

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Preterm birth (PTB) is related to increased risk for neonatal morbidity and mortality,12 resulting in a substantial socioeconomic burden.3 Although there is solid evidence about the association between microbial invasion of the amniotic cavity and PTB,45 several other complicated and multifactorial processes are associated with PTB. Genetics, lifestyle factors (such as diet, physical activity, maternal obesity, or maternal age), and psychological factors (such as depression or long-term stress) are such other risk factors.67891011 Among these risk factors, lifestyle factors are of specific concern because they are adjustable risk factors.
Maternal obesity is a major health issue, and pregnant women with obesity are at the increased risk for adverse maternal and perinatal outcomes, such as cesarean section, diabetes, fetal death in utero, and preeclampsia.12 In addition, previous studies have also reported an association of PTB with maternal obesity in singleton gestation,13 and this association was observed in both spontaneous and medically indicated PTB. In women with obesity, the risk of medically indicated PTB was explained by higher risk of obesity-related obstetric complications such as maternal diabetes and preeclampsia. The relationship between spontaneous PTB and obesity allowed us to have newer insights on the pathophysiology of PTB, such as sterile intra-uterine inflammation or alterations in adipokine regulation.
The relationship between PTB and maternal obesity is not as well evaluated in multiple pregnancy as in singleton pregnancy. This is an important issue, because multiple pregnancy itself increases the risk of PTB, compared with singleton pregnancy.1415 In the current study, we evaluated the risk of spontaneous PTB according to the pre-pregnancy body mass index (BMI) in twin gestations.
METHODS
This retrospective cohort study included women pregnant with twins who gave birth in Seoul National University Hospital or Seoul Metropolitan Government-Seoul National University Boramae Medical Center between 2004 and 2014. We reviewed clinical characteristics including age, height, pre-pregnancy weight, parity and previous history of PTB (gestational age of delivery [GAD] < 37 weeks). Data for variables were based on information from electronic medical records. All patients were asked to provide maternal pre-pregnancy body weight information at the time of admission. The study population was divided into three groups according to the maternal pre-pregnancy BMI; underweight (BMI < 18.5), normal (BMI 18.5 to 22.9), overweight/obese (BMI 23 to 24.9/BMI > 25).16 Cases with fetal death in utero or cases without documentation for the pre-pregnancy BMI in the medical records were excluded.
The risk of PTB was compared according to maternal pre-pregnancy BMI. The GAD was defined as the GAD of the first baby. PTB was classified as spontaneous PTB (preterm labor, preterm premature rupture of membranes, or cervical insufficiency) and medically indicated PTB (cesarean section or induction of labor due to maternal/fetal indications). In addition, the pregnancy outcomes such as GAD, birthweight, gestational diabetes mellitus and preeclampsia were also evaluated.
Statistical analysis
The Mann-Whitney U test or Kruskal-Wallis test was used for analysis of statistical associations between continuous variables, and we performed Fisher's exact test or χ2 test for analysis of statistical associations between categorical variables. Binary logistic regression analysis was done to adjust for confounding variables. All statistical analyses were performed using SPSS version 22.0 for Windows (SPSS Inc., Chicago, IL, USA), and P < 0.05 was considered significant.
RESULTS
During the study period, a total of 1,959 women met the inclusion criteria and were included in the analysis. In the study population, the percentages of total PTB and spontaneous PTB (GAD < 34 weeks) were 13.1% and 9.3%, respectively.
The clinical characteristics are summarized in Tables 1 and 2. The frequencies of underweight and overweight/obese women were 14.9% and 18.8%, respectively. Overweight/obese women were older and more likely to develop gestational diabetes mellitus.
Table 1
Clinical characteristics according to the pre-pregnancy BMI
Data shown are mean ± standard deviation or number (%).
BMI = body mass index, IVF-ET = in vitro fertilization-embryo transfer, NS = not significant, PTB = preterm birth.
aP value of comparison between groups 1 and 2; bComparison between groups 2 and 3; cComparison between groups 1 and 3; dComparison among groups 1, 2, and 3.
![]()
Table 2
Pregnancy outcomes according to the pre-pregnancy BMI

Data shown are mean ± standard deviation or number (%).
BMI = body mass index, GAD = gestational age of delivery, NS = not significant.
aP value of comparison between groups 1 and 2; bComparison between groups 2 and 3; cComparison between groups 1 and 3; dComparison among groups 1, 2, and 3.
![]()
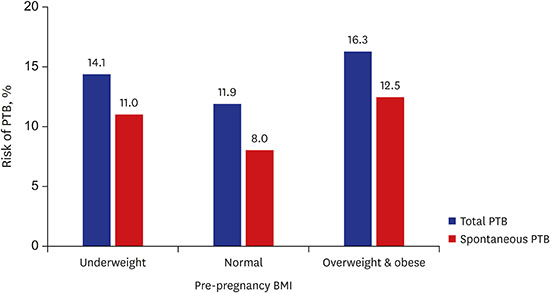
The percentages of total PTB in underweight, normal, overweight/obese women were 14.1%, 11.9%, and 16.3%, respectively (P = 0.076), and that of spontaneous PTB were 11.0%, 8.0%, and 12.5% (P < 0.05), respectively (Fig. 1). The risk of total or spontaneous PTB was significantly different between the women with normal weight and the overweight/obese women (P < 0.05 for both). However, the risk of total or spontaneous PTB between the underweight group and the normal group did not reach statistical significance (P = not significant). In normal weight group, the risk of PTB was lowest among the three groups.
 | Fig. 1Risk of total/spontaneous PTB according to the pre-pregnancy BMI.
PTB = preterm birth, BMI = body mass index.
|
The risk of total PTB was higher in overweight/obese group than in normal weight group, even after adjustment for a history of prior PTB, age, maternal height, parity, in vitro fertilization-embryo transfer (IVF-ET) (odds ratio [OR], 1.43; 95% confidence interval [CI], 1.01–2.03), and the risk of spontaneous PTB was also higher in overweight/obese group than in normal weight group after adjustment (OR, 1.58; 95% CI, 1.05–2.36), as presented in Table 3.
Table 3
Multiple logistic regression analysis for the association between pre-pregnancy BMI and total/spontaneous PTB

BMI = body mass index, PTB = preterm birth, OR = odds ratio, CI = confidence interval, IVF-ET = in vitro fertilization-embryo transfer, NS = not significant.
![]()
DISCUSSION
The principal findings of the current study were that 1) the percentages of total PTB were 14.1%, 11.9%, 16.3% in underweight, normal, and overweight/obese women, respectively, and the percentages of spontaneous PTB were 11.0%, 8.0%, 12.5% in these groups; 2) when compared to normal weight group, the rate of total or spontaneous PTB was significantly higher in overweight/obese group, and this difference remained significant after adjustment for history of prior PTB, age, maternal height, parity, IVF-ET.
In singleton pregnancy, many studies have reported the association between maternal obesity and the risk of total and spontaneous PTB. In Sweden, Cnattingius et al.7 concluded that overweight and obese women at early pregnancy were related to increased risks of preterm delivery, especially extremely preterm delivery. Several other studies have also reported similar findings in singleton pregnancy.171819
The finding that obese women are at higher risk for total PTB in the current study is consistent with the results of previous studies concerning multiple gestation. A study by Suzuki et al.20 indicated that maternal obesity was an independent risk factor for very PTB in dichorionic twin pregnancies. In 2014, a Canadian study reported a significant association between maternal pre-gravid BMI and the risk of very preterm delivery (< 32 weeks) in pregnancies with twins.21 However, we could not find any report which evaluated the risk of spontaneous PTB related to maternal pre-pregnancy BMI in multiple pregnancy.
We asked the question of why obesity is related to the risk of spontaneous PTB in both singleton and multiple pregnancy. The biologically plausible mechanism is that obesity is related to the presence of a mild inflammatory condition. Obesity is a known risk factor for coronary heart disease, and a mild inflammatory condition has been suggested as the possible mechanism of this association.22 Also, the study of Ramsay et al.23 showed that obesity in pregnancy could lead to an elevated inflammatory state. This state results in increased secretion of pro-inflammatory cytokines (e.g., interleukin [IL]-1 and tumor necrosis factor [TNF]-alpha), which may cause contraction of the myometrium and weakening of membranes.24 Another reason could be that insulin resistance associated with obesity might increase the risk of PTB,23 because the level of C-reactive protein or cytokines (IL-1, IL-6, or TNF-alpha) is elevated in adults with insulin resistance.2526 In addition, the risk of genitourinary tract infection, which is one of the risk factors of chorioamnionitis, is increased in obese women,2728 and such infections inducing chorioamnionitis may be affected by up-regulation of the inflammatory process. Lastly, it has been suggested that obesity is a factor in vulnerability to infection.
In contrast to the result with regard to singleton pregnancy, the risk of medically indicated PTB was not increased in overweight/obese women in the current study. The complications unique to multiple pregnancy (e.g., twin-to-twin transfusion syndrome and monoamnionic twin) constituted the causes of medically indicated PTB in part, and the difference in the indication of PTB may be one of the contributing causes of this difference between singleton and multiple pregnancy.
In singleton pregnancy, Shaw et al.29 showed that being underweight (maternal pre-pregnancy BMI < 18.5) was related to modest risks for spontaneous PTB (GAD ≤ 36 weeks), especially GAD ≥ 32 weeks. In the current study, underweight group had a higher risk of total and spontaneous PTB than normal weight group, but this difference did not reach statistical significance.
Table 3 shows that IVF-ET reduces the risk of total PTB (OR, 0.66; 95% CI, 0.48–0.93). There are several reports whether pregnancy conceived with assisted reproductive technique (ART) is related to maternal and fetal outcomes.3031323334 Luke et al.35 studied the effects of fertility status on adverse perinatal outcomes in twin pregnancies and found that the risk of PTB was increased among IVF twins. In contrast, the study by Geisler et al.36 reported that there is no significant difference in the risk of PTB in assisted and naturally conceived twin pregnancies. These results show that there is a disagreement on the relation between PTB and the type of conception in twin pregnancy.
Although this study reported statistically significance about the association of pre-pregnancy BMI with spontaneous PTB in twin pregnancy, it has several limitations. First, we adopted self-reported pre-pregnancy weights to calculate pre-pregnancy BMI as other several studies. Self-reported weights make bias for underestimated pre-pregnancy BMI. In addition, we could not evaluate several factors such as diet or physical activity. But Khatibi et al.17 reported that controlling dietary fiber intake and physical activity during leisure in pregnant women had no influence on the association between pre-pregnancy BMI and PTB. Third, the Institute of Medicine guidelines about gestational weight gain (GWG) has had an important role to guide prenatal care in clinical practice. There are several reports about the relation between GWG and maternal-fetal outcomes. In this study, GWG besides pre-pregnancy BMI also might affect the risk of PTB. To analyze the effect on PTB, the rate of GWG (per weeks in each trimester) because of the difference in GAD is needed. These data in this study are limited and further study is needed.37383940
In clinical practice, overweight/obese women planning to become pregnant could be recommended for preconceptual weight loss. Adequate control or reduction of body weight before pregnancy could help overweight/obese women with twin pregnancies to lower the risk of spontaneous PTB.
In conclusion, the risks of both total and spontaneous PTB were significantly greater in the overweight/obese group than in normal BMI group.
 XML Download
XML Download