

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Epilepsy is one of the most common neurological disorders in children. The prevalence of epilepsy in children ranges from 3.2 to 5.5/1,000 in developed countries and from 3.6 to 44/1,000 in developing countries.12 Children with epilepsy are at higher risk of neuropsychological disorders, such as learning disability, attention deficit hyperactivity disorder (ADHD), depression, and anxiety disorder.134 There is a prevalence of these neuropsychological comorbidities in children with epilepsy of 20%–60%.5 The wide variation in prevalence rate originates from differences in the study populations and methodologies.
Neuropsychological comorbidities in epilepsy are reportedly associated with epilepsy subgroup, age of seizure onset, seizure type and frequency, lateralization of interictal epileptiform discharges (IEDs) on electroencephalography (EEG), administration of antiepileptic drugs (AEDs), and psychosocial environment.367 Parents of children with epilepsy and neuropsychological comorbidities often believe that the neuropsychological problems originate from extrinsic factors other than epilepsy, such as AED administration. However, previous studies have reported that some patients with epilepsy already have neuropsychological problems at the time of their initial diagnosis.4891011 Early detection of and appropriate interventions for neuropsychological comorbidities in children with epilepsy is important because it may affect long-term neuropsychological outcome.8
The purpose of this study is to investigate cognitive function and neuropsychological comorbidities in AED-naïve children with newly diagnosed idiopathic epilepsy. It also aims to identify whether there are differences in cognitive function and neuropsychological comorbidities depending on epilepsy classification, EEG findings, and variables related to seizures in this patient group.
METHODS
Participants
Participants were patients admitted to the Pediatric Neurology Clinic at Ulsan University Hospital, Ulsan, Korea between April 2011 and April 2015, with the chief complaint of seizures. We recruited 131 patients, aged 5–17 years, who underwent a neuropsychological assessment battery as an initial diagnostic work-up. Among these patients, we identified those who were AED-naïve with newly diagnosed idiopathic epilepsy. We excluded 13 patients for whom AED had been administered prior to neuropsychological tests, 9 patients who had abnormalities on brain magnetic resonance imaging (MRI), 10 patients in whom the interval between initial seizure and neuropsychological tests was more than 30 months, and 2 patients who had full-scale intelligence quotients (FSIQs) below 50. We included an 8-year-old boy who showed Arnold-Chiari malformation I on brain MRI, as the abnormal MRI finding was considered not to be associated with his seizures. Finally, 97 patients were included in the study (Fig. 1). Of these, 49 (50.5%) patients underwent brain MRI, and the remaining 48 patients (40.5%) did not. No patients had a history of developmental delay or status epilepticus.
 | Fig. 1Study population and distribution of patients according to epilepsy classification.
AED = antiepileptic drug, MRI = magnetic resonance imaging, FSIQ = full-scale intelligence quotient, IGE = idiopathic generalized epilepsy, BCECTS = benign childhood epilepsy with centrotemporal spike, ILRE = idiopathic localization-related epilepsy.
|
Neuropsychological battery
The neuropsychological battery consisted of an intelligence quotient (IQ) test, Stroop Color and Word Test Children's Version, Children's Color Trails Test, ADHD Rating Scale-IV (ARS-IV), visual and auditory ADHD Diagnostic System (ADS), Children's Depression Inventory, and State-Trait Anxiety Inventory for Children. To evaluate cognitive function, full-scale, verbal, and performance intelligence quotients (FSIQ, VIQ, and PIQ) were measured in all patients using the Korean-Wechsler Intelligence Scale for Children-III (n = 84, 86.6%), Korean-Wechsler Preschool and Primary Scale of Intelligence (n = 12, 12.4%), and Korean-Wechsler Adult Intelligence Scale (n = 1, 1.0%), depending on the patient's age. To evaluate executive function, we administered the Stroop Color and Word Test Children's Version (n = 92, 94.8%), and the Children's Color Trails Test (n = 96, 99%). T-score in one or more parameters for the Stroop Color and Word Test Children's Version less than 40 were considered “impaired”.12 T-score in one or more parameters for Children's Color Trails Test below the 16th percentile were considered “impaired”.13 To evaluate the presence of ADHD, we used ARS-IV (n = 91, 93.8%) and the visual (n = 97, 100%) and auditory (n = 94, 96.9%) ADS. In this study, a total ARS-IV score of 19 or greater was defined as ADHD.14 For the visual and auditory ADS subscales, evaluation parameters consisted of 4 categories: omission error, commission error, response time, and response time variability. T-scores of 65 or greater in one or more parameters were defined as possible ADHD.15 The Children's Depression Inventory (n = 73, 75.3%) was used to measure depressive symptoms, with depression defined as a score of 22 or greater.16 The State-Trait Anxiety Inventory for Children (n = 73, 75.3%) was used to measure anxiety symptoms, with an anxiety state defined as a score of 41 or greater in State Anxiety Inventory or 39 or greater in Trait Anxiety Inventory.17
Epilepsy classification
Epilepsy was classified based on the 1989 International League Against Epilepsy classification of epilepsies.18 Patients were classified into idiopathic generalized epilepsy (IGE) (n = 46, 47.4%) or idiopathic localization-related epilepsy (ILRE) (n = 51, 52.6%). Patients with IGE were further subcategorized into juvenile myoclonic epilepsy (n = 8, 17.4%), childhood absence epilepsy (n = 6, 13.0%), juvenile absence epilepsy (n = 1, 2.2%), and other IGE (n = 31, 67.4%). Meanwhile, patients with ILRE were subcategorized into benign childhood epilepsy with centrotemporal spikes (BCECTSs) (n = 24, 47.1%), and other ILRE (n = 27, 52.9%) (Fig. 1). Based on the EEG findings, other ILRE were subdivided into frontal lobe epilepsy (n = 10, 37.1%), occipital lobe epilepsy (n = 7, 25.9%), temporal lobe epilepsy (n = 5, 18.5%), parietal lobe epilepsy (n = 2, 7.4%), and others (n = 3, 11.1%). Three patients classified as others had IED over the entire unilateral hemisphere on EEG. We compared performance on the neuropsychological battery among the epilepsy groups.
EEG and lateralization of IED
All patients underwent EEG (Grass-Telefactor, West Warwick, RI, USA). EEG electrodes were placed according to the International 10–20 system. Based on the EEG findings, IGE was defined when synchronous and symmetrical generalized IED appeared in both hemispheres, whereas ILRE was defined when focal IED appeared in one hemisphere or independently in both hemispheres. Of 46 patients with IGE, 3 patients (6.5%) had focal IED, as well as generalized IED on EEG. Two patients had focal IED in the frontal region, and another in the centroparietal region. We classified ILRE and its subgroups (BCECTS and other ILRE) into “unilateral” and “bilateral” groups, according to the lateralization of IED on EEG. The unilateral group was defined when focal IED were confined to one hemisphere. The bilateral group was defined when focal IED independently appeared in both hemispheres. We compared neuropsychological scores between the two groups. In addition, IQ scores were compared among the following three groups; unilateral ILRE, bilateral ILRE, and IGE.
Seizure variables
In all patients, we evaluated seizure duration before neuropsychological battery, age of seizure onset, and total number of seizures before neuropsychological tests. Seizure duration was categorized into 5 groups: less than 1 month, 1–6 months, 7–12 months, 13–24 months, and 25−30 months. Total number of seizures was categorized into 4 groups (1–3 times, 4–6 times, 7–10 times, and 11 or more times). We evaluated correlations between these seizure variables and neuropsychological battery results.
Neuropsychological association with ADHD
We also compared neuropsychological performance between patients with ADHD (total ARS-IV score ≥ 19) and patients without ADHD (total ARS-IV score < 19).
Statistical analysis
All statistical analyses were conducted with IBM SPSS Statistics version 21 (IBM Corporation, Armonk, NY, USA). Independent t-tests were used to compare scores for the neuropsychological battery among epilepsy groups based on epilepsy classification, and between unilateral and bilateral ILRE. Mann-Whiney U tests were used to compare the BCECTS and other ILRE groups. The analysis of variance (ANOVA) test and Scheffe's post hoc test were used to compare IQ scores between unilateral ILRE, bilateral ILRE, and IGE. ANOVA tests were used to analyze the relationship between seizure duration before neuropsychological battery and neuropsychological battery scores. Pearson correlation analysis was used to analyze the relationship between age of seizure onset and neuropsychological battery scores. The Kruskal-Wallis test was used to analyze the relationship between total number of seizures and neuropsychological variables. Finally, the Mann-Whiney U test was used to analyze the relationship between ADHD diagnosis and neuropsychological battery scores.
RESULTS
Participant demographics
We recruited 54 male patients (55.7%) and 43 female patients (44.3%) with a median age of 10.1 years (interquartile range, 7.8–12.4 years). The mean age of seizure onset was 9.7 ± 2.9 years.
Neuropsychological battery results
Patients had mean FSIQ, VIQ, and PIQ scores of 92.8 ± 16.5, 93.0 ± 16.3, and 93.2 ± 16.8, respectively. Nine patients (9.3%) had a FSIQ score below 70, while 35 patients (36.1%) had a FSIQ score ≥ 100. Impaired executive function was indicated in 34 patients (37.0%) on the Stroop Color and Word Test Children's Version and 28 patients (29.2%) on the Children's Color Trails Test. ADHD was diagnosed in 13 patients (14.3%), while 56 (57.7%) and 46 patients (48.9%) had possible ADHD based on the visual and auditory ADS, respectively. Finally, 3 patients (4.1%) had depressive symptoms and 9 patients (12.3%) had anxiety symptoms.
Association between neuropsychological performance and the epilepsy classification
Patients with IGE had significantly lower FSIQ and PIQ scores than patients with ILRE (89.0 ± 17.6 vs. 96.3 ± 14.8; P = 0.030 and 88.9 ± 16.3 vs. 97.0 ± 16.4; P = 0.016, respectively), but did not have lower VIQ scores (Fig. 2A). There were no significant differences in FSIQ, VIQ, and PIQ scores between patients with IGE and BCECTS (Fig. 2B). Meanwhile, patients with IGE had significantly lower PIQ scores than patients with other ILRE (88.7 ± 16.4 vs. 97.5 ± 16.0; P = 0.042, Fig. 2C), but did not have lower FSIQ or VIQ scores. Compared with patients with ILRE, patients with IGE had lower scores for the “omission error” category of the visual ADS (57.5 ± 23.4 vs. 72.3 ± 34.2; P = 0.014). There were no significant differences in scores for neuropsychological tests other than the “omission error” category of the visual ADS between IGE and ILRE.
 | Fig. 2Comparison of IQ scores according to epilepsy classification. (A) Idiopathic generalized epilepsy vs. idiopathic localization-related epilepsy. (B) Idiopathic generalized epilepsy vs. benign childhood epilepsy with centrotemporal spikes. (C) Idiopathic generalized epilepsy vs. other idiopathic localization-related epilepsy.
IQ = intelligence quotient, IGE = idiopathic generalized epilepsy, ILRE = idiopathic localization-related epilepsy, BCECTS = benign childhood epilepsy with centrotemporal spike, FSIQ = full-scale intelligence quotient, VIQ = verbal intelligence quotient, PIQ = performance intelligence quotient.
aP < 0.05 by independent t-test.
|
Association between neuropsychological performance and lateralization of IED
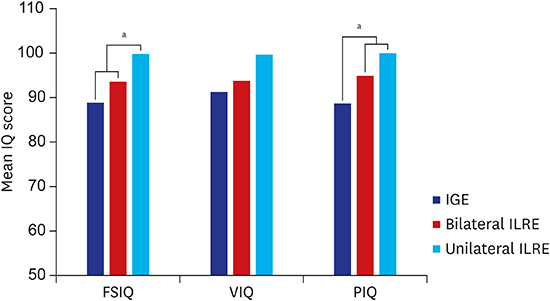
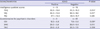
Of 51 patients with ILRE, 22 (43.1%) were classified as unilateral and 29 (56.9%) as bilateral. Of 24 patients with BCECTS, 7 (29.2%) were classified as unilateral and 17 (70.8%) as bilateral. Of 27 patients with other ILRE, 14 (51.9%) were classified as unilateral and 13 (48.1%) as bilateral. Although the bilateral group had lower mean FSIQ, VIQ, and PIQ scores than the unilateral group for patients with ILRE, BCECTS, and other ILRE, these differences were not statistically significant (Table 1). The FSIQ scores of patients with ILRE in the unilateral group (99.9 ± 12.2) were significantly higher than those of the bilateral group (93.7 ± 16.1), and patients with IGE (89.0 ± 17.6) (P = 0.039, Fig. 3). The PIQ scores of patients with ILRE in the unilateral group (100.1 ± 12.9) and bilateral group (94.9 ± 18.3) were significantly higher than those of patients with IGE (88.9 ± 16.3) (P = 0.030) (Fig. 3). There were no significant differences in results of other neuropsychological scores between the unilateral and bilateral groups for patients with ILRE, BCECTS, or other ILRE.
Table 1
Comparison of IQ scores according to lateralization of IED in ILRE and its subgroups

Values are expressed as mean ± standard deviation.
IQ = intelligence quotient, IED = interictal epileptiform discharge, ILRE = idiopathic localization-related epilepsy, BCECTS = benign childhood epilepsy with centrotemporal spike, FSIQ = full-scale intelligence quotient, VIQ = verbal intelligence quotient, PIQ = performance intelligence quotient.
aIndependent t-test; bMann-Whitney U test.
![]()
 | Fig. 3Comparison of IQ scores among IGE and ILRE with bilateral or unilateral IED.
IQ = intelligence quotient, IED = interictal epileptiform discharge, IGE = idiopathic generalized epilepsy, ILRE = idiopathic localization-related epilepsy, Unilateral ILRE = idiopathic localization-related epilepsy with unilateral interictal epileptiform discharges, Bilateral ILRE = idiopathic localization-related epilepsy with bilateral interictal epileptiform discharges, FSIQ = full-scale intelligence quotient, VIQ = verbal intelligence quotient, PIQ = performance intelligence quotient, ANOVA = analysis of variance.
aP < 0.05 by ANOVA and Scheffe's test.
|
Association between neuropsychological performance and seizure variables
There was no correlation between the scores of each neuropsychological test including IQ test and the following seizure variables: seizure duration before the neuropsychological tests, age of seizure onset, and total number of seizures before neuropsychological tests.
Association between neuropsychological performance and ADHD
Patients with ADHD had significantly lower FSIQ and VIQ scores than patients without ADHD (83.9 ± 16.0 vs. 95.3 ± 15.5; P = 0.014 and 84.2 ± 12.6 vs. 96.5 ± 16.1; P = 0.011, respectively), but they did not have lower PIQ scores (Table 2). Patients with ADHD also had higher scores in the “omission error” category of the auditory ADS (71.3 ± 23.8 vs. 55.2 ± 16.6; P = 0.017). Scores for the Children's Depression Inventory in patients with ADHD were significantly higher than those in patients without ADHD (12.3 ± 6.6 vs. 7.8 ± 5.8; P = 0.031, Table 2). There were no significant differences in results for the other neuropsychological tests between patients with ADHD and patients without ADHD.
Table 2
Comparison of IQ scores and questionnaire results depending on the presence of ADHD
Values are expressed as mean ± standard deviation.
IQ = intelligence quotient, ADHD = attention deficit hyperactivity disorder, FSIQ = full-scale intelligence quotient, VIQ = verbal intelligence quotient, PIQ = performance intelligence quotient, CDI = Children's Depression Inventory, SAIC = State Anxiety Inventory for Children, TAIC = Trait Anxiety Inventory for Children.
aP < 0.05 (Mann-Whitney U test).
![]()
DISCUSSION
In the present study, we observed that neuropsychological problems, including abnormal executive function, ADHD, depression, and anxiety are already present in some children with idiopathic epilepsy at the time of initial diagnosis and before AED administration. Nonetheless, many patients and their parents had not complained of any specific neuropsychological symptoms except for seizures. There appear to be differences in neuropsychological function depending on epilepsy classification, with patients with IGE having lower FSIQ and PIQ scores than patients with ILRE. In addition, lateralization of IED is also associated with neuropsychological function, with patients with ILRE and unilateral IED having significantly higher FSIQ scores than patients with ILRE and bilateral IED, and patients with IGE. Lastly, we also found that patients with comorbid ADHD had significantly lower FSIQ and VIQ scores than patients without ADHD.
The association between childhood epilepsy and neuropsychological comorbidities, including cognitive impairment, has long been recognized. However, the mechanisms and contributing factors for this relationship remain unknown. Compared with children with symptomatic epilepsy accompanied by specified causes of epilepsy, such as brain anomalies and chromosome abnormalities, neuropsychological comorbidities are more likely to be overlooked in children with idiopathic epilepsy. However, as neuropsychological comorbidities can seriously affect quality of life in patients with epilepsy, early detection is vital to prevent further impact. There is a higher prevalence of ADHD in patients with epilepsy than in typically developing children (28%–70% vs. 5%–10%).19 Furthermore, compared with the general population, patients with epilepsy have a higher prevalence of depressive disorder (10%–36% vs. 1%–2%) and anxiety disorder (24%–35% vs. 3%–8%).1520212223 In this study, we identify ADHD, depression, and anxiety in 14.3%, 3.0%, and 9.3% of patients, respectively. Compared with results from previous studies, the prevalence of these neuropsychological comorbidities in this study population was higher than in general populations, but lower than in patients with epilepsy. The differences in prevalence appear to originate from several methodological factors. First, in this study, diagnosis of neuropsychological disorders was made based on the result of questionnaires completed by patients' parents, rather than a clinical diagnosis made by a psychiatrist. Second, the neuropsychological tests were performed in all patients with newly diagnosed epilepsy as screening tests even though neither patients nor their parents had complained of any specific neuropsychological symptoms except for seizures. It is possible that this caused parents to respond more positively on the questionnaires compared with parents who have visited the clinic with complaints of specific neuropsychological symptoms. Third, this study included only patients with newly diagnosed idiopathic epilepsy, excluding patients with symptomatic epilepsy and those who have previously taken AED. This might lead to a lower prevalence of neuropsychological comorbidities in our study. Nevertheless, compared with the general population, we observed a higher prevalence of neuropsychological conditions in children with newly diagnosed idiopathic epilepsy who are AED-naïve. This suggests that such comorbidities may be inherently present in these patients, rather than resulting from extrinsic factors, such as AED administration or uncontrolled seizures.
Indeed, there have been many studies investigating cognitive function in children with epilepsy, but these have mostly focused on intractable or catastrophic forms of epilepsy, such as West syndrome, Lennox-Gastaut syndrome, and Dravet syndrome.242526 Few studies have investigated cognitive function in patients with idiopathic epilepsy, and only a few studies have directly compared IQ scores between patients with IGE and those with ILRE, as we did.272829 In this study, we investigated whether there are differences in IQ scores between patients with IGE and those with ILRE, observing significantly lower FSIQ and PIQ scores in the former group. We assumed that diffuse IED over both hemispheres might have more negative effects on patient cognition than would focal IED. One previous study reported that children with IGE had significantly lower PIQ scores than children with BCECTS.27 Meanwhile, another reported that patients with IGE had lower PIQ scores than patients with temporal lobe epilepsy.28 However, a further study did not observe significant differences in any cognitive domains between children with IGE and children with ILRE.29 Therefore, further investigation is required to identify whether there are differences in cognitive function between IGE and ILRE.
Interestingly, we also observed that patients with ILRE and unilateral IED had significantly higher FSIQ scores than patients with ILRE and bilateral IED, and patients with IGE. This result appears to originate from two possible causes: IED and bilaterality of cerebral lesions. It has been known that frequent IED can impair cognitive performance in children.3031 In addition, IED can disrupt short-term cognitive processes.32 Meanwhile, in various neurological disorders, such as temporal lobe epilepsy, semantic dementia, and herpes simplex virus encephalitis, patients with bilateral cerebral lesions have much worse cognitive function than patients with unilateral lesions.33 When unilateral cortical tissues are damaged, the opposite intact side can compensate via brain plasticity in the highly interconnected system distributed bilaterally across the hemispheres of the brain.32 However, bilateral cerebral damage remarkably reduces the possibility of such compensation. Based on the results of this study, we presume that the presence of IED in both hemispheres may lead to lower FSIQ in patients with IGE and patients with ILRE and bilateral IED, regardless of synchronicity of IED in both hemispheres.
In this study, we also observed lower FSIQ and VIQ scores in patients with comorbid ADHD than those without ADHD. This was not surprising because many children with ADHD have lower IQ scores than typically developing children, and working memory, inhibition, and expressive language are often impaired in ADHD.34 In terms of the pathophysiology of decreased cognitive function in patients with epilepsy and ADHD, it has been suggested that neuronal pathways involved in attention, interference, and working memory are potentially associated with ADHD, and the diffuse spikes-and-waves in patients with epilepsy involve the “fronto-insular-thalamic network”.35 Hence, the comorbid presentation of epilepsy and ADHD may relate to interference with broader areas of the cognitive network.
Another interesting finding of this study is that patients with comorbid ADHD had higher scores in the “omission error” category of auditory ADS than those without ADHD, but they did not have higher scores in the “commission error” category. Omission errors are significantly correlated with inattention, while commission errors are significantly correlated impulsivity.15 Previous studies also showed that compared to patients with ADHD only, patients with epilepsy and ADHD more often met the criteria for a predominantly inattentive type of ADHD than a combined type of ADHD.363738 This finding is important because inattention is strongly associated with academic underachievement in children with epilepsy.39 Meanwhile, patients with comorbid ADHD had higher Children's Depression Inventory scores than patients without ADHD in this study. However, this result does not mean that patients with comorbid ADHD are more likely have depressed mood since the scores are negligibly low in both groups considering the criteria for depression on the Children's Depression Inventory.
This study has several limitations. First, as this study was retrospective using a chart review, diagnosis of neuropsychological disorders was made based on the results of questionnaires, rather than using a clinical diagnosis made by a psychiatrist. Therefore, we determined the presence of depressive and anxiety symptoms but not a diagnosis of depressive disorder and anxiety disorder when aberrant scores were detected on the Children's Depression Inventory or State-Trait Anxiety Inventory for Children. Second, we did not include an age-matched control group. For this reason, although we compared the results of neuropsychological tests among subgroups of patients with idiopathic epilepsy, we could not perform a comparison of these patients with healthy controls. Third, as this study included 9 patients with mild intellectual disability (FSIQ below 70) and 48 patients in whom brain MRI was not performed, we cannot exclude the possibility of inclusion of patients with symptomatic epilepsy. Finally, some patients did not complete certain tests of the neuropsychological battery due to the patient's poor cooperation.
In conclusion, our results suggest that idiopathic epilepsy may be accompanied by a variety of neuropsychological comorbidities even at the time of initial diagnosis. In addition, patients with IGE, patients with ILRE and bilateral IED on EEG, and patients with comorbid ADHD were more likely to be at higher risk of decreased cognitive function. Further studies are needed to identify long-term neuropsychological outcomes and prognostic factors for children with idiopathic epilepsy. In addition, further investigations are required to elucidate the pathophysiology underlying neuropsychological comorbidities in patients with idiopathic epilepsy.
 XML Download
XML Download