

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Plasmodium vivax malaria, which is called ‘Hakjil’ in Korea, has been prevalent in Korea for many centuries. Outbreaks, the severity of which have fluctuated over the years, greatly increased during the Korean War (1950–1953), and 15% of the febrile diseases that occurred in the Korean military at that time were malaria.1 After the end of the Korean War, the incidence of malaria rapidly decreased due to improved living standards, an improved healthcare system, implementation of an anti-malaria program, and the spread of pesticides. In 1979, the World Health Organization officially declared that malaria had been eliminated in Korea. However, since then, the incidence of P. vivax malaria has rapidly increased due to its reemergence in 1993 among soldiers near the demilitarized zone (DMZ). To prevent continuous spread within the military and subsequent transmission to civilians, mass chemoprophylaxis was conducted on up to 16,000 soldiers in 1997 and was expanded to 200,000 soldiers in 2005.2 Chemoprophylaxis effectively reduces the morbidity and mortality of malaria during times of high incidence, and is more useful in isolated areas where the risk of malaria infestation is low or during seasonal epidemics.3 It is thought that the mass chemoprophylaxis used in the Korean military actually contributed to the decreased occurrence of malaria in military personnel. However, because resistance can be induced by poor compliance and the exposure risk for soldiers working in malaria risk areas is not high, malaria control systems need to be reestablished in the military.4
As malaria control programs develop, the subjects of interventions are being narrowed down from the whole population to populations in areas at risk for malaria and finally, to individual malaria cases. Although mass chemoprophylaxis was effective in treating malaria during it reemergence, it is necessary to narrow the scope of applicable subjects at this time when the incidence of malaria is markedly reduced. P. vivax malaria has the characteristic of potential transmission before treatment initiation because gametocytes appear in the human body in the early stages of infection.5 Accurate and rapid diagnosis during the early stages after symptom onset is required to eradicate malaria.6 A rapid diagnostic test (RDT), which is an immune-chromatography test that measures P. vivax antigens in human blood, facilitates rapid diagnosis without skilled personnel due to simple reading. RDTs can also be useful for detecting malaria in patients with fever in healthcare facilities that are not equipped with microscopy such as the military. However, the efficacy, safety, and cost of RDTs should be investigated to assess their potential as a substitute for chemoprophylaxis.
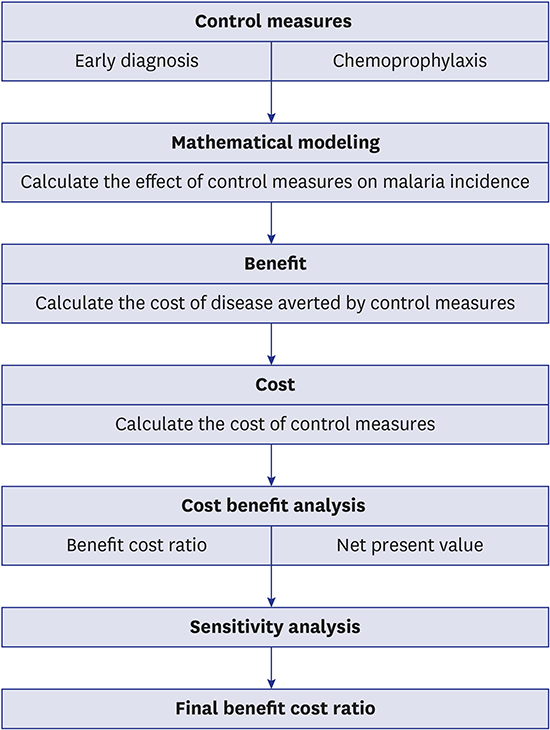
In this study, we developed a mathematical model based on the characteristics of P. vivax malaria, and calculated the expected number of malaria cases when the effects of current mass chemoprophylaxis and alternatives were applied to the model. In addition, cost-benefit analyses were conducted by estimating the cost of each alternative and malaria treatment (Fig. 1). Based on this analysis, we estimated the costs and benefits from a sociological perspective and used the results as evidence for reestablishing a malaria prevention system in military units and implementing national malaria control projects.

METHODS
Study design
Population
The number of people susceptible to malaria infection was defined as the number of military soldiers stationed in malaria risk areas (323,948 soldiers in 2010, 301,835 soldiers in 2011, and 214,623 soldiers in 2012). The rates of moving into and leaving the malaria risk areas were determined by calculating the mean weekly manpower replacement rate (1.1% per week) based on a military service period of 21 months. The density of vector mosquitoes in areas, which the Korea Centers for Disease Control and Prevention (KCDC) has been monitoring, was used to substitute the number of vector mosquitoes. The number of vector mosquitoes contacted by one person was calculated as the daily mean density of vector mosquitoes × the number of workers in the risk area × (31 weeks × 7). The sporozoite infection rate of mosquitoes was assumed to be 0.7%. Mathematical modeling was implemented using the number and duration of malaria cases for the 840,406 soldiers who worked in the malaria risk areas, which was designated by the military between 2010 and 2012 to estimate the number of people in a group.
Perspective
Cost items were determined depending on which perspective of the analysis was adopted. Because the societal perspective was selected in this study, not only medical and non-medical costs but also productivity loss costs associated with morbidity and the cost of premature death due to disease were included in the total costs.
Strategies
The effects of three malaria control strategies were evaluated. As the current malaria chemoprophylaxis (Intervention 1 [μ1]), chloroquine was administered once a week from May to September, and primaquine was administered for 2 weeks starting October 1. For the shortened malaria chemoprophylaxis (Intervention 2 [μ2]), only primaquine was administered for 2 weeks from October 1 without chloroquine. The early diagnosis of malaria (Intervention 3 [μ3]) was conducted using RDT for patients with fever, without the implementation of chemoprophylaxis.
Modelling
In this study, malaria transmission was assumed to only occur through contact between mosquitoes and humans, and a deterministic compartmental model was used. All of the soldiers working in malaria risk areas were classified into four categories: susceptible, exposed, infectious, and treated. The variation within each group was described using simultaneous differential equations, and the number of patients according to each malaria control strategy was calculated. When a susceptible human (susceptible host [Sh]) is bitten by an infectious mosquito (infectious vector [Iv]), sporozoites, which are an infectious form that affects humans, are introduced into the blood at a probability of 1. They first enter the liver, leading to the development of a latent period (exposed host [E1h]). A total of 64% of sporozoites migrating to hepatocytes have a short latency period (E1sh) and 36% have a long latency period (E1lh).7 After undergoing short and long latency periods in the liver, sporozoites enter the erythrocytic stages (E2h), and gametocytes appear up to 5 days after the erythrocytic stages. Because gametocytes enter the mosquito body when a mosquito feeds on blood and undergo the sporogonic cycle, the human becomes infectious (infectious host [Ih]) up to 5 days after the erythrocytic stages.8 If the human is diagnosed and treated during the erythrocytic stage at a probability of 7, it corresponds to early diagnosis and treatment. If the Ih is diagnosed and treated at a probability of 8, it corresponds to late diagnosis and treatment. Treatment failure is indicated by a probability of 9, and treated host (Th) is progression towards E1h+E2h for primaquine resistance and towards E2h for chloroquine resistance (Fig. 2). The time-dependent variation in each group was represented by a simultaneous differential equation (Fig. 3).
 | Fig. 2Diagram of Plasmodium vivax transmission.
Sh = susceptible host, E1h = exposed host, E1sh = exposed host — short latent period in hepatic cycle, E1lh = exposed host — long latent period in hepatic cycle, E2h = exposed host — erythrocytic cycle, Ih = infectious host, Th = treated or recovered host, Sv = susceptible vector, Ev = exposed vector, Iv = infectious vector.
|
 | Fig. 3A mathematical model for Plasmodium vivax using a system of nonlinear ordinary differential equations.
|
We develop a mathematical model for P. vivax malaria using a standard compartmental approach.910 Transmission rates between humans and vector are defined as;

The basic reproduction number is computed using the next generation matrix method given in.11

Parameter estimation
Treatment success rates (τ) indicate that a patient is maintained as a Sh without relapse and reinfection after treatment. Because the rate of relapse (ρ) and rate of reinfection (f) is 3%–5% based on the Epidemiological Investigation of Infectious Disease in Korea reported annually by the KCDC, the τ value was estimated at 0.96. Natural recovery rates (ν), which are represented by the duration required for the natural treatment of infected patients, are from 2.5 to 3 years. The ρ and f were both estimated at 1%. The values of γ1 and γ2, which are the reciprocal of the infection duration of people treated at the E2 and Ih stages, were calculated with the assumption that the patient will recover 3 days after treatment. The progression from E2 to Ih is associated with the time required for gametocyte development after the onset of fever; it is 5–6 days for P. vivax.8 This study assumed that it takes 5 days. The number of vectors estimated for 3 years from 2010 was used to describe a consecutive graph, and the number, birth rate, and death rate of vectors were estimated by calculating the solution of simultaneous differential equations using the least squares method. Based on these values, the fitted plot for soldiers and veterans between 2010 and 2012 was created, and the cumulative number of people infected with malaria depending on each malaria control strategy was calculated.
Benefit data sources
The major benefit of malaria control strategies is the reduction in the costs of malaria control and treatment due to a decrease in the number of patients. In Korea, deaths due to P. vivax are extremely rare, so the benefit due to a reduction in deaths was not considered in this study. The benefit of a reduction in malaria patients was calculated by separating outpatient and inpatient treatments. All costs for each treatment included medical costs, non-medical costs, and costs caused by loss of productivity. In addition, because malaria-related administrative costs incurred in the military may decrease by reducing the incidence of malaria, this cost was also included (Table 1).
Table 1
Predicting the incidence of malaria in soldiers (veterans) during 2010–2012 according to chemoprophylaxis compliance and early diagnosis rate

µ1 = use of chloroquine and primaquine during May and October, µ2 = use of primaquine during the first 2 weeks of October, µ3 = early diagnosis of malaria with a RDT kit within 5 days of fever.
RDT = rapid diagnostic test.
![]()
Medical costs
During military service, malaria may occur during the period of military service or after the service period; thus, medical costs were estimated by dividing the subjects into soldiers on service and veterans. For soldiers who were supposed to receive inpatient treatment in the military hospital, no outpatient medical costs were considered. The inpatient medical costs for soldiers were calculated using the annual inflation rate of medical expenses and the inpatient costs for 50 people in 2013 provided by the Armed Force Medical Command. For veterans, both inpatient and outpatient medical costs were estimated based on data from 294 people who visited medical institutions due to the diagnosis codes B51 (P. vivax malaria), B53 (other specified malaria), and B54 (unspecified malaria) between January and December 2012, which were provided by the Health Insurance Review and Assessment Service (HIRA).
Transportation costs
For soldiers who were supposed to receive inpatient treatment in the military hospital, no transportation costs were considered. Transportation costs due to hospitalization were estimated by applying the inflation rate to the cost of medical evacuation per capita (8,100 KRW), which was calculated by multiplying the distance from the Division Medical Corps to the military hospital by the cost of fuel for ambulance use.12 For veterans, the transportation cost was estimated using data on the transportation cost per capita according to the type of medical institution obtained from the Korea Health Panel Survey. It was assumed that two outpatient treatments were performed, including a primary medical institution (clinic) visit prior to malaria diagnosis and an outpatient visit after inpatient treatment for malaria. With the assumption that inpatient treatments are implemented at the same rate in general hospitals and tertiary hospitals, the average transportation costs for the two types of medical institutions were used.
Caregiver costs for inpatient treatment
The cost of caregiver services needed for hospitalization was only calculated for veterans. For the hospitalization of soldiers, caregiver costs were not estimated because the use of paid caregivers or care provided by family members and relatives are impossible in military hospitals. The Korea Health Panel data reported that patients aged 20–29 years do not use a paid caregiver and 39.4% of them receive care from family caregivers or relatives.13 In the current study, the wages of family caregivers or relatives providing care were considered an opportunity cost and were calculated as caregiver costs for inpatient treatment. The family members or relatives were assumed to be in their 50s, and the length of the hospital stay was estimated to be 5 days. It was assumed that 39.4% of the patients received care from family members or relatives.
Costs of productivity loss
The cost of productivity loss due to outpatient treatment was calculated by multiplying the time required for outpatient treatment by hourly wages. The time required for outpatient treatment was divided into the time for treatment (outpatient visit + treatment) and the time for dispensing. Data obtained from the National Public Health and Medical Condition Survey in 2000 and the Korea National Health and Nutritional Examination Survey in 2005 were used. The hourly wages were estimated using the regular payments and employment rates of men aged 20–29 years in data provided by Statistics Korea. The cost of productivity loss due to inpatient treatment was calculated by multiplying the number of lost working days due to hospitalization and daily wages. The number of lost working days, which was estimated to be the median hospital stay length obtained from medical records in the military hospital and HIRA claims data, was 9 days for soldiers and 5 days for veterans. The wages of veterans were estimated from hourly regular payments and the employment rates of men aged 20–29 years using data provided by Statistics Korea. The wages of soldiers were estimated from the total loss of earnings due to military service (opportunity costs for the period of military service + career discontinuity for the period of military service) rather than using the unrealistically low wages of soldiers to prevent underestimating the benefits. A previous study reported that the total loss of earnings for a 2-year military service is 47.11 million KRW for high school graduates, 60.23 million KRW for 2-year college graduates, and 75.98 million KRW for 4-year college graduates.14 Assuming that the distribution of soldiers according to the level of education (including high school and 2- and 4-year college graduates) is equal, the daily wage, which was calculated by applying the annual wage growth rate (5%) to the results of the above study, was 68,188 KRW in 2010, 71,777 KRW in 2011, and 75,554 KRW in 2012.
Malaria-related administrative costs
The malaria-related administrative costs can be divided into the cost of vector control to prevent malaria mosquito breeding and the cost of an epidemiological survey for malaria patients. Because vector control to eradicate mosquitoes or larvae is necessary to prevent not only malaria but also other mosquito-borne diseases, this cost was not included in the cost estimation. By contrast, the cost of an epidemiological survey is influenced by the number of malaria patients. When four or more malaria infections occur within 2 weeks in a military unit such as a battalion, an epidemiological survey is conducted together with an investigation on the use of medications for malaria using through an onsite audit and mosquito control. The frequency of epidemiological surveys is related to the incidence of malaria, so it should be included in the cost estimation. Because 300,000 of 520,000 soldiers (which is equivalent to approximately half of the army troops) are stationed in malaria risk areas, the number of battalions was assumed to be 450. The actual frequency of epidemiological surveys implemented per battalion was unknown; thus, the frequency of epidemiological surveys was assumed to be the number that was equivalent to 10% of malaria cases. It was assumed that research teams composed of two people with a Master's degree and three people with a Bachelor's degree conducted epidemiological surveys for 2 days and prepared an improvement scheme for 3 days. The cost of epidemiological surveys was calculated using a wage growth rate of 5% and the personnel expenses of research assistants according to data published by the National Research Foundation of Korea.
Cost data sources
The costs required to implement the following interventions were estimated: current malaria chemoprophylaxis (Intervention 1), shortened malaria chemoprophylaxis (Intervention 2), and the early diagnosis and treatment of malaria (Intervention 3). The cost was defined as the direct costs related to the operation of each intervention and any indirect costs incurred concomitantly. For chemoprophylaxis, the cost of prophylactic medications and the administrative cost associated with the management and administration of prophylactic medications were included in the direct cost. By contrast, the cost related to the treatment of adverse events caused by the prophylactic medications was included in the indirect cost.
Costs of current chemoprophylaxis for malaria (Intervention 1)
The malaria chemoprophylaxis regimen that is currently implemented in the military is the administration of 15 mg primaquine for 2 weeks from October 1 after the administration of 400 mg chloroquine once a week from May 1 to September 30. The cost of prophylaxis medications is calculated based on the price supplied by the Defense Procurement Agency of a price per tablet of 408 KRW for 400 mg chloroquine and 378 KRW for 15 mg primaquine. Accordingly, the total medication cost per capita is 13,452 KRW for 20 tablets of 400 mg chloroquine and 14 tablets of 15 mg primaquine. Because individual military units get a supply of medications and deliver them directly to individuals, costs related to transportation, time, and management are excluded from the cost of the malaria chemoprophylaxis. Personnel expenses are not included because the additional personnel expenses associated with the administration of medications are unpaid. Costs related to adverse events caused by the medications used for chemoprophylaxis are calculated by dividing the total cost into the cost of treatment for adverse events and the cost of work loss. The antibody-positive rates and malaria risk factors for soldiers who were stationed in the Paju area in 201315 were used to examine the frequency and type of adverse events caused by the use of prophylaxis medications. In the current study, the frequency of adverse events due to the use of primaquine and chloroquine was 5.2% and 8.1%, respectively. All of the adverse events caused by primaquine were gastrointestinal diseases. Most of the adverse events caused by chloroquine were mild and included gastrointestinal diseases (91%) and headaches (9%). All of the adverse events were mild, so it was thought that these symptoms would be resolved with only one outpatient treatment. The cost of treatment-related adverse events was estimated using the medical fee per outpatient visit to a physician according to the National Insurance Statistical Yearbook: 17,636 KRW in 2010, 18,427 KRW in 2011, and 19,007 KRW in 2012. It was assumed that no transportation costs or work loss costs were incurred because medications for mild adverse events can be administered within the military.
Costs of shortened chemoprophylaxis for malaria (Intervention 2)
Unlike current malaria chemoprophylaxis, this method administered 15 mg primaquine for 2 weeks from October 1 without chloroquine. The total medication cost per capita was 5,292 KRW based on a price of 378 KRW per 15 mg tablet of primaquine. Personnel expenses and management costs were excluded from the cost estimation, as with current chemoprophylaxis. It was presumed that the rate of adverse events due to the use of primaquine was 5.2%, and that all of the adverse effects were gastrointestinal. The cost of adverse events was estimated as described above for current chemoprophylaxis.
Costs of early diagnosis for malaria (Intervention 3)
According to the uninsured medical expenses reported by general hospitals in Korea, the testing cost with RDT kits ranges from 13,000 to 30,000 KRW. Considering the price of the RDT kits available in Korea, logistical costs, and the cost of incidental materials, the cost required for implementing an RDT test once was assumed to be 20,000 KRW. The RDT kit storage and testing costs were not considered with the assumption that the early diagnosis of malaria is performed by an army doctor or medic in the battalion. Forecasting the demand of RDT kits is required to estimate the cost of early diagnosis. The following three methods were used to quantify the demand for RDT kits for malaria diagnosis within 5 days of fever in the current study. The first method was to add the number of RDTs implemented and the number of malaria patients who did not use an RDT. A total of 10,000 RDT kits are purchased annually by the military, and 20% of these are reserved. Accordingly, the number of RDT implementations can be estimated to be 8,000 RDT kits used, excluding the amount stored. The number of cases in which RDTs were not implemented was estimated by multiplying the number of malaria cases occurring in the military (695 cases in 2010, 434 cases in 2011, and 151 cases in 2012) and the number of RDT kits that were not used for malaria cases occurring in places other than the military (70% in 2010, 76% in 2011, and 83% in 2012). According to this method, the annual demand for RDT kits was estimated to be 8,486 kits in 2010, 8,330 kits in 2011, and 8,125 kits in 2012. The second method was to assume that the use of RDT kits will increase by 50% compared to the existing use, if early diagnosis is adopted as a strategy for malaria control, which would lead to the estimation that 15,000 RDT kits will be used annually. The third method was to estimate the demand for RDT kits based on the treatment volume for patients with fever under the premise that 450 Medical Corps in malaria risk areas are in charge of early diagnosis. Based on experts' opinions, it was assumed that an average of three patients with fever per day receive treatment in the Medical Corps, and one of these three patients uses an RDT when the cause of fever is unclear. It was estimated that 81,000 (180 × 450) RDT kits per year would be necessary if daily treatment for malaria was possible for the 6 months between May and October in which malaria mainly occur. This method was estimated based on the treatment volume of the Medical Corps conducting the early diagnosis; therefore, it could be the most realistic method of demand forecasting rather than a theoretical estimation.
Benefit-cost ratio analysis depending on the malaria prevention strategy
Data regarding the costs and benefits of the three prevention strategies were collected, but Intervention 2 did not affect the number of malaria cases in a mathematical model, so it was excluded from the final economic evaluation. In the military, current chemoprophylaxis (Intervention 1) or shortened chemoprophylaxis (Intervention 2) are implemented depending on the risk of malaria, and early diagnosis using RDTs (Intervention 3) is performed at the same time. Accordingly, the benefit-cost ratio analysis for each intervention (Intervention 1/Intervention 3) as well as a combination of Intervention 1 and Intervention 3 were conducted.
Sensitivity analysis
Sensitivity analyses were performed for chemoprophylaxis compliance (whether prophylaxis medications were administered regularly according to the dose regimen) which may affect the benefit-cost ratio, the early diagnosis rate (rate of diagnosis and administration within 5 days of fever), and the demand for RDT kits. Because a previous study reported that 50%–60% of soldiers regularly took prophylaxis medications,15 sensitivity analyses for chemoprophylaxis compliance were conducted with two assumptions of 50% and 70%. For the early diagnosis rate, two assumptions of 50% and 70% were used in the sensitivity analysis because it was difficult to identify the relevant epidemiological data.
RESULTS
Predicting the number of malaria cases
In the case of combining Interventions 1, 2, and 3 at the same chemoprophylaxis compliance and early diagnosis rate as actual clinical settings, the number of malaria cases can be estimated to be 402 cases and 286 cases, which is almost the same as the actual number of malaria cases. The reduction in malaria cases from baseline with Intervention 1 and Intervention 3 was 82% and 77% for soldiers and 47% and 31%, respectively, for veterans. The number of malaria cases depending on the combination of control strategies and the increase in chemoprophylaxis compliance or RDT rates was estimated (Table 1).
Benefit prediction
The cost of treatment and management per malaria patient in 2010 was 1,414,042 KRW for soldiers and 1,266,277 KRW for veterans. The combined inpatient and outpatient medical expenses were 711,877 KRW for soldiers and 714,414 KRW for veterans. The transportation costs for soldiers and veterans were 11,473 KRW and 30,311 KRW, respectively. Caregiver costs were not considered for soldiers and were an estimated 406,277 KRW for veterans. The cost of productivity loss was estimated at 613,692 KRW for soldiers and 194,980 KRW for veterans. For 2011 and 2012, the relevant costs were estimated in view of price and wage inflation rates (Table 2). The total benefit was calculated by multiplying the cost of treatment and management per patient by the reduced number of patients per malaria prevention strategy. For the same prevention strategy, the reduced number of patients varies depending on the chemoprophylaxis compliance and early diagnosis rate, so the total benefit differs. The total benefit of current chemoprophylaxis was estimated to be 6.6 billion to 7 billion KRW, and 6.9 billion to 7.3 billion KRW when early diagnosis methods were added. When only early diagnosis methods were used, the total benefit was 6 billion to 6.1 billion KRW. There was no large difference in total benefit with the single use of early diagnosis methods and the combination of chemoprophylaxis and early diagnosis methods.
Table 2
Details of benefit per reduction in malaria infection

![]()
Cost estimation
The cost of current malaria chemoprophylaxis was estimated to be 3.3 billion (2012) to 4.9 billion KRW (2010) and 1.3 billion (2012) to 2 billion KRW (2010) for shortened chemoprophylaxis. In addition, the cost of early diagnosis was estimated to be 1.6 billion to 3 billion KRW based on demand prediction methods (Table 3).
Table 3
Cost of each control measure by year

Unit: one million KRW (average exchange rate in 2010 was 1 USD = 1,156.86 KRW). Estimated RDT kit demand based on suspected cases and tested cases using the RDT kit (Early diagnosis demand ①), estimating that the RDT kit demand will increase by 50% (Early diagnosis demand ②), estimating that 450 medical corps use RDT kits for febrile patients (Early diagnosis demand ③); the number is empirically estimated.
CQ = chloroquine, PQ = primaquine, µ1 = use of chloroquine and primaquine during May and October, µ2 = use of primaquine during the first 2 weeks of October, µ3 = early diagnosis of malaria with a RDT kit within 5 days of fever, RDT = rapid diagnostic test.
![]()
Benefit-cost ratio
The total benefit of all control strategies was estimated to range from 6 billion to 7.2 billion KRW depending on the drug compliance and early diagnosis rates. The benefit-cost ratio was less than one for Intervention 1, regardless of drug compliance, and was also less than one for the combination of Interventions 1 and 3. Because the benefits were less than the costs, both strategies were uneconomical. For Intervention 3, the benefit-cost ratio was greater than one, irrespective of the demand forecasting for RDT kits and the early diagnosis rate; therefore, this strategy was considered economical (Table 4).
Table 4
Benefit-cost ratio of chemoprophylaxis and early diagnosis by changing chemoprophylaxis compliance and the early diagnosis rate
Unit: KRW (average exchange rate in 2010 was 1 USD = 1,156.86 KRW). Estimated RDT kit demand based on suspected cases and tested cases using the RDT kit (Early diagnosis demand ①), estimating that the RDT kit demand will increase by 50% (Early diagnosis demand ②), estimating that 450 medical corps use RDT kits for febrile patients (Early diagnosis demand ③); the number is empirically estimated.
µ1 = use of chloroquine and primaquine during May and October, µ3 = early diagnosis of malaria with a RDT kit within 5 days of fever, B-C ratio = benefit-cost ratio, RDT = rapid diagnostic test.
![]()
DISCUSSION
Mass chemoprophylaxis was introduced to reduce the incidence of malaria, which rapidly increased among soldiers stationed near the DMZ. Although this method has helped reduce the incidence of malaria to some extent, a new malaria control strategy has become necessary because of the possibility of inducing resistance due to low drug compliance and the reduced risk of infection. In this study, three strategies for malaria control (current chemoprophylaxis, shortened chemoprophylaxis, and early diagnosis methods) were evaluated using mathematical modeling and benefit-cost ratio analysis. The results showed that the number of malaria cases was decreased most by current chemoprophylaxis using chloroquine and primaquine. In addition, although the early diagnosis method reduced the incidence of malaria, the reduction was less than that achieved with the current chemoprophylaxis. However, the results of economic evaluation by estimating benefits and costs revealed that the early diagnosis method had the highest benefit-cost ratio and was the most economical.
Mathematical models have been studied less for P. vivax than for P. falciparum. A mathematical model was used to estimate the expected number of malaria cases using characteristics of the type of malaria commonly reported in Korea.16 In addition, two studies were conducted to estimate the effectiveness of chemoprophylaxis using a mathematical model. The first study showed that mass chemoprophylaxis helps reduce secondary transmission by assessing temporal trends in the transmission of P. vivax in Korea.17 The second study showed that the policy of attempting to lower the vectorial capacity by providing bed-nets and implementing chemoprophylaxis in the Solomon Islands could decrease the prevalence of P. vivax.18 However, this study is the first to provide evidence for policy decision-making based on comparing malaria control strategies using a mathematical model.
Sir Ronald Ross developed a mathematical model to understand malaria transmission patterns at the population level and he was awarded the first Nobel Prize in Physiology or Medicine in 1902. His malaria mathematical framework led to the development of the mathematical theory of infectious diseases.19 Since then, mathematical modeling has been successfully used to investigate the transmission dynamics of various infectious diseases.2021 It has been helpful to give valuable insights to predict the complex characteristics of epidemics especially when no experimental approaches are available or possible. We develop and analyze a mathematical model similar to those proposed in order to study the dynamics of malaria transmission with relevant epidemiological data in Korea.2021
Although malaria control strategies have been evaluated economically in other countries,22 no studies have compared chemoprophylaxis and early diagnosis methods. In Korea, a cost-effectiveness analysis of chemoprophylaxis was conducted to assess the malaria incidence rate according to the standard of prophylaxis medication administration. However, there were many omissions from the cost and benefit items and there was only one alternative. Therefore, the data were limited for conducting an exact economic evaluation.12 For this reason, the current study is the first to systematically conduct a cost-effectiveness analysis for chemoprophylaxis and early diagnosis methods.
There were several limitations due to limited data in this study. First, an actual value was not reflected in the mathematical model due to the limited data available related to mosquitoes. For exact calculations, it is most desirable to investigate the vector mosquito density and sporozoite infection rate of mosquitoes from May to October by collecting mosquitoes in the vicinity of military units stationed in malaria risk areas. Because these data were not available, the frequency of malaria vector mosquitoes in some locations where mosquitoes were collected and the daily mean density of vector mosquitoes were used in this study. Sporozoite positive rate in mosquitoes varied depending on region investigated and year.23242526 Values were obtained from a study which was conducted near DMZ in 2011.24 Second, because a mathematical model was designed on an annual basis, the effects of the number of patients infected in the previous year on the number of people infected in the following year were not considered. Regarding the epidemiologic features of malaria in Korea, the short incubation period (malaria incidence within 1 month from infection) and long incubation period (malaria incidence 8–12 months after infection) overlapped. Therefore, the number of people infected with malaria for 1 year is associated with not only the number of malaria cases in the year, but also with the number of patients infected in the previous year and undergoing the long incubation period. Although it is necessary to obtain a fitted value in view of the number of malaria cases for three consecutive years, the fitted value was calculated on an annual basis due to the complexity of designing a mathematical model. As a result, the possibility that patients infected in the previous year and undergoing a long incubation period will infect people in the following year was not considered in the mathematical model. Third, the administrative costs such as those related to quality control, education were not considered for the implementation of early diagnosis. When planning the expansion of RDT kits, it is necessary to purchase quality-assured RDT kits, select the subjects for testing in the military, and educate them about these kits. In addition, procedure monitoring to assess whether the plan is properly implemented in the field and post-evaluation should be conducted at the same time. To properly diagnose and treat patients with fever caused by factors other than malaria, it is necessary to develop algorithms that can manage cases that are RDT-negative for malaria. People in charge of conducting the test and soldiers should be aware of the need to test using RDT kits for the differential diagnosis of malaria, depending upon the clinical symptoms when patients present with fever in the military unit.
If fever persists despite the diagnosis and treatment of non-malarial febrile illness due to the low possibility of early stage malaria, the patient should visit a hospital and undergo testing using an RDT kit. In addition to medication costs, the costs related to education (which is needed to properly implement this strategy) and medication quality assurance must be included in the costs required for expanding early diagnosis using RDT kits. However, in this study, these costs were not considered due to difficulties with cost estimation. Since establishing a management system for patients with fever can help prevent a secondary infection by expanding early diagnosis and also reduce the use of unnecessary medications and tests,27 it was presumed that the benefit-cost ratio would not be influenced because of the increase in benefits. In addition, it is necessary to consider any additional benefits that could be expected, aside from reducing the number of patients. In this study, the results of a study on the economic costs of mandatory military service were used to quantify the loss of national defense due to soldiers infected with malaria.14 However, because only labor costs in the general labor market was considered in the abovementioned study, the fact that the malaria risk area is a contact area of the Korean army where the military force cannot be easily replaced was not reflected. Thus, the application of multiple value criteria would be necessary to assess national defense loss in the contact area.
Although the aforementioned limitations were present, this study remains significant because a mathematical model was established based on data regarding the incidence of malaria in the military and a benefit-cost ratio analysis by collecting data related to all costs and benefits from a societal perspective. Based on the results of the current study, we suggest the following. First, the implementation of chemoprophylaxis was a useful policy for reducing the incidence of malaria. However, the development of alternative strategies is needed because the costs exceed the benefits due to a reduced number of patients and the risk of drug resistance due to low compliance. Second, the strategy of early diagnosis using RDT kits is effective for reducing the incidence of malaria and economical compared to chemoprophylaxis. In addition, because the early diagnosis method has no risks of drug resistance and adverse effects, it may be a suitable malaria control strategy that could replace chemoprophylaxis. Third, to establish an early diagnosis method as a malaria control strategy, it is necessary to purchase confirmed RDT kits and educate users about their use. In addition, the development of new algorithms and systematic education for the algorithm and evaluation would be needed to ensure consistent measures for patients with fever.
 XML Download
XML Download