

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Uveal melanoma is the most common primary intraocular malignancy in adults and retinoblastoma in children, respectively.12 Even though these primary intraocular malignant tumors have traditionally been treated with enucleation, globe-saving treatment modalities are currently encouraged.
Of these methods, PBRT is the most recently developed technique.3456 It uses charged particles with a sharp Bragg peak curve (a sharp dose deposition at a specific depth in tissue), resulting in a greater radiation dose to the target tumor with less scatter to critical adjacent normal structures.7
As for primary intraocular tumors, such as uveal melanoma and retinoblastoma, most studies have focused on evaluating treatment outcomes, such as local tumor control, survival rate, recurrence, metastasis, or prognosis, because they are relatively rare diseases, and PBRT has relatively short history as a primary treatment for intraocular tumors.34567891011 Currently, very little information is available regarding complications following PBRT for intraocular tumors, especially with respect to orbital and periorbital problems. At present, only a few studies have focused on the intraocular toxicity of PBRT, such as keratopathy, cataract, retinopathy, neovascular glaucoma, and optic neuropathy.41213 Recently in 2014, Mouw et al.4 mentioned cosmetic problems including orbital hypoplasia, hyperpigmentation, or soft tissue fibrosis over the irradiation portal, even though they did not record PBRT-related cosmetic issues in their cohort. In the current study, we present orbital and periorbital complications of PBRT in six patients with intraocular tumors, which have not previously been reported in the literature.
METHODS
Out of 24 patients with uveal melanoma and 8 patients with retinoblastoma who were treated primarily with PBRT from October 2007 to September 2014, this retrospective study analyzed 3 cases of uveal melanoma and 3 cases of retinoblastoma referred to oculoplasty clinics in Seoul National University Hospital and Seoul Metropolitan Government-Seoul National University Boramae Medical Center. Approval for conducting this study was obtained from the Institutional Review Board/Ethics Committee. Types of the adverse effects associated with PBRT and their management were evaluated.
In anophthalmic patients who eventually underwent enucleation due to disease progression after PBRT, we analyzed orbital volume (OV) changes from magnetic resonance (MR) imaging using the software program Pinnacles3 (Philips Medical Systems, Bothwell, WA, USA).
Proton beam radiation therapy (PBRT)
In uveal melanoma patients, clinical baseline visit, tantalum clip insertion, and follow-up examination took place at the Seoul Metropolitan Government-Seoul National University Boramae Medical Center. In retinoblastoma patients, clinical examination and all treatments except PBRT (chemotherapy and enucleation) were performed at the Seoul National University Children's Hospital. In all six patients, PBRT was delivered at the Proton Therapy Center, National Cancer Center in Korea. In uveal melanoma patients, a total dose of 53–60 cobalt grey equivalents (CGE) was delivered in four sessions over four consecutive days. In retinoblastoma patients, the prescribed dose was 46–50 CGE delivered in 24–28 fractions, at a rate of four fractions per week.614
Enucleation after PBRT due to disease progression
Enucleation was performed as described in our previous report.15 All enucleations were performed by one surgeon (HKC). In order to determine the size of the implant, we measured the axial length of the contralateral healthy eye in adult patients. In pediatric patients, however, it is difficult to measure the exact axial length due to poor cooperation. Therefore, in this clinic, the size of the implant is determined on the basis of age for pediatric enucleation. We usually use 18 mm spherical implants for patients under 12 months of age, and 20 mm spherical implants for patients over 12 months of age. There was one adult patient who eventually underwent enucleation and the axial length of the healthy eye was 20.88 mm. All of the three pediatric patients were over 12 months of age (3–6 years, Table 1), so all inserted orbital implants were 20 mm diameter smooth surface tunnel porous polyethylene orbital implants (Medpor® SSTTM, Stryker, Kalamazoo, MI, USA). Patients were referred to an ocularist 6–8 weeks after enucleation for prosthesis fitting.
Table 1
Demographic and clinical features of orbital and periorbital complications of the six patients with primary intraocular tumors who were treated with PBRT
OV measurement
OV was assessed from MR images using the Pinnacle3 program. Pinnacle3 was originally designed as a treatment planning system for radiotherapy, providing volumetric rendering in the region of interest of MR or computed tomography (CT) images and also automatically calculating target volume.16 In this study, isotropic T2-weighted axial images were used for volume assessment.
All measurements were repeated three times by two masked, experienced observers. The surface of the orbit was examined layer by layer in the transverse section. The OV on each section was contoured manually using the cursor to trace the orbital area excluding the eyeball of the healthy eye and the orbital implant of the sick eye. The surface area of the each layer was calculated by the Pinnacle3 software, and then summation of each surface area was calculated automatically by the program. We evaluated changes in OV before enucleation (pre-PBRT) and after enucleation surgery, and we also compared OV between both orbits.
RESULTS
Of the six patients with intraocular tumors and PBRT history, three adults were uveal melanoma patients (two choroidal melanomas and one iris melanoma), and three children were retinoblastoma patients. Among the three uveal melanomas, the one iris melanoma showed favorable response to PBRT while the other two were not controlled with PBRT and enucleation was recommended. Only one of these two patients ultimately underwent enucleation surgery. As for retinoblastoma, all three patients were previously treated with primary chemotherapy and one of them was also treated with local therapy before PBRT, but poor responses to these strategies led to enucleation. Therefore, among the six eyes with intraocular tumors treated with PBRT, only two eyes were managed with PBRT only, and the other four eyes ultimately underwent enucleation.
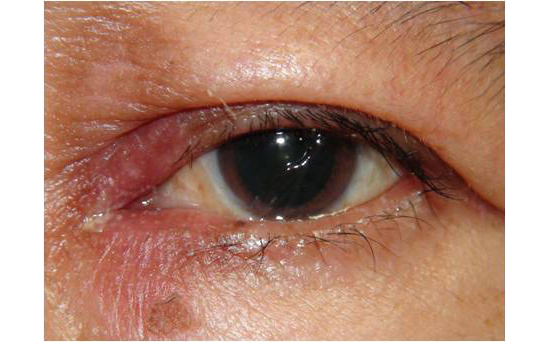
Demographics and clinical features including ocular and periocular complications of the six patients are listed in Table 1. Two eyes (cases 1 and 2) from patients with melanomas in the nasal lesion mainly suffered from radiation dermatitis and intractable epiphora (Fig. 1A and B). Case 1 was referred to the oculoplasty clinic complaining of epiphora accompanied by eyelid erythema and whitish discharge, which occurred immediately after PBRT. Under a diagnosis of canaliculitis, 1-snip punctoplasty with canalicular curettage was performed. However, symptoms did not improve. In case 2, membranous punctal obstruction was found and 3-snip punctoplasty was performed; however, epiphora persisted even after secondary punctoplasty. This patient was also referred to the dermatologist to manage radiation dermatitis and after 3 years of conservative treatment, there still remained persistent madarosis and cicatricial scarring of the eyelid skin (Fig. 1C).
Fig. 1
Eyelid and lacrimal complications of PBRT. (A) Case 1: choroidal melanoma patient treated with PBRT manifested periocular erythema, conjunctivitis, localized loss of eyelashes and high tear film meniscus due to canaliculitis. (B, C) Case 2: choroidal melanoma patient treated with PBRT manifested eyelid erythema, madarosis and increased tear film meniscus height due to punctal stenosis (B). This patient persistently complained of intractable epiphora at 3 years after PBRT despite of two times of punctoplasty. Note persistent madarosis and cicatricial scarring of eyelid skin (C).
PBRT = proton beam radiation therapy.
All four anophthalmic patients including one adult patient with uveal melanoma and three pediatric patients with retinoblastoma exhibited severe enophthalmic features with periorbital hollowness (Fig. 2). OV analysis revealed that the difference in OV between both orbits was less than 0.1 cm3 before enucleation, but after enucleation, this difference increased to more than 2 cm3 (Table 2). This result indicates that significant enophthalmos developed after enucleation. In the adult melanoma patient (case 3), OV decreased more than 2 cm3 after enucleation. When comparing OV separately before and after surgery in pediatric patients, all of them showed an OV increase in healthy eyes of more than 1.5 cm3, but OV decreased in sick eyes after surgery (Table 2).
Fig. 2
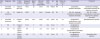
Orbital complication of PBRT presented as severe enophthalmos. (A-C) Case 3: left eye with choroidal melanoma was treated with PBRT and subsequently enucleated due to disease progression. Note severe anophthalmic enophthalmos with periorbital hollowness (A, B). This patient underwent volume augmentation with hyaluronic acid gel 6 months after enucleation; however orbital volume deficit and periorbital hollowness still remained (C). (D-F) Case 5: right eye with retinoblastoma was treated with PBRT and subsequently enucleated due to disease progression. This patient also showed severe enophthalmos and periorbital hollowness.
PBRT = proton beam radiation therapy.

Table 2
OV changes in the patient with uveal melanoma (case 3) and three pediatric patients with retinoblastoma (cases 4–6) who eventually underwent enucleation after PBRT due to disease progression

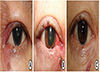
Of the pediatric retinoblastoma patients, case 4 received continuous MR imaging follow-up during a series of treatment modalities including chemotherapy, PBRT, and enucleation; therefore, OV changes in this patient could be monitored at individual stages (Fig. 3).
Fig. 3
OV changes in a pediatric retinoblastoma patient (case 4) following chemotherapy, PBRT, and enucleation. Until one year after PBRT, there was no difference in OV between both eyes; however, OV difference developed after subsequent enucleation.
OV = orbital volume, PBRT = proton beam radiation therapy, EN = enucleation, Lt = left, Rt = right, CTx = chemotherapy.
DISCUSSION
Compared with conventional photon-based radiotherapy, PBRT can decrease the dose to non-target tissues and is expected to reduce long-term side effects. Given the relatively short history and lack of availability, there are few systemic reports of the side effects of PBRT. Recently in 2014, Mouw et al.4 reported a median 8-year follow-up of disease and toxicity outcomes in a large cohort of pediatric retinoblastoma patients (49 patients, 60 eyes) treated with PBRT. Even though they experienced successful tumor control in the majority of patients, 18% of irradiated eyes were ultimately enucleated due to progressive disease or ocular complications. Moreover, 20% of irradiated eyes developed treatment-related intraocular complications, such as cataract, radiation retinopathy, glaucoma, and neovascularization. Even though they did not record PBRT-related cosmetic issues in their cohort, one-third of patients reported cosmetic problems, including orbital hypoplasia, hyperpigmentation, or soft tissue fibrosis over the irradiation portal. Also, they commented that the actual rate of cosmetic side effects from PBRT may be higher because of the lack of standardization in their cohort.
In the current study, we confirmed that PBRT can cause periorbital and orbital complications and also presented details regarding subsequent oculoplastic problems. Orbital and periorbital complications of PBRT can be classified into two categories: 1) eyelid and lacrimal complications, and 2) severe enophthalmos, which was observed in all anophthalmic orbits that underwent PBRT followed by enucleation.
As for lacrimal complications in the present study, the two patients with uveal melanoma nasal lesions whose puntae lay in the PBRT radiation field, also showed membranous punctual obstruction or canaliculitis. It is thought that damage caused by PBRT to the conjunctiva or to the canalicular epithelium might have resulted in the chronic inflammation. Such inflammation causes persistent punctal obstruction, intraluminal adhesion, and scarring, eventually leading to obstruction of the lacrimal drainage system. Therefore, prophylactic lacrimal stenting and steroid use in early stages might prevent lacrimal drainage obstruction.
As for the second type of complication, severe enophthalmos and periorbital hollowness is the most attention-attracting complication of PBRT that developed in all four anophthalmic sockets post-PBRT followed by enucleation. There have been many studies reporting enophthalmos as a rare complication of enucleation over a long follow-up period, as long as an appropriately sized orbital implant was inserted.15161718192021222324 In our study, properly sized orbital implants were inserted in all patients at the time of enucleation. For pediatric enucleation, our clinic usually uses 18 mm spherical implants for patients under 12 months of age, and 20 mm spherical implants for patients over 12 months of age15; these sizes are considered larger than what is typically recommended or used in other clinics.2021 We have already reported good surgical outcomes following enucleation with Medpor® SSTTM in children with retinoblastoma.15 In that study, we reported that only 2 of 44 consecutive pediatric patients showed severe enophthalmos greater than 2 mm during an average follow-up period of 5 years. One of these patients was a pediatric patient included in the present study who received PBRT before surgery (case 6), and the other was a pediatric patient who received enucleation 4 months after birth with the insertion of an 18 mm orbital implant. It is notable that the present research showed that severe enophthalmos occurred in all three pediatric patients who had received both PBRT and enucleation, in contrast to the previous study that reported only one patient (2.6%) with severe enophthalmos who underwent enucleation without PBRT. It implies that PBRT itself has effect on the development of enophthalmos in anophthalmic socket.
With respect to the effect of conventional radiotherapy on the pediatric anophthalmic socket, Shildkrot et al.25 reported 135 anophthalmic sockets treated with systemic chemotherapy and/or orbital external beam radiation therapy (EBRT) before or after enucleation compared with patients who received primary enucleation only and revealed that during the median follow-up period of 3.6 years, socket contracture was 0% in the primary enucleation group, 8% in the adjuvant chemotherapy group, and 50% in the group receiving a combination of chemotherapy and EBRT group. Although they did not report when the socket contraction occurred with respect to treatment, they concluded that EBRT greatly increased the risk of contracture. Even though the radiation treatment modality was not PBRT but conventional radiotherapy (EBRT), this is a meaningful study to determine the impact of radiation therapy on the pediatric anophthalmic socket.
Case 4 is a very interesting case who definitively demonstrated the effects of PBRT on the orbit (Fig. 3). After chemotherapy and PBRT, there was no difference in OV between both eyes; however, a remarkable OV difference developed after subsequent enucleation. As mentioned above, as long as proper surgical techniques and a proper sized implant are used, enophthalmos is generally not prominent after primary enucleation. Interestingly, in this pediatric patient, chemotherapy and PBRT by themselves did not affect the growth of OV during at least 1 year following PBRT, but subsequent enucleation surgery lead to an ultimate reduction in OV growth even though proper surgical techniques and a proper implant were used. Similarly, two uveal melanoma patients who had received only PBRT without enucleation did not show any enophthalmos, but the patient who had received PBRT and subsequent enucleation developed severe enophthalmic feature. Based on these data, we hypothesize that atrophy of orbital tissue, which is a later effect of radiation, does not cause enophthalmos provided the eyeball is maintained normally, but atrophy of orbital tissue became prominent in the anophthalmic socket after enucleation. In addition to OV changes, periorbital hollowness caused by atrophy of the periorbital tissue also became prominent.
The physical advantages of PBRT over conventional photon-based radiotherapy (EBRT) are illustrated in Fig. 4.26 The dose distribution from a single proton field targeting a retinoblastoma is compared to the dose distribution from a single conventional photon field. In this example, the dose proximal to the tumor within the eye is much greater for the photon field. Also, the dose distal to the tumor within the posterior orbit and brain is much higher. From this physical advantage, PBRT derives its main clinical benefit: less normal tissue is irradiated. Therefore, Proton beam is much less intense in the posterior part of the orbit than conventional EBRT. In this reason, severe cosmetic complication such as hourglass facial deformity, a well-known complication of conventional radiation treatment,27 does not occur. However, although the proton beam has a lower radiation dose than the conventional photon beam, the influence of radiation on the normal tissues of anterior orbit, which are proximal to the intraocular tumor, cannot be avoided. Radiation effects may not be noticeable in situations where the eyeball is maintained, but it is thought that tissue damage and subsequent fibrosis accelerated the orbital atrophy after iatrogenic surgical trauma of enucleation, and enophthalmic features may eventually be maximized.
Fig. 4
A comparison of proton beam and conventional photon beam treatments for retinoblastoma. The photon field (A) has a higher dose proximal to the target and a significant exit dose beyond the target into the posterior orbit and temporal lobe, which is absent in the proton field (B).

There are several limitations to our study. For instance, this study is not a prospective cohort study of intraocular tumors treated with PBRT, but a case series of intraocular tumor patients treated with PBRT and referred to the oculoplasty clinic due to periorbital or orbital complications. Therefore, we were unable to compare OV before and after PBRT in all patients. Secondly, patients treated only with PBRT did not receive MR or CT imaging after PBRT and thus we were unable to analyze the isolated PBRT effect on OV, although they did not show significant enophthalmos. In patients who received enucleation, time from completion of PBRT to enucleation was relatively short (less than 1 year), and the possibility that orbital atrophy did not yet become evident before enucleation cannot be excluded. Therefore, it is difficult to assess the long-term effects of PBRT alone by eliminating the contribution of enucleation on OV loss. As for the two adult patients who underwent only PBRT and did not exhibit enophthalmic features during the 2–3 years follow-up, their lesions were limited to the nasal area and it is possible that PBRT did not influence posterior orbital tissue and subsequently did not cause enophthalmos.
In conclusion, PBRT is expected to be superior to conventional radiation therapy with respect to protecting normal surrounding tissues, yet it can still cause radiation-related orbital and periorbital complications and therefore careful orbital examination before and after treatment is mandatory. Given the possibility of lacrimal complications after PBRT aimed at anteromedial tumor locations, early evaluation of the lacrimal drainage system and proper consultation with oculoplastic clinic is highly recommended. If the irradiated eye is ultimately subjected to enucleation due to disease progression, it should be kept in mind that significant enophthalmos that can affect facial cosmesis may result.
 XML Download
XML Download