diseases. Furthermore, some adults and the elderly who lack opsonic activities against GBS may be at risk of invasive GBS infection.
Five (Ia, Ib, II, III, and V) of the ten serotypes were selected for this study since they accounted for 94% of invasive GBS disease in young infants, globally.11 In the US, most cases of invasive GBS disease are caused by these five serotypes, and accounted for 88% of cases in non-pregnant adults during 1999–2005.25 In Korea, these five serotypes accounted for 99% among invasive isolates collected from patients younger than 1 year from 1995–201526 and in pregnant women.272829 Since different populations exhibit varying serotype distributions330 and serotype changes can occur secularly, in future studies, it would be needed to expand the serotypes (including VI and VIII) in the analysis.
To our knowledge, studies on the seroprevalence against GBS CPS in various age groups have not been performed worldwide. Baker et al.31 and Edwards et al.32 reported opsonophagocytic antibodies against type III or V during the third trimester of pregnant women, while the DEVANI program described the prevalence of antibodies against CPS for Ia, Ib, and III serotypes in pregnant women.10 In non-pregnant adults, Edwards et al.32 reported a CPS-specific IgG response after invasive GBS infection in acute and convalescent-phase serum. However, as described, their study did not evaluate the functional aspect of immune responses, which is a critical limitation for the study in adults and the elderly populations. This current study was the first to show the seroprevalence of OIs to five GBS serotypes in different age groups. The advantage of our data is in the measurement of functional antibodies using OPA which is preferable to enzyme-linked immunosorbent assay (ELISA) for the evaluation of immunity in the elderly as well as the adults since IgG ELISA does not measure IgM antibodies that are opsonic.33
A limitation of this study is that the protective level of opsonic antibody against each GBS serotype is not yet known as in many other infectious diseases. However, to date, many established vaccines such as poliovirus, mumps, and pertussis vaccines are based on serological measurement of antibodies. For pneumococcal conjugate vaccine, OPA is an ideal surrogate marker for vaccine efficacy in adults and the elderly although there is limited data for the threshold of OI for protecting individuals from diseases. However, considering that serum sample from an elderly with a high OPA titer conferred considerably more protection against invasive pneumococcal disease than that from an elderly with a low OPA,34 OI differences in different age groups in this study are therefore of value.
In the future, it will be necessary to expand the research on serotypes to a larger number of subjects to be sufficiently representative of the entire population, and to study continuously by including the immune compromised and high risk groups. Moreover, GBS disease surveillance and development of suitable vaccine for these populations are needed.
There are increasing interests for the GBS diseases and vaccines from public health agencies, academia, and industries. In 2016, World Health Organization held the first technical consultation on GBS vaccines.35 As research continues and protective thresholds of OPA against various GBS diseases in different age groups are clarified further, this study is expected to provide the basic information about GBS diseases and its immunity.
Go to :
 XML Download
XML Download