

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The major cause of death and disability in children is injury in both developing and developed countries worldwide.1 According to the Centers for Disease Control and Prevention (CDC) Childhood Injury Report, on average, 12,175 children 0 to 19 years of age died each year in the United States from an unintentional injury.2 An estimated 9.2 million children annually had an initial emergency department (ED) visit for an unintentional injury.2 Also, over 40% of children aged under 12 years were found to have some form of disability due to unintentional injury from the Global Childhood Unintentional Injury Surveillance conducted in four cities.3 The most common cause of death in adolescence in Korea was also injury.4 Pediatric patients who visited the ED due to unintentional injury were 6,097 and the rate of critical injury was 59.8 per 100,000 population under aged 20 years.5
Schools have been regarded as relatively safe places from injury. Contrary to this belief, a significant number of injuries occur in schools. Previous studies reported that school injuries accounted for 26%–35% of all injuries in children.67 As school-aged children spend a considerable amount of time in school, school areas should be considered a more likely place than home for the occurrence of injury.8 School injury is an important target for injury prevention programs. Evaluation of the epidemiologic characteristics of injuries that occur in the school is the first step in establishing a strategy for school injury prevention programs.
Previous studies on school injury have used survey data from students or retrospective review of medical records. These data were limited in that detailed information about injury circumstances such as the time of injury could not be obtained.910 The present study used data from the emergency medical services (EMS). In Korea, EMS data are collected nationwide and systematically managed and offer relatively detailed information about injuries.
This study compared the demographic and injury characteristics of school-aged children transported by the EMS for injuries that occurred at school with those of same-aged children who were injured outside of school.
METHODS
Study design and setting
This retrospective cohort study used data from the EMS database from January 1, 2012 through December 31, 2014. This population-based database is nation-wide in Korea. The EMS databases is governed by each of 17 provincial EMS headquarters and shares the same structure.11 The data variables included patient demographic characteristics; clinical information; emergency care provided at the scene and during transportation; and time variables such as call, departure to scene, arrival at scene, etc. This database also included injury information, including the place and mechanisms of injury.12
Study subjects
We included data from injured children who were transported by EMS and were 6 to 17 years of age. Injury was defined as resulting physical harm, either intentional or unintentional, as coded by EMS providers at the scene. Cases with missing information regarding the place of injury were excluded.
Variables and statistical analysis
The place of injury was categorized as “school setting” when documented as “school,” whereas injuries that occurred in any location other than school were coded as “non-school.” Age was categorized into four groups with 3-year intervals: 6 to 8, 9 to 11, 12 to 14, and 15 to 17 years, which approximate the low-grade primary, high-grade primary, middle, and high school-age groups, respectively, according to the academic system in Korea.
The demographic findings and epidemiologic characteristics based on school and outside of school were described. The call day and time for EMS were defined as the occurrence day and time of injury. We investigated temporal variability in the time of day and season in the incidence of school injury.
Continuous data are reported as means and standard deviation or medians and interquartile range; categorical variables are reported as counts and percentages. Two-sided tests were conducted, and P < 0.05 was considered statistically significant. Gender-stratified multivariable logistic regression analysis was conducted to estimate the risks of school injury in each age group and adjusted odds ratios (aORs) and 95% confidence intervals (CIs) were calculated after adjusting for potential risk factors such as sex, season, time of day of injury occurrence, and urbanization level.
RESULTS
We analyzed a total 167,104 cases of child injuries transported by the EMS between 2012 and 2014 in Korea (Table 1). Of these injuries, 13% (22,285 patients) of injuries occurred while in school. The injury mechanisms differed between those that occurred inside and outside school. The most common injury mechanism was road accidents (48%) among school injuries that occurred outside of school, but the most common injury mechanism was fall (44%) among those that occurred in school.
Table 1
Demographics of injury occurred inside or outside the school and transported via EMS

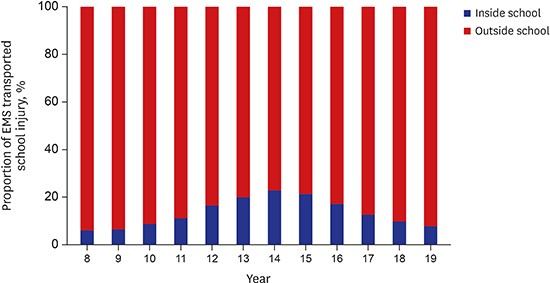
High school grade children were most often injured (70,743, 42%) outside school. Among school injuries, middle school grade children were most often injured (8,828, 39.6%) (Table 1). The proportion of school injuries increased until 12 years and then gradually decreased (Fig. 1). The proportion of fall injuries was highest in the low-grade primary school grade group. As the age increased, the proportion of fall injury gradually decreased (Table 2).
Table 2
Baseline characteristics of school injury grouped by level of school

Both inside and outside of school, the proportions of injured boys were higher compared to those of girls. In girls, the proportion of school injuries were highest in high school-aged children (36.9%). In boys, the proportion was highest in middle school-aged children (40.7%).
In multivariate analysis, the odds of school injury were 1.35 times greater in boys than in girls. The results of gender-stratified multivariate regression are shown in Table 3. When reference group was set to the high school-aged group, only middle school-aged girls had higher odds ratios (ORs). In boys, higher ORs were observed in not only middle school but also high-grade primary school-aged children compared to high school-aged children (Table 3).
Table 3
Multivariate logistic regression models for association between sex and school injury, sex stratified models for association between age group and school injury

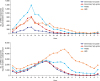
As shown in Fig. 2, the peak time for the occurrence of school injuries was lunch time (13:00–13:59) in all four age groups. However, the peak times for non-school injuries differed by age group. In primary and middle school-aged children, the peak time for non-school injury was around 5 p.m. In high school-aged children, the peak time for non-school injury was around 10 p.m.
DISCUSSION
The epidemiologic characteristics of school injuries differed from those of non-school injuries. Among school injuries, the risk of injury varied according to age group and gender. These epidemiologic findings provide insight to establish priorities and develop strategies for the prevention of school injuries.
We used the EMS database to evaluate the epidemiologic characteristics of school injuries. The EMS data in this study were systematically collected using a standardized, structured nationwide registry. Therefore, there was no recall bias, which is a concern when using surveys of injury experiences. Recently, the EMS database has been used for injury surveillance, including monitoring for injuries such as poisoning and drug overdose,13 mass casualty incidents,14 and severe trauma15 and for risk analysis such as regional variations or injury patterns in young adults engaged in alcohol use.16 This study provides a novel use for the EMS database for the surveillance of injuries occurring in a specific location, such as school.
The findings regarding the injury mechanism of school injury in this study were consistent with those of previous studies.171819 We also identified falls as the most common mechanism of school injury. Previous studies reported falls to be the most common mechanism of injury that required hospitalization and visit to the ED.2021 There was a report that slippery floors accounted for about one-third of school injuries. Environmental factors such as old facilities in disrepair, disorderedly stacked items, slippery or hard floors, and poor supervision of teachers are among the known risk factors for injury. To prevent injury in school and reduce serious damage, it is necessary to replace the floor of playgrounds or under hanging equipment with a soft material or to fix slippery staircases or corridors.22
In this study, 19.6% of the injuries occurring in school were classified as “other mechanism of injury.” We re-categorized mechanisms of injury in the EMS database according to International Classification of External Cause of Injury (ICECI) standards.23 However, there were items that did not match the classification criteria of ICECI because the injury mechanisms in the EMS database were classified according to the scope of the specific objectives of EMS prehospital care and transportation. For example, items such as ‘simple drunken person’ or ‘victim of violence’ in the EMS database did not re-categorize to mechanisms of injury according to ICECI. We categorized these items as ‘other mechanism of injury.’ Among injury mechanisms that were matched ICECI, proportions of thermal injury (1.0%) and poisoning (0.2%) were small. These injury mechanisms included in the ‘other mechanism of injury’ category. The items recorded as ‘other mechanism’ in EMS database were reviewed individually and reclassified according to ICECI.
As several previous studies have also reported, there is a need to pay more attention to middle school injury.24252627 During the middle school years, students' activity levels increase as the body grows rapidly, and the impulsive nature of adolescents contribute to the increased occurrence of injuries in this age group.26 A previous study reported that 50% of school injuries classified as violent occurred in children 10 to 14 years of age.28 Unfortunately, there was no information for intent of injury in the 119 EMS database. In this study, high-grade primary school boys were also at risk for school injury. Depending on the age of puberty, faster, earlier interventions may be necessary to prevent injuries.
Boys were injured more often in this study. According to a previous study, the proportion of serious injuries requiring hospital admission was higher in boys.17 This may be because boys have more dangerous behaviors that are likely to cause injury, such as hanging or climbing high.2930 In this study, the age groups at risk for school injury differed by gender. When developing an injury prevention strategy, age group and gender should be considered.
In a previous study of approximately 15,000 children 0–16 years, the peak rate of injury occurred at approximately 17:00 and a noticeable shoulder in the temporal pattern was observed around noon among all injuries. The peak times among 5–15 years old children clustered between 15:56 and 16:24.31 Another study of 70,000 pediatric trauma cases showed a circadian acrophase at 14:30, with no case recorded between midnight and 04:00.32 The authors suggested that physical activities at school should be planned for the morning rather than in the afternoon. In the present study, the peak incidence was lunch time for all age groups. Several explanations are possible. In Korea, boys may try to compensate for insufficient physical activity in class to play soccer at lunch time. There was also loose teacher supervision during lunch time.
The present study had some limitations. First, the characteristics of patients transported by the EMS differed from those of non-EMS patients. Generally, people with low socioeconomic status and those with more severe injuries tend to use the EMS.33 This difference should be considered when interpreting the results of this study. Second, there was no information on the injury outcomes such as severity of injury or disposition. The linkage of EMS data and hospital records was a challenging issue.
In conclusion, a significant proportion of injuries to school-aged children occur at school and notable differences exist between the epidemiology of in- and out-of-school injuries. These epidemiologic findings provide an insight to establish priority and develop strategies for prevention of the school injury.
 XML Download
XML Download