

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Adenoidectomy with/without tonsillectomy is a commonly performed pediatric otorhinolaryngology surgery. In 2006, 132,000 adenoidectomies without tonsillectomy were performed in children younger than 15 years of age in the United States.1 Our previous study reported that the rate for adenoidectomy with/without tonsillectomy was 0.8 per 1,000 in Korea.2
The adenoids are a mass of lymphoid tissues located in the superoposterior area of the nasopharynx and affect breathing in the upper airway. It is known that, in general, the adenoids are tiny in size at birth and consistently grow during several years after birth due to the hyperactivity of the immune system.3 The adenoids are known to cause either mechanical obstruction or stasis of secretions or may be a nidus causing repeated episodes of upper respiratory infection.4 Additionally, the adenoid can serve as a reservoir of pathogenic bacteria and recurrent or persistent adenoiditis is associated with common diseases of neighboring structures including sinusitis.5 In many children, adenoid hypertrophy and sinusitis are known to coexist. The association between the two conditions is variable, with some authors finding that an association exists678 and others showing that there is no such association.910
Indications for adenoidectomy are controversial. Widest agreement surrounds their removal for obstructive sleep apnea, usually combined with tonsillectomy.11 There is also support for adenoidectomy in recurrent otitis media in children previously treated with tympanostomy tubes.12 However, at present the effectiveness of adenoidectomy in children with recurrent or chronic nasal symptoms remains uncertain and practice is experience-based rather than evidence-based. Some surgeons prefer to perform adenoidectomy in these children,81314 whereas others do not.151617
The purpose of this study is to compare post-operative (post-op) visits for sinusitis between the adenoidectomy and non-adenoidectomy participants (control) using the national cohort study. In this study, we matched the adenoidectomy and control group as 1:4 for age, sex, income group, and the number of pre-operative sinusitis histories. We followed the participants at least 1 year, at maximum 9 years.
Go to : 
METHODS
Study population and data collection
This national cohort study relied on data from the Korean Health Insurance Review and Assessment Service-National Patient Sample (HIRA-NPS). The Korean National Health Insurance Service (NHIS) selected samples directly from the entire population database to prevent non-sampling errors. Approximately 2% of the samples (one million) were selected from the entire Korean population (50 million). This selected data could be classified into 1,476 levels (age [18 categories], sex [2 categories], and income level [41 categories]) using randomized stratified systematic sampling methods by proportional allocation to represent the entire population. After data selection, the appropriateness of the sample was verified by a statistician who compared data from the entire Korean population with the sample data. The detailed methods of these procedures were described by the National Health Insurance Sharing Service.18 This cohort database included 1) personal information, 2) health insurance claim codes (procedures and prescriptions), 3) diagnostic codes using the International Classification of Disease-10 (ICD-10), 4) socio-economic data (residence and income), and 5) medical examination data for each participant for a period ranging from 2002 to 2013.
As all Korean citizens have a 13-digit resident registration number from birth to death, exact population statistics can be determined from the database. It is mandatory for all Koreans to enroll in the NHIS. All Korean hospitals and clinics use the 13-digit resident registration number to register individual patients for the medical insurance system. Therefore, the risk of overlapping medical records is minimal, even if a patient moves from one place to another. Moreover, all medical treatments in Korea can be tracked using the HIRA system without exception.
Participants selection
From 1,025,340 cases with 114,369,638 medical claim codes, participants who received adenoidectomy (claim codes: Q2800) with/without tonsillectomy from 2004 through 2012 were included (n = 2,735). Among them, the participants who received sinus surgery such as antrostomy, endoscopic sinus surgery, or Caldwell-Luc operation were excluded (n = 12). They were 1:4 matched with the participants (control group) who never received adenoidectomy from 2002 through 2013 in this cohort. Matching was processed for age group, sex, income group, region of residence, and the number of pre-operative sinusitis histories for 2 years. To prevent selection bias when selecting the matched participants, control group participants were sorted by random number order, and they were selected from top to bottom. Adenoidectomy participants who did not have enough matching participants were excluded (n = 130). Finally, we used 1:4 matching to select 2,593 adenoidectomy participants (adenoidectomy without tonsillectomy = 332 [12.6%], adenoidectomy with tonsillectomy = 2,309 [87.4%]) and 10,372 control participants (Fig. 1).
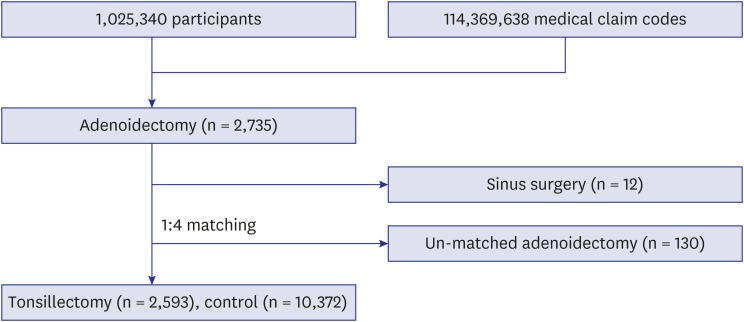 | Fig. 1Schematic illustration of participant selection for the present study. Of a total of 1,025,340 participants, 2,735 adenoidectomy participants were selected. Participants who underwent sinus surgery were excluded (n = 12). The adenoidectomy participants were matched 1:4 with controls who did not undergo adenoidectomy. Un-matched adenoidectomy participants were excluded (n = 130). Finally, 2,593 adenoidectomy participants and 10,372 control participants were included.
|
Variables
The age groups were classified into 5-year intervals: 0–4, 5–9, 10–14, …, and 80+ years old. Consequently, 17 age groups were designated (Age group of 0 and 1–4 were merged). The income groups were initially divided into 41 classes (one health aid class, 20 self-employment health insurance classes, and 20 employment health insurance classes). These groups were re-categorized into 11 classes (class 1 [lowest income]–11 [highest income]). Regions of residence were divided into 16 areas according to administrative district. It was regrouped as urban (Seoul, Busan, Daegu, Incheon, Gwangju, Daejeon, and Ulsan) and rural area (Gyeonggi-do, Gangwon-do, Chungcheongbuk-do, Chungcheongnam-do, Jeollabuk-do, Jeollanam-do, Gyeongsangbuk-do, Gyeongsangnam-do, and Jeju-do).
We defined sinusitis using the ICD-10 codes: J01 (acute sinusitis) and J32 (chronic sinusitis). The number of visits to clinics or hospitals for sinusitis was counted every year. Pre-operative sinusitis was counted for 2 years. Post-op sinusitis was counted each year (1, 2, 3, …, 9 years), and post-op sinusitis for total periods were calculated (Fig. 2).
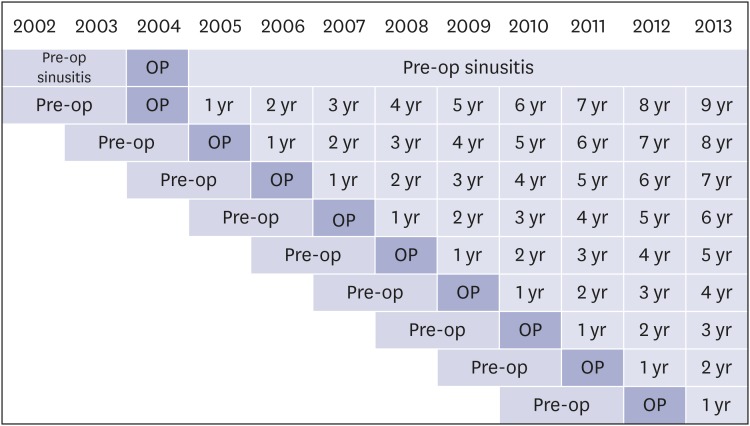 | Fig. 2Schematic illustration of numbers of pre-operative and post-operative sinusitis visits. The number of visits for sinusitis were recorded for 2 years before adenoidectomy. Postoperative visits for sinusitis were counted for 1–9 years according to when the patient underwent surgery.
Pre-op = pre-operative, OP = operative.
|
Statistical analyses
An equivalence test was used to compare the number of sinusitis visits (pre-operative, post-op 1, 2, 3, ..., 9 years) between the adenoidectomy group and control group. The null hypothesis is that post-op sinusitis between the adenoidectomy and control group is not the same. Margin of equivalence of difference (adenoidectomy − control group) was set as −0.5 to 0.5.
For the subgroup analysis according to frequency of sinusitis, the participants were divided into 2 groups: rare pre-operative sinusitis (< 3 times for 2 years) and frequent pre-operative sinusitis (≥ 3 times for 2 years). For the subgroup analysis according to age, the participants were divided into 3 groups: 0–4, 5–9, and 10–14 years old.
For the equivalence test, 95% confidence interval (CI) of difference < 0.5 was considered to indicate statistical significance. The results were statistically analyzed using SPSS v. 21.0 (IBM, Armonk, NY, USA).
Ethics statement
The Institutional Review Board of the Hallym University (2014-I148) approved the use of these data. Written informed consent was exempted by the Institutional Review Board.
Go to :
RESULTS
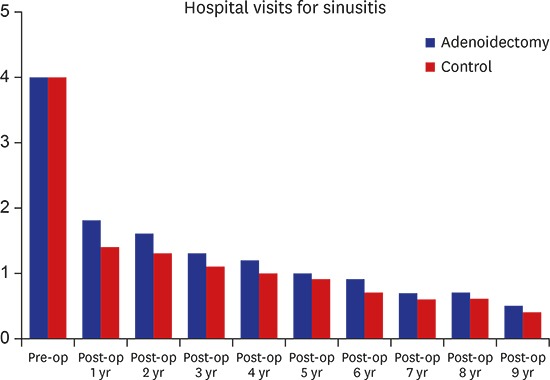
Because of matching, the general characteristics (age group, sex, income level, and region of residence) were equivalent in both groups (Table 1). We compared the visits for sinusitis during the follow up periods. The number of visits for pre-operative sinusitis was also exactly the same in both groups. There were trivial differences between the adenoidectomy and control group from post-op 1 to 2 years (0.3 < 95% CI of difference in post-op 1 year < 0.6; 0.2 < 95% CI of difference in post-op 2 years < 0.5). Visits for sinusitis were larger in the adenoidectomy group than control group from post-op 1 to 2 years. However, there were no differences between the adenoidectomy and control group from post-op 3 through 9 years (−0.5 < all of 95% CI of difference < 0.5). We could find that sinusitis visits gradually decreased from 4.0/2 year (pre-operative), 1.8/year (post-op 1 year), 1.6/year (post-op 2 years), 1.3/year (post-op 3 years), 1.2/year (post-op 4 years), 1.0/year (post-op 5 years), 0.9/year (post-op 6 years), 0.7/year (post-op 7 years), 0.7/year (post-op 8 years), and 0.5/year (post-op 9 years) in the adenoidectomy group. These changes were also found in the control group as the same scale (Table 2).
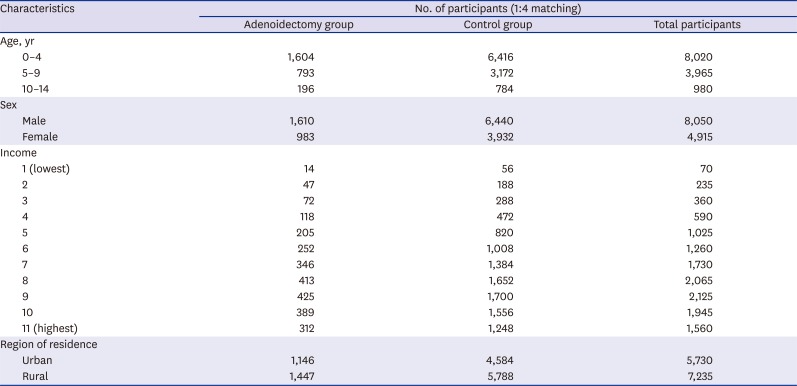
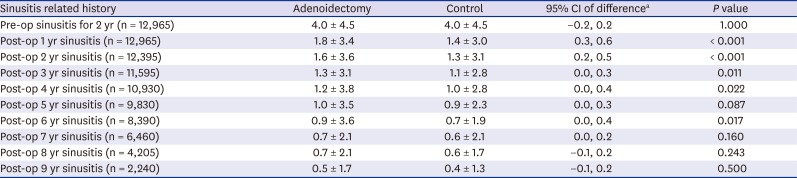
Table 1
General characteristics of participants
![]()
Table 2
Difference of mean values of pre-operative and post-operative sinusitis between adenoidectomy and control group
Data are shown as mean ± standard deviation.
Pre-op = pre-operative, Post-op = post-operative, CI = confidence interval.
aDifference = adenoidectomy − control group.
![]()
In the rare pre-operative sinusitis group (< 3 times for 2 years), there were minor differences between the adenoidectomy and control group from post-op 1 to 2 years (0.4 < 95% CI of difference in post-op 1 year < 0.7; 0.2 < 95% CI of difference in post-op 2 years < 0.5). Additionally, there were insignificant differences between the adenoidectomy and control group from post-op 1 to 2 years in the frequent pre-operative sinusitis group (0.1 < 95% CI of difference in post-op 1 year < 0.6; 0.0 < 95% CI of difference in post-op 2 years < 0.5). Visits for sinusitis were larger in the adenoidectomy group than the control group from post-op 1 to 2 years in both the rare and frequent pre-operative sinusitis group. However, no difference of visit for sinusitis were found between the adenoidectomy and control group (−0.5 < all of 95% CI of difference < 0.5) during follow up periods from post-op 3 through post-op 9 years (Table 3).
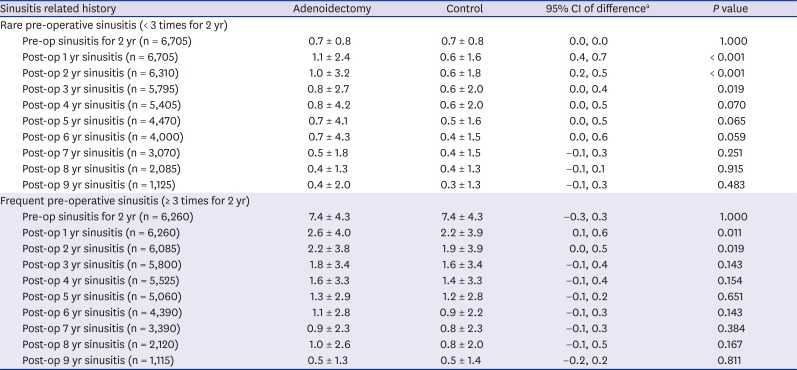
Table 3
Subgroup analysis of mean values of pre-operative and post-operative sinusitis between adenoidectomy and control group (Rare vs. frequent pre-operative sinusitis)
Data are shown as mean ± standard deviation.
Pre-op = pre-operative, Post-op = post-operative, CI = confidence interval.
aDifference = adenoidectomy − control group.
![]()
In the 0–4 years old group, there were minor differences between the adenoidectomy and control group from post-op 1 to 2 years (−0.8 < 95% CI of difference in post-op 1 year < −0.4; −0.6 < 95% CI of difference in post-op 2 years < −0.2). However, no difference in the number of visits for sinusitis were found between the adenoidectomy and control group (−0.5 < all of 95% CI of difference < 0.5) during follow up periods from post-op 3 through 9 years. Additionally, there were no differences between the adenoidectomy and control group during the whole follow up period from post-op 1 through post-op 9 years (Table 4).
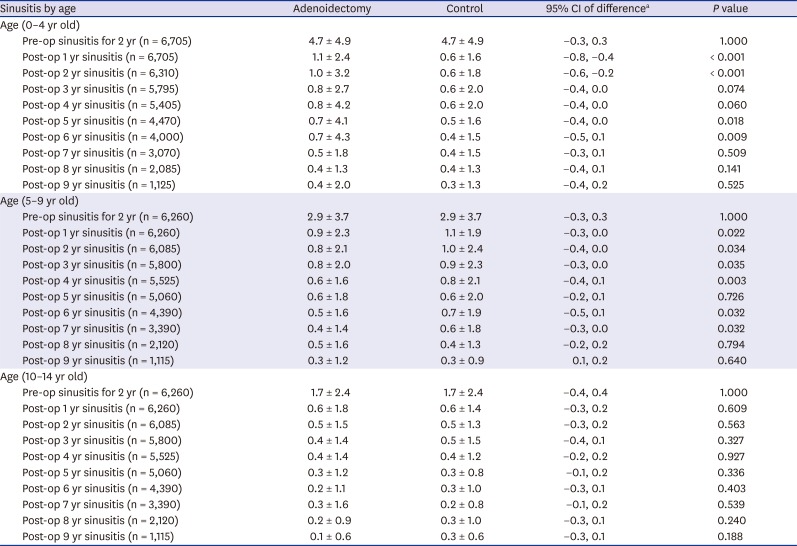
Table 4
Subgroup analysis of mean values of pre-operative and post-operative sinusitis between adenoidectomy and control group according to age group
Data are shown as mean ± standard deviation.
Pre-op = pre-operative, Post-op = post-operative, CI = confidence interval.
aDifference = adenoidectomy − control group.
![]()
Go to :
DISCUSSION
We could not find a definite difference of sinusitis visits between the adenoidectomy and control groups from post-op 3 through 9 years. Although visits for sinusitis were larger in the adenoidectomy group than the control group from post-op 1 to 2 years, they were not very significantly deviated in the equivalence test. After adenoidectomy, the sinusitis visits gradually decreased during follow up periods. However, this was also found in the control group on the same scale.
The latest Cochrane library review reviewed 2 randomized controlled trials (RCTs) for children.10 One study showed that improvement in frequency of nasal obstruction, meaning a change from frequent to infrequent, was found in 61% vs. 41% after 12 months, and in 63% vs. 55% after 24 months in the adenoidectomy and control groups, respectively. The risk difference was non-significant, being 20% (95% CI, −2%, 43%) and 8% (95% CI, −15%, 32%).17 The other study found that at 6 months the mean number of days with nasal discharge in children who underwent adenoidectomy was 26 as compared to 23 days in the control group. The difference was non-significant, being −4 days (95% CI, −13, 7 days).16 These studies' designs were randomized, double blind, and controlled trials. The level of evidence is higher than any other study design. In fact, the designs of studies to support the effectiveness of adenoidectomy for sinusitis were retrospective chart review8 or prospective study without control.131418
Adenoid tissue was historically regarded as a source for bacteria.814 Additionally, the effect of adenoid for sinusitis may be secondary to mechanical obstruction of the nasopharynx.4 Therefore, some authors suggested that adenoidectomy should be performed to remove mechanical obstruction of the nasopharynx or infection focus in chronic or recurrent sinusitis patients.131419 However, they had some limitations due to small participant size,1319 significant follow up loss,19 and lack of investigation about subjective sinusitis symptoms.8 Additionally, Tuncer et al.20 compared maxillary sinus aspirate cultures with adenoid tissue cultures in pediatric subjects with both chronic sinusitis and adenoid hypertrophy. There was a difference of isolated bacteria between adenoid and sinus. The most frequently isolated bacteria in the adenoid culture were Staphylococcus aureus and Streptococcus pneumoniae. The most frequently isolated bacteria in the sinus aspirate culture were α-hemolytic Streptococcus, Neisseria, and β-hemolytic Streptococcus. Thus, they concluded that adenoids did not act as a reservoir of bacteria.20 Furthermore, Berçin et al.9 demonstrated that adenoid volume is not correlated with the extent of sinusitis on paranasal sinus computed tomography scan in the pediatric patients with sinusitis.
One advantage of this study is the large number of study participants (n = 12,965). We followed the adenoidectomy group for a maximum of 9 years, while other studies were conducted for a maximum of 2 years.1317 To our knowledge, this is the largest study which evaluated the efficacy of adenoidectomy for sinusitis. Another advantage is the availability of the comprehensive medical records of each participant. Previous studies asked the participants their histories of recurrent nasal symptoms, which could produce recall bias.1719 In this study, we used their medical record for sinusitis visits using HIRA data. These recorded data were not distorted by their memories. This HIRA data include the entire nation without exception. Therefore, we did not miss any participants during follow up periods, while significant loss of follow up were problems of other studies.13171921 Even though we did not use RCT methods, we matched our participants exactly with a control group according to age, sex, income, region of residence, and previous operative sinusitis visit. Income and region matching were important in that they could be determinant factors for access to medical treatment. Income levels were determined very accurately using the Korean NHIS, given that the patient's premium is determined based on income. Our study results were representative of the entire Korean population, as the data were selected from a database covering the entire population and were verified by a statistician for representativeness. Therefore, we think that removing the adenoid is not the effective treatment in patients who present with symptoms of sinusitis. Additionally, as the children grow, the immune system comes to maturity and adenoid tissue size decrease.
Our study had several limitations. We used health insurance claim data and counted the numbers of visit for sinusitis. It did not exactly mean the number of infections. Many Korean doctors choose the ICD code for insurance coverage of their treatment under the performance-based payment system. The ICD code for sinusitis may be used for common cold patients. However, we think that the number of visits for sinusitis could be a surrogate index of the number of infections within the context of these big data. We could not measure the severity of sinusitis in each participant. The medical use of each participant could be variable in the same disease. We included the participants who received adenoidectomy with tonsillectomy for chronic tonsillar hypertrophy, in that we could not evaluate the purpose of adenoidectomy in each participant. However, if adenoidectomy could reduce sinusitis, the sinusitis of the participants who received adenoidectomy with tonsillectomy for chronic tonsillar hypertrophy also should be decreased.
In conclusion, adenoidectomy does not have a benefit for sinusitis. Sinusitis decreased over time regardless of adenoidectomy.
Go to :
 XML Download
XML Download