

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Although deaths in bathtubs have been reported worldwide,123456789 most of studies of bath-related deaths have been performed in Japan.56789 This focus is likely explained by the fact that the head-out-of-water immersion style while sitting in a bathtub filled with hot water is part of the traditional lifestyle. Moreover, an increasingly aging society may also be associated with the high prevalence of bath-related deaths in Japan. In Korea, bath-related deaths are also likely to increase owing to the high popularity of public spas (jjimjilbangs) as well as the recent rapid growth of the elderly population. However, the decision to perform a medico-legal autopsy in Korea is ordered by public prosecutors employed by the Ministry of Government Administration and Home Affairs; hence, the autopsy rate is extremely low (1.6%).10 Therefore, no coronial investigations for bath-related deaths have been conducted in Korea, and no information is available regarding the risk groups and risk factors for bath-related deaths that would enable the development of preventive strategies.
Bath-related deaths could raise medico-legal issues related to the manner and cause of death, which determines adjustments for life insurance. Although bathtub drowning has been regarded as one of the leading causes of death in bathtubs, general physicians sometimes issue death certificates for hospital-referred drowning victims without precise assessment of the cause of death. Furthermore, the diagnostic criteria for bathtub drowning have not been established among pathologists internationally, which causes additional confusion.6
In this study, 84 bath-related deaths that occurred between January 2008 and December 2015, as derived from a nationwide registry in Korea, were analyzed. We investigated pathological findings in victims of bathtub-related deaths as well as police reports. The drowned subjects' medical histories as well as photographs of the scenes were investigated to determine the criteria for diagnosing bathtub drowning, and to identify the risk factors associated with bath-related deaths. Our study thus aimed to shed light on an important public health issue in Korea.
METHODS
The cases analyzed were collected from a nationwide pool of bath-related deaths that occurred between January 2008 and December 2015. The inclusion criterion was that individuals had died in a water-filled bathtub. From 31,123 autopsy records obtained over 8 years, 84 subjects who satisfied the inclusion criterion were identified. All individuals were found unresponsive in a bathtub with their faces submerged. Any subject showing signs of trauma were excluded from this study. We collected data on the victim's medical and psychosocial history as well as autopsy findings that included toxicological data for drugs and alcohol.
Specimens for toxicology were obtained from heart blood (right ventricle) and/or peripheral blood (femoral vein). Drug screen tests were performed using gas chromatography-mass spectrometry. The blood alcohol concentration (BAC) was analyzed by headspace gas chromatography.
The degree of coronary atherosclerosis was determined by a forensic pathologist as minimal, mild, moderate, or severe based on cross-sectional luminal narrowing (stenosis) by the atherosclerotic plaque. The overall reported degree of coronary artery disease was based on the most advanced degree of atherosclerosis found in the three major coronary artery branches. Coronary atherosclerosis greater than 75% was considered to be significant, as previously described.7 The degree of cardiac hypertrophy was analyzed using the calculated normal heart weight based on a previously reported equation.11 We considered a ≥ 20% degree of cardiac hypertrophy as significant.
We also compiled data that were indicative of water-inhalation based on previously reported bath drowning reports,4712 including the following: froth in the air passage space, hyperinflated lung (aqueous emphysema), watery fluid in the sphenoid sinuses, Paltauf's spots (subpleural hemorrhages), and watery fluid in the stomach and/or duodenal contents. To evaluate the factors leading to bath-related death, we divided the deceased into two groups: those determined to have died of drowning in the bath and those who died of other causes.
RESULTS
Demographic findings of bath-related death
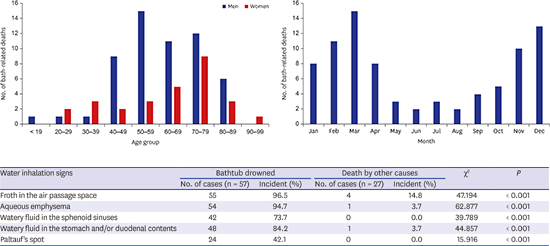
Between January 2008 and December 2015, 84 deaths (56 men and 28 women) were found to have occurred in bathtubs. As shown in Fig. 1, the individuals' ages ranged from 18 to 91 years, with a mean age ± standard deviation of 61.3 ± 16.0 years. Forty-seven individuals were older than 60 years (29 men and 18 women). No significant age difference was found between men and women.

As shown in Fig. 2, more deaths occurred in the winter and early spring (November to March). The number of drownings in the winter (December to February; n = 32) was approximately 4.6-fold higher than those in the summer (June to August; n = 7). Table 1 shows the settings in which the deaths occurred; a majority of subjects (n = 67.9%) were found in communal baths, followed by the home (n = 20.2%).

Table 1
Types of setting in bath-related death (n = 84)

| Type of setting | No. (%) |
|---|---|
| Home | 17 (20.2) |
| Hotel or motel | 10 (11.9) |
| Communal bath | 57 (67.9) |
![]()
The interval between the time that the individual started bathing and the time of death in the bathtub was determined by police investigation reports. Of the 62 victims with available data, 9 (14.5%), 18 (29.0%), 23 (37.1%), and 12 (19.4%) had intervals of < 15 minutes, 15 intervals of < 15 minutes, and > 60 minutes, respectively.
Autopsy findings in bath-related deaths
The postmortem interval (PMI) was calculated from the time the individual was last seen alive to the time of the autopsy. Of the 84 individuals, 12 had PMIs < 24 hours, 63 had PMIs of 24–48 hours, and 10 had PMIs of 48–60 hours.
The primary cause of death in 57 of the 84 individuals in this study (67.9%) was found to be drowning in the bath; 24 (28.6%) were found to have died of other causes (including natural diseases), and 3 (3.6%) died of acute alcohol intoxication. Table 2 shows the relationship between the determined cause of death and the presence of water inhalation signs. Of the 57 individuals who diagnosed as drowning in a bathtub, froth in the airway passage was found in 55 (P < 0.001); the same was found in 4 of 27 (14.8%) individuals in the non-drowned group; these were associated with one case of acute alcohol intoxication, one case of subarachnoid hemorrhages, and two cases of ischemic heart disease. Hyperinflated lung and watery gastric contents were found in two respective individuals with ischemic heart disease in the non-drowned group. Findings of watery fluid in sphenoid sinuses and Paltauf's spots were only observed in the bathtub drowned group. There were significantly greater incidences of hyperinflated lungs, fluid in the sphenoid sinus and stomach/duodenal contents, and Paltauf's spots in the bathtub drowned group than in the non-drowned group (P < 0.01). As shown in Table 3, multiple signs of water inhalation were significantly correlated with bathtub drowning (P < 0.01).
Table 2
Comparison of water inhalation signs between individuals determined to have drowned in a bathtub vs. those that died of natural diseases

![]()
Table 3
Evaluation of water inhalation signs in the determination of bathtub drowning in the victims with their face submerging under the bath water at the scene

![]()
Postmortem examination revealed that various pathologic findings that contributed to deaths in the bathtub (Table 3). The most common contribution to the cause of death was a severe degree of coronary atherosclerosis, including myocardial ischemia and cardiomegaly, which was observed in 43 (75.4%) and 22 (81.5%) individuals in the drowning and non-drowning groups, respectively. Subarachnoid hemorrhage and a history of seizure-inducing disorder were confirmed in 1 and 2 victims of bathtub drowning, respectively, whereas 2 individuals who experienced subarachnoid hemorrhages were not classified as having drowned in the bathtub based on postmortem examinations. There was no significant difference in the prevalence of cardiovascular disease between the drowning and non-drowning groups. Two individuals with drug intoxication showed no signs of water inhalation.
The BAC was analyzed in all individuals (Table 4). Postmortem examination revealed that 29 of all 84 victims (34.5%) had alcohol in their blood. The mean BAC was 0.169%, ranging from 0.017% to 0.508%, and 27 (93.1%) blood-positive individuals exceeded a BAC of 0.08%. The difference in the BAC between the drowning and non-drowning groups was statistically significant (P < 0.05).
Table 4
Contributory causes of deaths confirmed in postmortem examination
BAC = blood alcohol concentration.
aHypertrophic cardiomyopathy (n = 1); bAortic dissection (n = 1) and valvular heart disease (n = 1); cAmitriptyline and zolpidem (n = 1) and amitriptyline, zolpidem and sertraline (n = 1); dThere were no individuals with blood alcohol levels between 0.050% and 0.079%.
![]()
DISCUSSION
Recently, the role of forensic pathologists has expanded beyond criminal justice service to involve public health and safety. Forensic pathologists are in a unique position to clarify the cause and manner of sudden unexpected death via autopsy; hence, forensic pathologists are frequently required to testify in courts or provide consultations regarding cases of sudden unexpected deaths. The population in Korea is rapidly aging, as lifespans have continued to increase owing to developments in modern medical science. Additionally, the high popularity of public spas could result in bath-related deaths that require investigations by forensic pathologists.
To our knowledge, this study is the first to investigate bath-related deaths in Korea. Our study of the age distributions showed that Korean individuals who experienced bath-related deaths tended to be younger than those in Japan, in which most victims consisted of elderly individuals older than 65 years. However, consistent with previous studies, the majority of bath-related deaths in our study were observed during the winter season.56789 The reason for this has been suggested to be the thermal difference between low environmental vs. higher room temperatures, which could affect cardiovascular function including heart rate, ventricular contractility, vascular resistance, and blood pressure.1314 Most previous studies showed that bath-related deaths occurred while the victims were in tubs filled with hot water in a private bathroom.56789 In our study, the majority of victims were found in communal baths; since public spas such as jjimjilbangs are open 24 hours a day, many Koreans visit jjimjilbangs after drinking or working overnight to regain sobriety and cure hangovers through bathing. This could explain why victims of bath-related deaths were relatively younger and were more often found in communal baths, in contrast to Japan. Considering these factors, the decision to perform a medico-legal autopsy in Korea is determined by public prosecutors, and the autopsy is typically performed if warranted, as in suspicious deaths associated with a likely crime. Therefore, there is also the possibility that victims in younger age groups who were found in communal baths were more likely to receive autopsies compared to those who died in different settings.
Although we selected individuals whose faces were submerged in bath water at the scene, 27 deaths (32.1%) were not attributed to drowning based on the scene investigations, victims' medical histories, and autopsy findings. In 57 individuals classified as having drowned, having more than two signs of water inhalation was significantly correlated with bathtub drowning, while the absence of water inhalation signs indicated that the cause of death was a natural disease. Our data revealed that froth in the airway was not specific to bathtub drowning; the development of froth could have resulted from deaths from other causes such as sudden cardiac death.
Among the individuals analyzed in this study, the most common primary cause of death according to autopsy reports was drowning followed by cardiovascular disease and alcohol and drug intoxication. The most common contributor to the cause of death in both bathtub drowning and non-drowning events was ischemic heart disease, including severe coronary atherosclerosis and/or cardiac hypertrophy. These findings indicate that cardiac lesions appear to be the most important risk factor associated with bath-related deaths. A plausible theory to explain sudden deaths of individuals with cardiac lesions in bathtubs is that they could experience ventricular tachycardia and ventricular extrasystole, or else gradually decreasing blood pressure with a decrease of resistance in peripheral blood vessels, which could lead to a sudden death in vulnerable people.1415
Other than cardiac lesions, acute alcohol intoxication (more than 0.30% of BAC) were observed in three individuals who drowned as well as in three whose causes of death were not drowning. Furthermore, most (93.1%) of blood alcohol-positive individuals exceeded a BAC of 0.08%. Binge drinking, a prevalent pattern of alcohol intake accounting for more than 75% of alcohol consumed,16 is defined by the National Institute on Alcohol Abuse and Alcoholism as consuming more than four or five alcoholic beverages within two hours and a BAC elevated to > 0.08%.17 It is normally preceded by a loss of consciousness owing to the effects of alcohol. Acute alcohol intoxication could cause increased interatrial electromechanical delay before death in a bathtub.18 Therefore, alcohol consumption before bathing ought to be emphasized as a risk factor for bath-related deaths.
The diagnosis of bath-related deaths raises medico-legal questions regarding the determination of the primary cause and manner of death, since no consistent criteria have been defined for the distinction between death of natural diseases while in a bathtub vs. actual bathtub drowning; this has impacted adjustments of life insurance. Furthermore, two considerable problems remain with respect to determining the cause and manner of death in a bathtub. First, the autopsy rate in Korea is extremely low (1.6%) compared to other countries,19 and most bath-related deaths are assessed by a general physician. If such physicians do not have sufficient postmortem examination expertise, they may consider these deaths as a progressive collapse due to preexisting diseases (including cardiovascular diseases) and issue death certificates based on the previously diagnosed illnesses of the victims. Second, even after a full autopsy, the precise cause of death can remain unclear since a certain proportion of autopsies show no pathological and toxicological findings; furthermore, swallowing small amounts of water can stimulate laryngeal spasms mediated by the vagal reflex, which could lead to drowning.20 Considering the autopsy rate, the number of bath-related deaths may be underestimated when determining public health statistics.
This study had several limitations. As mentioned above, the autopsy rate in Korea is extremely low (1.6%),10 and performed only when necessary; this prevented us from determining the mortality rates due to bath-related deaths per 100,000 inhabitants in Korea. However, forensic pathologists produce a high diagnostic yield of histological examinations and perform toxicological screening, including alcohol, in all deaths to ensure a high diagnostic accuracy. Additionally, individuals with bathtub-related injuries would normally be transferred to a hospital, but if they subsequently died, an autopsy was usually not performed. As death certificates were issued by clinicians, there were no data on in-hospital deaths associated with bath-related deaths.
In conclusion, our study revealed that the primary cause of mortality in two-thirds of bath-related deaths was drowning, while the remainder died of natural diseases and acute alcohol intoxication. Although the diagnosis of bathtub drowning is still performed by a process of elimination, our results showed that multiple water inhalation signs as found on complete autopsy can confirm bathtub drowning. Two leading contributory causes of bath-related deaths were cardiovascular disease and alcohol intoxication (binge drinking before bathing). Preventive strategies for reducing bath-related deaths should target alcohol drinking before bathing. Moreover, long soaking times in bathtubs should be avoided, especially among elderly individuals with preexisting cardiovascular diseases. Lastly, the manner and cause of bath-related deaths can have legal consequences; if clinicians do not have sufficient experience in investigating bath-related deaths, they ought to consult forensic pathologists for assistance in determining the manner and cause of death.
 XML Download
XML Download