

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Multifetal gestations are associated with increased risks of fetal and infant morbidity and mortality, such as an approximately five-fold increased risk of stillbirth and a seven-fold increased risk of neonatal death. These issues are primarily due to complications of prematurity.12345 The increasing number of unexpected stillbirths and neonatal deaths in multiple gestations in high-income countries since 2005 has made it important to evaluate the optimal timing of delivery to achieve positive outcomes in twin pregnancies.67
Due to the significant neonatal morbidities associated with moderate and late preterm births and the risk of perinatal death at approximately 38 weeks of gestation,89 the American College of Obstetricians and Gynecologists (ACOG) Committee suggested recommendations for timing of delivery in women with uncomplicated twin gestations as follows10: 1) women with uncomplicated dichorionic-diamniotic twin gestations can undergo delivery at 38 weeks of gestation; 2) women with uncomplicated monochorionic-diamniotic twin gestations can undergo delivery at between 34 weeks and 37 6/7 weeks of gestation; 3) women with uncomplicated monochorionic-monoamniotic twin gestations can undergo delivery at 32–34 weeks of gestation. There are fewer data for triplet and higher-order multiple gestations despite the fact that the risk of stillbirth increases with plurality. Stillbirth and infant death are two adverse perinatal outcomes that demonstrate substantial disparities according to race/ethnicity, maternal age, pre-pregnancy body mass index, birth weight, and so on.11
According to previous reports and the Korean statistical information service's data (http://kosis.kr), the multiple birth rate, which is the incidence of multiple births per 1,000 live births, increased from 11.3 in 1992 to 13.2 in 1995, 20.0 in 2003, 27.5 in 2008, and finally 36.9 in 2015.12
With the above in mind, this study aimed to investigate the risks of stillbirth and infant death after birth in Korea according to the week of gestation in twin and triplet pregnancies and to quantify the risk associated with expectant management vs. delivery during the late third trimester.
METHODS
De-identified Korean Vital Statistics Birth Certificate, Vital Statistics Death Certificate, and Vital Statistics Fetal Death File data11 from a total of 3,181,145 newborns and 43,385 fetal deaths in utero were obtained from Statistics Korea. Korean Vital Statistics is a nationwide database that was developed to increase the understanding of birth, death, marriage, and divorce, i.e., the basic causes of changes in the size and structure of the Korean population. Data from Korean Vital Statistics are released monthly and annually via a press release, on the web (http://kosis.kr), and in online publications such as the ‘Annual Report on the Vital Statistics.’
Raw data on all live fetuses delivered from 2009 to 2015 (444,849 in 2009, 470,171 in 2010, 471,265 in 2011, 484,550 in 2012, 436,455 in 2013, 435,435 in 2014, and 438,420 in 2015) were analyzed. Our results were based on 92,619 twin and 1,352 triplet births after applying exclusion criteria. Data regarding newborns or stillborns at gestational age (GA) < 32 weeks or > 42 weeks (n = 76,218), singleton pregnancies (n = 3,113,304), quadruplet pregnancies (n = 4), unknown number of fetuses (n = 7,308), and extreme maternal age (< 15 or > 45 years old, n = 12,202) were excluded. Some of the exclusions (n = 78,477) were duplicated. Pregnancy dating was determined using the best obstetric estimate rather than the last menstrual period. However, if the estimated age based on the last menstrual period was significantly different from that estimated by ultrasound, GA determined using ultrasound was used and there was no allowance for GA correction following birth. GA was expressed in intervals in completed weeks. For example, a GA of 40 weeks refers to 40 weeks plus 0–6 days. The body weight was measured to the nearest 10 g. This study used anonymous registry data.
Inclusion and exclusion criteria
The study population comprised all twin and triplet deliveries to women between 32 0/7 and 42 6/7 weeks of gestation. We excluded fetal or infant deaths caused by congenital abnormalities in the death registry.
Outcome measures
Stillbirth was defined as intrauterine fetal death occurring after a GA of 16 weeks and before the start of delivery or that occurring during labor. Infant death was defined as death occurring within the first year of life. The incidence of stillbirth at a given GA was calculated as the number of stillbirths (whether antepartum or intrapartum) at that GA per 10,000 ongoing pregnancies minus half of the births in the given week. This correction factor (subtracting half of the deliveries during the week of investigation from the denominator of total ongoing pregnancies) was described by Smith as a way to correct for the censoring of pregnancies that are delivered during the week assuming that they occurred on average half-way through the week.1314 Infant mortality at each GA was calculated as the number of infants born at that GA who died within 1 year of life per 10,000 live births at that same GA. The mortality risk associated with delivery during a given week was defined as the mortality rate among infants born during that gestational week. The mortality risk associated with 1 week of expectant management was defined as the risk of stillbirth over that week plus the mortality risk experienced by infants born in the subsequent week of gestation. The composite risk associate with 1 week of expectant management represents the sum of the probability of stillbirth during a given week of gestation plus the probability of infant death when birth occurs in the subsequent week. This composite risk of expectant management beyond each given week of gestation was then compared with the risk of infant death for children born in the given week of gestation. The “number needed to deliver” was calculated as an analogous measure as the “number needed to treat” by taking the reciprocal of the absolute difference in risk between delivery and expectant management.
Statistical analysis
Statistical calculations were performed with Excel and SAS version 9.3 (SAS Institute Inc., Cary, NC, USA), including proportions, relative risks, and 95% confidence intervals (CIs). Χ2 tests were performed to compare the proportions of independent variables and a t-test was performed to compare means. Poisson regression analysis was performed to compare the risk of stillbirth, infant death, and expectant management by GA. Statistical significance was reached with a P value of < 0.05 or if the 95% CIs did not overlap. We assumed that the binomial probability distributions of both mortality risks approximated the normal distribution and derived the CI of the composite risk using the sum of the variances plus twice the covariance of the estimates of infant death and stillbirth.
RESULTS
Our analysis included 94,170 multiple deliveries between 32 and 41 weeks of gestation, of which 92,619 (98.4%) were twin and 1,352 (1.44%) were triplet pregnancies. In twin pregnancies, there were 448 stillbirths (0.48% in total twin births between 32 and 41 weeks of gestation) and 196 infant deaths (2.13%) in 92,171 twin live births between 32 and 41 weeks of gestation. In triplet pregnancies, there were 17 stillbirths (1.26% in total triplet births between 32 and 41 weeks of gestation) and three infant deaths (0.22%) in 1,335 twin live births between 32 and 41 weeks of gestation. The maternal and infant baseline characteristics of the study cohort are shown in Table 1.
Table 1
Demographic characteristics of women with multiple gestations between 32 and 41 weeks of gestation in Korea between 2009 and 2015

![]()
Twin pregnancies
In twin pregnancies, the highest risk of stillbirth was seen at 41 weeks with 250 per 10,000 ongoing pregnancies (95% CI, 14.44–1,054.95) (Table 2 and Fig. 1). The risk of stillbirth was significantly increased between 34 and 35 weeks (from 7.02, 95% CI, 5.4–8.93 to 12.3, 95% CI, 10.03–14.88 per 10,000 ongoing pregnancies) and between 37 and 38 weeks (from 12.56, 95% CI, 9.55–16.14 to 31.1, 95% CI, 21.67–42.92 per 10,000 ongoing pregnancies).
Table 2
Risk of stillbirth and infant death associated with expectant management by gestational age

CI = confidence interval.
aComposite risk = risk of stillbirth at this gestational age + risk of infant death at the next gestational age (week).
![]()
 | Fig. 1Stillbirth rate per 10,000 ongoing pregnancies. (A) Twin pregnancies. (B) Triplet pregnancies.
Stillbirth rates show an increasing pattern from 38 weeks onwards in twin pregnancies (A) and 35 weeks onwards in triplet pregnancies (B). The dotted line in (B) is a trend line.
|
The highest risk of infant death was seen at 32 weeks, with 132.36 deaths per 10,000 live births (95% CI, 90.04–186.04) (Table 2 and Fig. 2). The risk of infant death at 33 weeks, with 98.89 deaths per 10,000 live births (95% CI, 68.98–136.32), was significantly higher than the risk at 34 weeks of gestation (41.06 per 10,000 live births, 95% CI, 27.25–58.88). The risk of infant death at 34 weeks, with 41.06 deaths per 10,000 live births (95% CI, 27.25–58.88), was significantly lower than the risk at 33 weeks of gestation (98.89 per 10,000 live births, 95% CI, 68.98–136.32), but significantly higher than the risk at 36 weeks of gestation (12.87 per 10,000 live births, 95% CI, 8.91–17.85). The risk of infant death at 37 weeks was the lowest, with 9.44 deaths per 10,000 live births (95% CI, 6.54–13.10). There was no significant difference in the risk of infant death between 36 and 39 weeks of gestation (P value = 0.20).
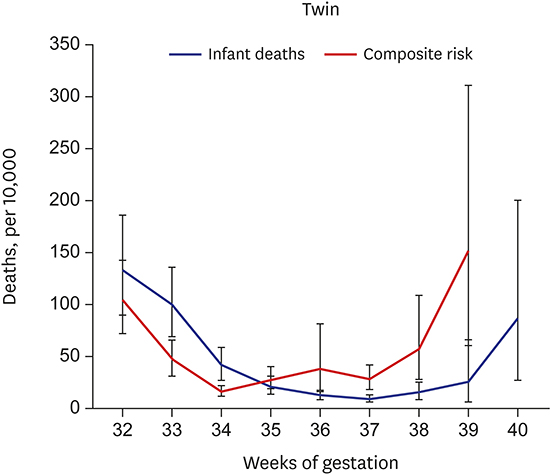
 | Fig. 2Graph comparing the risk associated with delivery (represented by infant death) with the risk associated with expectant management for 1 week (represented by the stillbirth rate plus the infant death risk at the subsequent gestational age) at each gestational age in twin pregnancies.
|
At 37 weeks of gestation, the risk associated with expectant management was significantly higher than that associated with delivery (28.35 compared with 9.44 deaths per 10,000, relative risk 3, 95% CI, 1.41–6.38) (Table 3). The risks diverged substantially at 38 weeks, favoring delivery over expectant management when considering the overall risk for either fetal or infant death (Fig. 2). The absolute difference in risk ranged from 6.83 deaths per 10,000 (95% CI, 5.22–9.29) at 35 weeks of gestation to 125.88 deaths per 10,000 at 39 weeks of gestation (95% CI, 54.29–244.78). From these data, the number needed to deliver ranged from 1,463 (95% CI, 1,077–1,917) at 35 weeks of gestation to 529 (95% CI, 350–839) at 37 weeks of gestation and 79 (95% CI, 41–184) at 39 weeks of gestation (Table 3).
Table 3
Relative and absolute risks associated with expectant management compared with delivery at 32–41 weeks of gestation

![]()
Triplet pregnancies
In triplet pregnancies, the highest risk of stillbirth was seen at 38 weeks, with 1,250 deaths per 10,000 ongoing pregnancies (95% CI, 75.85–4,453.57). The lowest risk of stillbirth was seen at 34 weeks, with 10.78 deaths per 10,000 ongoing pregnancies (95% CI, 0.62–47.36) (Table 2 and Fig. 1). The risk of stillbirth increased significantly between 34 and 37 weeks (from 10.78, 95% CI, 0.62–47.36 to 731.71, 95% CI, 187.16–1,789.03 deaths per 10,000 ongoing pregnancies). Because there were just three infant deaths among 1,335 triplet live births between 32 and 41 weeks, analysis of the risks associated with infant death and expectant management vs. delivery was mostly unfeasible (Table 2). Therefore, the relative and absolute risks of expectant management were not analyzed in this subgroup.
DISCUSSION
In this study, we estimated the risks of stillbirth and infant death after birth in Korea according to the weeks of gestation in twin and triplet pregnancies and quantified the risks associated with expectant management vs. delivery during the late third trimester. The risk of stillbirth significantly increased with increasing GA between 34 and 35 weeks and between 37 and 38 weeks of gestation in twin pregnancies and between 34 and 37 weeks of gestation in triplet pregnancies. This result supports ACOG recommendations based on the significant neonatal morbidities associated with moderate and late preterm births and the risk of perinatal death at approximately 38 weeks of gestation. As expected, the risk of infant death following delivery gradually decreased as pregnancies approached full term. Week-by-week differences in the risk of infant death were statistically significant (both P < 0.05) between 33 and 34 weeks and between 35 and 37 weeks in twin pregnancies. In triplet pregnancies, most of the week-by week changes in the risk of infant death could not be calculated due to the small number of cases. In twin pregnancies, the composite risk of stillbirth and infant death associated with an additional week of pregnancy increased from 37 to 38 weeks of gestation without statistical significance. At 37 weeks of gestation, the relative risk of mortality was significantly higher with expectant management compared to immediate delivery (relative risk, 3.00; 95% CI, 1.41–6.38) in twin pregnancies. Recent studies suggest that delivery should be considered at 37 weeks of gestation in uncomplicated dichorionic twin pregnancies to minimize the risk of perinatal death.151617
With respect to neonatal morbidities in twins, the latest data from Korea show that neonatal composite morbidity is non-significant in births after 35 weeks in monochorionic twins and 36 weeks in dichorionic twins when defined as either one or both twins having one or more of the following: fetal death after 35 weeks of gestation, admission to a neonatal intensive care unit, mechanical ventilator requirement, respiratory distress syndrome, and neonatal death.18 When we consider the three times higher relative risk of death associated with expectant management compared to delivery in this study, delivery at 37 weeks of gestation seems reasonable in uncomplicated twin pregnancies.
The current study has some of the same methodological limitations as previous studies.13141519 A novel limitation was our inability to exclude some complicated pregnancies and to differentiate chronicity and maternal nationality due to limitations in the data. However, the major strength of the current study is that the dataset was large enough to examine stillbirth rates at each GA in twin and triplet pregnancies in Korea. It is almost impossible to estimate these rates at the non-national level. The results of this study suggest that close monitoring regarding fetal death should be performed from 34 weeks of gestation in twin pregnancies. The data and recommendations concerning triplet pregnancies are more limited. In one previous study, the point of intersection of fetal and neonatal death rates in triplet pregnancies occurred at between 35 and 36 weeks. After 36 weeks, the prospective risk of stillbirth exceeded the neonatal death rate.20 On the basis of these data, most experts agree that even if the pregnancy is otherwise uncomplicated, triplet gestations should not extend beyond 36 weeks. The ACOG does not comment on the timing of delivery for triplets. The National Institute for Health and Care Excellence (NICE) guidelines state that women carrying triplets should be offered delivery at 35 weeks and at no later than 36 weeks.21 In this study, we could not draw conclusions regarding the optimal timing of delivery in triplet pregnancies due to the limited sample size. However, the risk of stillbirth showed an increasing tendency after 34 weeks of gestation. Therefore, close fetal surveillance should be a component of antepartum care in triplet pregnancies after 34 weeks of gestation. Finally, it seems reasonable to follow the NICE guidelines concerning the timing of delivery in triplet pregnancies.
Delivery at 37 weeks of gestation can minimize the risks of stillbirth and infant death in uncomplicated twin pregnancies, although individual maternal and fetal characteristics must be considered when determining the optimal timing of delivery in these cases. In both twin and triplet pregnancies, close fetal surveillance should be emphasized in antepartum care after 34 weeks of gestation. Although data are still limited, delivery seems reasonable until 35 weeks in triplet pregnancies in accordance with the NICE guidelines.
 XML Download
XML Download