

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In 2006, an undifferentiated type of fatal children's interstitial lung disease was observed in Korea.123 Subsequent nationwide epidemiologic and animal studies linked toxic chemicals in humidifier disinfectants (HDs) to the development of serious lung injury (LI).456789
HDs contain polyhexamethylene guanidine (PHMG), oligo (2-[2-ethoxy]ethoxyethyl) guanidinium chloride (PGH), 5-chloro-2-methyl-4-isothiazolin-3-one (CMIT), or 2-methyl-4-isothiazolin-3-one (MIT).10 In previous experimental studies,411 it was reported that PHMG and PGH could cause lung injuries, which are defined as HD-associated lung injuries (HDLIs).12 However, animal studies have not established definitive links between exposure to HDs containing CMIT and/or MIT and the development of HDLI, even though patients exposed to HDs containing only CMIT and/or MIT showed clinically similar LIs to those seen after exposure of individuals to HDs containing PHMG and/or PGH. Due to the lack of evidence on the inhalational toxicity of CMIT and/or MIT in animal and human studies, victims with CMIT/MIT exposure-associated LIs were not legally protected.
Victims with HDLIs were most commonly exposed to HDs containing PHMG (76.5%), followed by HDs containing PGH (8.8%) and those containing a mixture of other components with CMIT/MIT (7.2%).1314 However, only two of the HDLI victims were exposed to HDs containing only CMIT/MIT.
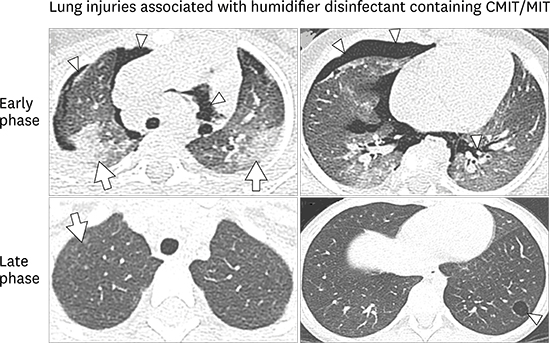
Generally, HDLIs are characterized by rapid progression of respiratory difficulty without causative factors and the presence of ground-glass opacities, spontaneous air leak syndrome, and consolidation with later diffuse centrilobular nodular opacity on chest computed tomography (CT).81516 On lung biopsy, bronchiolar destruction and centrilobular distribution of alveolar destruction with subpleural sparing were predominant in these patients.817 Here, we report two cases of HDLIs after exposure to HDs containing only CMIT/MIT that developed in twin sisters. The twin sisters were exposed to only one kind of HD product featuring only CMIT/MIT mixtures.
CASE DESCRIPTION
Case 1
The patient is the younger twin sister of case 2. She was previously healthy. She had been exposed to HDs containing CMIT/MIT alone from 4 months of age to 6 months of age. Exposure assessment was performed by experienced experts using a questionnaire and supporting evidence of the purchase of HD.5614 Investigation methods for usage of HD are described elsewhere in detail.13
At 6 months of age, she presented with a 3-day history of cough, sputum, and respiratory difficulty on April 11th, 2012. She showed an acutely ill-looking appearance. On physical examination, she was apyrexial and tachypneic and lung sounds were decreased with chest retraction. Chest radiography and chest CT revealed multiple patchy consolidation and ground-glass opacities in both lungs with pneumothorax and pneumomediastinum (Fig. 1A and B). Arterial blood gas analysis (ABGA) showed no hypoxemia or hypercapnia. Her total white blood cell count was 11,040/μL with 64.1% neutrophil and 29.1% lymphocytes. Multiplex reverse transcription polymerase chain reaction (RT-PCR) of nasopharyngeal aspirates revealed the presence of influenza B infection. A lung biopsy was not done. Thoracostomy was performed due to pneumothorax at admission and she was discharged at 11 days of hospitalization.
 | Fig. 1Chest radiography and computed tomography (CT) of case 1. (A, B) At 6 months of age, initial chest CT (1-mm-thick axial images) showed extensive air leakage (arrowheads) indicating pneumothorax, pneumomediastinum, and pulmonary interstitial emphysema. Patchy consolidations (arrows) and ill-defined ground-glass opacities are also noted. (C, D) After 3 years, larger, subtle ground-glass opacities with air trapping, suspicious ill-defined centrilobular nodules (arrow), and a small air cyst (arrowhead) remained. (E, F) At 5 years of age, multiple tiny and faint centrilobular nodules (arrow) in both lungs and a small air cyst (arrowhead), possibly a pneumatocele, remained in the basal segment of the left lower lobe.
|
At 8 months of age, she was hospitalized with acute bronchiolitis. During the hospitalization, she presented with chest retraction, tachypnea, and desaturation. However, there was no air leak syndrome on chest radiography. Follow-up chest CT scan, performed at 3 years of age, showed tiny ground-glass opacities in both lungs (Fig. 1C and D). At 5 years of age, multiple tiny nodules and faint centrilobular ground-glass opacities in both lungs were observed with the presence of small pneumatocele on chest CT (Fig. 1E and F). She is healthy but reports intermittent wheezing after exercise.
Case 2
This patient is a previous healthy 12-month-old girl who visited a tertiary hospital due to dyspnea on November 3rd, 2012. She had cough, rhinorrhea, and mild fever for 7 days before the hospital visit. She had been exposed to HD containing only CMIT/MIT in the same concentration during the same period with her sister (case 1). According to her aunts' statement, she was kept away from HDs after her elder sister's hospitalization at 6 months of age. The cumulative exposure dose was 19.56 g/m3.13 Her respiratory difficulty had aggravated 2 days before hospitalization. At admission, saturation was 93% and recovered with application of 0.5 L/min oxygen via a nasal prong. She showed an acute ill appearance at admission. On physical examination, a coarse breathing sound was auscultated without definite rales or wheezes. In her family history, her younger twin sister experienced sudden onset of dyspnea, cough, and mild sputum at 6 months old. When her sister visited a tertiary hospital, extensive pneumothorax and pneumomediastinum without identified causes of the air leak syndrome was observed. During her younger sister's hospitalization, an aunt raised this girl.
ABGA showed mild hypoxemia with no hypercapnia. Her white blood cell count was 4,630/μL with 44.5% neutrophil and 43.0% lymphocytes. Respiratory RT-PCR using sputum samples revealed the presence of respiratory syncytial virus at admission. Her chest radiography and CT revealed consolidation in both lung fields and pneumomediastinum, air trapping, and pulmonary interstitial emphysema in the right lung field (Fig. 2A and B).
 | Fig. 2Chest radiography and computed tomography (CT) of case 2. At 12 months of age, (A) initial chest radiography and (B) a 1-mm-thick axial CT image revealed diffuse ground-glass opacities and suspicious pulmonary interstitial emphysema (arrows) in both lungs and pneumomediastinum (arrowheads). (C, D) After 2 months, diffuse ground-glass opacities and patchy consolidations (arrows) along the bronchovascular bundles were noted, and several air cysts are visible (arrowhead). (E, F) After 5 years, subtle ground-glass opacities and multiple tiny ill-defined centrilobular nodules (arrows) were still evident in both lungs.
|
On the 6th day of hospitalization, pneumomediastinum was observed in the left lung on chest radiography. The patient required mechanical ventilation for a total of 50 days. Even with the administration of five cycles of high-dose methylprednisolone (20 mg/kg, 3 consecutive days) and high-dose immunoglobulin during ventilator care, extubation failed with three attempts. On the 55th day of hospitalization, after the third failed extubation, a tracheostomy was performed. On follow-up chest CT on the 60th day of hospitalization, a patchy consolidation along the bronchovascular bundles was observed with air bronchogram and multiple lung cysts (Fig. 2C and D). At 5 years of age, chest CT revealed ground-glass opacity and multiple tiny centrilobular ground-glass opacities nodules in both lungs (Fig. 2E and F).
The patient reports dyspnea and tachypnea during exercise. Decannulation was attempted when she was 5 years of age. A pulmonary function test was not performed due to the tracheostomy. Her height and weight are at the 25th percentile for her age.
DISCUSSION
We report two cases of HDLI after exposure to HDs containing CMIT/MIT alone in twin sisters. Although the evidence for the development of HDLI after exposure to HD containing CMIT/MIT alone in animal studies is lacking, these case reports support the belief that CMIT/MIT can cause HDLIs in those exposed to HDs containing these chemicals, similar to HDLIs caused by exposure to PHMG or PGH.8
Cases of HDLI are typically characterized by rapid progression of respiratory difficulty, starting from mild cough or tachypnea, without any definitely identified causes,38 which is consistent with the features of the present two cases. On chest CT, chronological changes include consolidation to centrilobular opacities with subsequent faint centrilobular nodules.815 Spontaneous air leak syndromes, observed in 26%–44% of HDLI patients according to the disease course,1517 were seen in both of the patients in the present report. However, the interval between HDLI development in the two sisters might be associated with reduced attention paid to case 2 due to the hospitalization of case 1 and subsequent aggravation of respiratory symptoms combined with respiratory syncytial virus infection in case 2. Respiratory viral infection was itself not the direct cause of the LIs in the present study considering the unusually rapidly progressing respiratory failure and only partial detection of respiratory viral infection in a cluster of other HDLIs.317 A time-lag between exposure to HDs and onset of HDLIs in case 2 might be associated with lack of additional information on exposure to HDs due to remote memory on the periods of HD usage or a viral infection as a triggering factor of the expression of HDLIs with underlying unidentified or indistinctive symptoms. The possibility of HD usage after 6 months of age could not be completely ruled out in case 2.
The isothiazolinones in CMIT/MIT have biocidal properties and are therefore usually found in perfume, air conditioning systems, and HDs.18 In previous studies,1920 CMIT/MIT in paint and cosmetics were found to cause airborne allergic contact dermatitis. However, there are no studies of the respiratory health effects of CMIT/MIT inhalation in either animals or humans. A 53-year-old chemical operator was reported to develop asthma 5 months after beginning work in an isothiazolinone manufacturing plant.21 Unpublished experimental data showed that exposure to HDs containing a mixture of CMIT and MIT was not associated with LIs,22 despite the presence of cases of HD containing CMIT/MIT-associated LI, as in the present cases.
Aside from the previous studies on the effect of cutaneous exposure to CMIT/MIT, one previous study found harmful effects of CMIT/MIT inhalation in the respiratory system in humans,23 demonstrating that exposure to HDs containing CMIT/MIT causes peripheral airway dysfunction without bronchial hyperreactivity, especially in children who inhale high levels of CMIT/MIT. The results of that study suggested the possible mechanisms of the peripheral airway dysfunction, namely, bronchiolar destruction with alveolar damage, in response to inhalational exposure to CMIT/MIT.23 One other published experimental study on CMIT toxicity using rat alveolar macrophages and NR8383 cell lines reported that treatment with CMIT markedly inhibited phagocytic oxidative bursts and cellular cytokine secretion, causing toxic respiratory effects.24 The production of oxidative stress and changes in the expression of oxidative stress-related genes after exposure to toxic chemicals in HD, such as PHMG/PGH and CMIT/MIT, might be a common pathway in the development of HDLIs.122526
The estimated exposure intensity to HDs in cases of CMIT/MIT-associated LIs in the present study (mean, 82 µg/m3) were far lower than that of PHMG or PGH exposure associated LI cases (mean, 900 µg/m3).13 This may explain the lower prevalence of HDLIs in victims exposed to HDs containing CMIT/MIT alone, as well as the differences in toxicity levels by types of HD. In addition, the health effects of CMIT/MIT might differ according to species, susceptibility, receptor, exposure dose, and duration.27 More sophisticated and elaborate experimental studies are currently underway, because further studies of the respiratory health effects of CMIT/MIT inhalation are needed to limit their harmful effects.
In summary, we report two cases of LIs linked to HDs containing CMIT/MIT alone, although experimental evidence and mechanisms explaining the harmful respiratory effects of CMIT/MIT are still lacking. This issue requires attention to prevent the occurrence of additional harmful respiratory diseases caused by CMIT/MIT inhalation.
 XML Download
XML Download