

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In Seoul, about 2.5 μSv/h of radioactivity was detected on two roads in 2011. It was measured with a radiation detector in a car owned by one citizen. The radionuclide-contaminated roads were 5–6 m wide and 90–200 m long. They were opened to both cars and pedestrians, where a large number of people traveled to reach the subway station. Near these roads are schools, commercial properties, and apartment complexes.1 After receiving much media reportage, the Nuclear Safety and Security Commission and the Korean Institute of Nuclear Safety measured the level of radiation and analyzed the nuclides present in the asphalt concrete samples from the roads. It was demonstrated that the concentration of radioactivity of cesium-137 (137Cs) was 1.82–35.4 Bq/g.1 Responding to public concerns on these radionuclides contaminated roads, an epidemiological study supported by the Seoul Metropolitan Government was initiated.
137Cs is an artificial radioactive substance. It is a common product of a nuclear fission reaction that occurs in nuclear weapons, or in nuclear reactors, used for the generation of electricity at nuclear power plants.2 It has a half-life of about 30 years. Therefore, it can persist in the environment. When released into the atmosphere, radioactive 137Cs can travel thousands of kilometers before settling on the ground. Oral ingestion of contaminated food items is the greatest source of internal exposure, although exposures through inhalation and dermal contact are possible. External exposure to beta and gamma radiation can also occur, following release of radioactive Cs. In 1987, an accidental exposure to 137Cs in Goiania, Brazil resulted in the death of 4 people due to acute radiation syndrome and about 130,000 hospital admissions.3 In animal studies, an increase in cancer risk has been demonstrated after an internal or external exposure to a relatively high dose of 137Cs.2 The outcome of long-term, low dose exposure to 137Cs in humans, however, has not been reported.
Our first aim was to assess the dose of radiation exposure in each individual who participated in the study. Secondly, we aimed to determine and compare cancer incidence in both the study region where the contaminated roads were included and neighboring regions, by using the cancer registry. Further, we intended to gather information on the past medical history, mental health status and risk perception level of participants, by questionnaire survey. We also gathered information on the interventions expected of the government, by the residents. In a previous study, individual exposure to radiation was assessed.1 In this study, we report on the results of an epidemiological investigation of the two 137Cs contaminated roads in Seoul.
METHODS
Study participants
The target populations were residents of the region or pedestrians of the roads, to whom the questionnaires were distributed. The study region was Wolgye 2-dong, the second smallest administrative district, including 43 smaller districts (tongs), and the contaminated roads. As of January 31, 2012, there were 31,053 registered residents and 12,428 households. We recruited study participants using two different methods: a stratified, random sampling of households in the entire area of Wolgye 2-dong, and a survey of all school-going children and their families in Wolgye 2-dong. The stratified random sampling was carried out on the 43 smallest administrative districts. One person per household was selected, based on the 1,200 randomly sampled households (estimated sampling error 2.8%). All schools in the study region, and 3 childcare institutions near the contaminated roads participated in the study. A total of 10,631 individuals, comprising 1,470 adults and 9,161 students agreed to participate in the study. Two hundred fifteen incomplete questionnaire responders, 1,380 individuals who neither lived nor worked in Wolgye 2-dong, and 103 participants with missing information on age or gender were excluded. Finally, 8,875 people (28.6% of the target population) were analyzed in the present study. We allocated post hoc weights for analysis by age group and gender, based on the population registered in the corresponding gu-community office (Table 1).
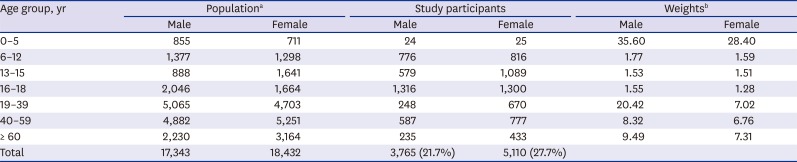
Table 1
Population, study participants and post hoc weights in the town (dong), including 137Cs contaminated roads, 2012, Wolgye 2-dong, Seoul
137Cs = cesium-137.
aThe total of 35,775 is not same as the 31,052 number of residents registered in the gu-community office, because in this table, the population was based on the number of registered residents in the corresponding gu-community office for 0–5, and 19 or older age groups, and numbers of students in all schools in the study region for 6–12 (elementary), 13–15 (middle), and 16–18 (high school) age groups based on the school reports; bweights calculated as the total population divided by the number of study participants.
![]()
Radiation exposure assessment
The assessment of exposure to radiation from the 137Cs contaminated roads has been previously described in detail.1 Briefly, we obtained information regarding the frequency of use of the contaminated roads by pedestrians, residents, and workers, via questionnaire administration. We calculated each individual's cumulative radiation dose, for the 8,875 participants, by combining information of measured doses reported by the Nuclear Safety and Security Commission. The mean duration of exposure was 4.75 years (range, 0.08 to 11.98 years). Geometric mean of the cumulative radiation dose was 0.049 mSv (range, < 0.001 to 35.35 mSv) in exposed participants (63% of the all participants). The cumulative radiation dose was categorized into tertiles for the analysis.
Cancer incidence
We identified cancer cases in each smaller district (dong) of Nowon-gu, one level higher than the administrative district of the study region. We covered 10 dong districts, including Wolgye-dong, using the Central Cancer Registry from 2000 to 2008.4 Target cancers were: all cancers (International Statistical Classification of Diseases and Related Health Problems, 10th revision; ICD-10 code, C00–C97), stomach cancer (C16), lung cancer (C34), colon cancer (C18–C20), thyroid cancer (C73), leukemia (C91–C96), non-Hodgkin's lymphoma (C82–C86), and female breast cancer (C50). Cancers were selected based on the International Agency for Research on Cancer (IARC) cancer classification5 and domestic incidence rates.
To compare cancer incidences between Wolgye-dong and neighboring districts at the administrative level, we used the total number of population from 2000 to 2008 in the resident register data6 as a standard population to calculate the age-standardized incidence rate and the gender-specific standardized incidence ratio (SIR).
History of disease diagnosis
We obtained information on the past medical history (if yes, the time of the disease diagnosis was requested) since the roads' construction in 2000 and after the respondent started living or working in the target area, Wolgye-dong.
The questionnaires were age-specific. For children aged ≤ 12 years, their parents/guardians responded to 20 items. For those aged > 12 years (students in middle and high schools, and adults), 38 questionnaire items were self-administered. Questions regarding previous diagnosis of asthma, congenital heart disease, epilepsy, juvenile diabetes mellitus (DM), attention deficit hyperactivity disorder (ADHD), thyroid disease, and cancer were asked, of children ≤ 15 years old. Questions regarding previous diagnosis of asthma, hypertension, hyperlipidemia, stroke, myocardiac infarction, angina, DM, thyroid disease, and cancer were asked of those aged > 15 years.
Mental health
The State-Trait Anxiety Inventory (STAI-X-1)78 and State-Trait Anxiety Inventory for Children (SAIC)910 were used to measure the anxiety levels, of those aged > 15 and those aged ≤ 15 years, respectively. The former was composed of 20 items with a 4-point scale and a sum score of 20 to 80. The cut-off score for high-risk group was 57 or more. The latter was composed of 20 items with a 3-point scale and a sum score of 20 to 60, with a cut-off score of 39.
We also used the short-form Psychosocial Wellbeing Index (PWI-SF) to assess the psychosocial stress levels of participants aged > 15 years, in which 18-items and a 4-point scale with a sum score of 0 to 54 were included.11 The sum score for the high-risk stress group was 27 or more.
Risk perception and needs
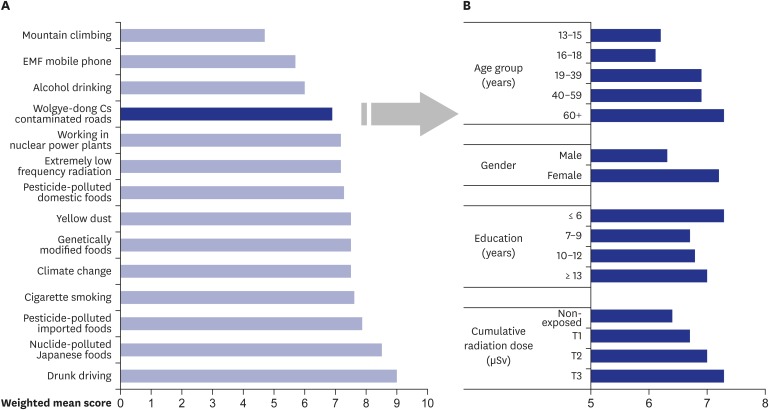
We used the visual analogue scale (VAS) of 0–10 to assess and compare the levels of perceived risk on 14 environmental or behavioral factors in relation to radiation exposure from 137Cs contaminated roads. The environmental and behavioral factors, reflecting currently raised concerns of the public and the media, assessed were: occupation at a nuclear power plant, drunk driving, yellow dust, nuclide-polluted Japanese foods, pesticide-polluted domestic foods, pesticide-polluted imported foods, genetically modified foods, climate change, power line, extremely low frequency radiation, mobile phone use, radiofrequency radiation, mountain climbing, smoking (or tobacco or cigarette use), and alcohol consumption.
To prioritize interventions expected of the government, participants were asked to choose the most important one among several tasks, i.e., economic compensation, long-term epidemiological monitoring, health examination, environmental management, education and provision of information, and improvement in the community's tarnished image as a radioactive polluted area.
Confounders and covariates
Via the questionnaire survey, we collected information on smoking (current, ex-, never smoker), and alcohol intake (yes, no). We also gathered information on medical radiation exposure, including diagnostic examinations, i.e., simple X-ray, fluoroscopy, computed tomography (CT), single photon emission CT, positron emission tomography CT, mammography, nuclear medicine examination (scans for liver, thyroid, bone), and radiotherapy (radiotherapy for head and neck, cancers, megalothymus) (if yes, the frequency for the past 10 years was requested). We calculated the total medical radiation exposure dose for the past 10 years using mean radiation dose of each examination or therapy,12 which was considered as a confounding factor in the analysis.
Statistical analysis
The rate of cancer incidence was standardized to 10-year age groups, using the population from 2000–2008 as the standard population. Mid-year populations of registered residents by sex, the 10-year age groups, and the administrative districts for each year were obtained from Statistics Korea6 and used as denominators. Stone's test13 was performed to compare cancer incidence in Wolgye-dong with those in neighboring regions. To estimate the risk of being diagnosed with a disease or high-risk deprived mental health, the survey logistic regression model was applied with adjustment for age group, gender, calculated medical radiation exposure dose, behavioral factors (smoking, and alcohol intake for those aged ≥ 16), and other covariates (birth weight and doctor's consultation history with respect to developmental problems in children aged ≤ 15). The odds ratio (OR) and its 95% confidence intervals (CIs) were calculated. The P value for the trend test was obtained in the corresponding survey logistic regression model, using a continuous scale of the variable. Statistical analyses were performed using R version, 2.15.2 (R Project for Statistical Computing, Vienna, Austria; http://www.r-project.org/)14 and SAS 9.1 (SAS Institute Inc., Cary, MC, USA) with a significance level at 0.05.
RESULTS
Cancer incidence in the region
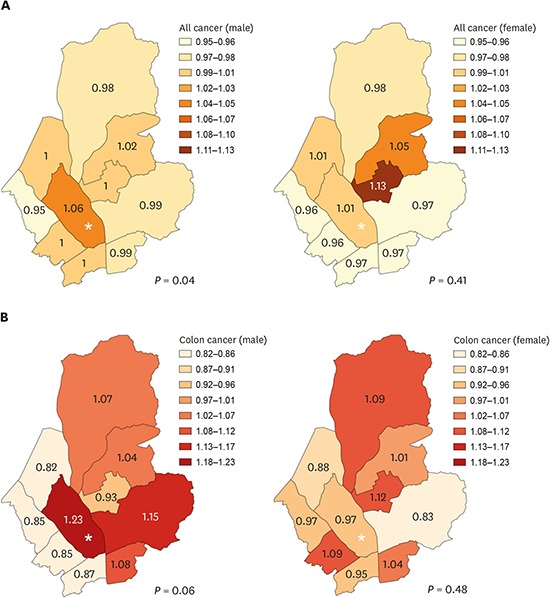
The incidence of all cancers in males in Wolgye-dong for 2000–2008 was higher (Stone's P = 0.040) than those in the neighboring regions, while there was no significant difference among regions in the female groups (Table 2). For site-specific cancers, colon cancer in males in Wolgye-dong showed the highest SIR (Stone's P = 0.060) (Fig. 1). However, other cancers in males or every types of cancer in females in Wolgye-dong were not significantly different from those in the neighboring regions (data not shown).
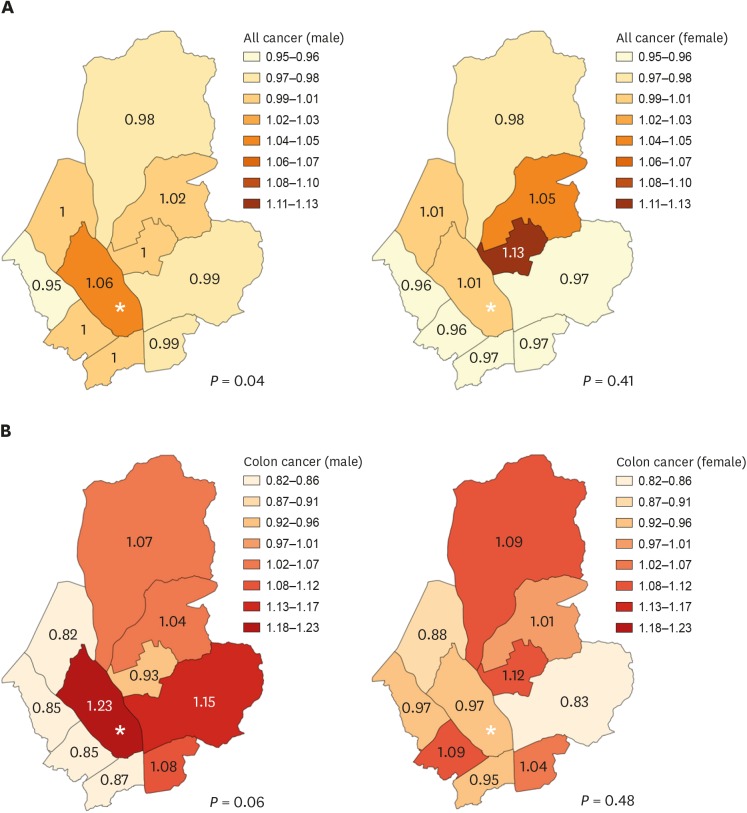
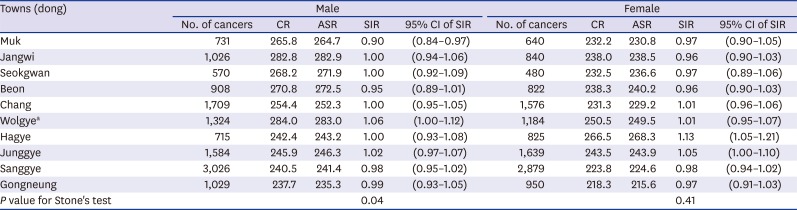
Fig. 1
SIR of cancer by study area and 10 neighboring communities. (A) all cancer and (B) colon cancer.
P value by the Stone's test to compare difference of SIRs among regions. Asterisks showed the study area, Wolgye-dong.
SIR = standardized incidence ratio.
![]()
Table 2
Standardized incidence rates of all cancers in the community (gu) including 137Cs contaminated roads; 2000–2008, Nowon-gu, Seoul
P value for Stone's test calculated to assess risk around given locations, using the SIRs.
137Cs = cesium-137, CR = crude incidence rate per 106 population, ASR = age-standardized incidence rate per 106 population, SIR = standardized incidence ratio calculated by indirect method, CI = confidence interval.
aThe town where the 137Cs contaminated roads were found.
![]()
History of disease diagnosed
In children aged 6–15 years old, there was no significant increase in disease history of congenital anomaly, asthma, ADHD, thyroid disease, or cancer, and no eligible case was reported of epilepsy and juvenile DM (Table 3). Among 6–12 year-old children who were born after the contaminated roads were constructed, there was no difference of disease risks between those born in the study region and born in other regions, meaning no evidence of prenatal exposure effects (Supplementary Table 1).

Table 3
Risk of being diagnosed with a disease in 3,260 children aged 6–15 in association with radiation exposure dose from the 137Cs contaminated roads, 2012, Wolgye-dong, Seoul
OR (95% CI) calculated using survey logistic regression model adjusted for age group, gender, medical diagnostic radiation exposure, and (for the 13–15 age group) cigarette smoking and alcohol intake. P-trend calculated using the continuous scale of cumulative radiation dose in the corresponding model.
The case includes those who were diagnosed with a disease after the roads were constructed and after they started to live in the target area. In the case of no information of exposure duration (missing start year to live in the area or year of disease diagnosed), considered unknown. T1, T2, and T3 of cumulative radiation dose (µSv); 0.02–26.1, 26.1–87.9, and 87.9–35,317.3, respectively.
137Cs = cesium-137, OR = odds ratio, CI = confidence interval, DM = diabetes mellitus, ADHD = attention deficit hyperactivity disorder.
![]()
In female residents aged > 15 years, there was a significant increasing trend of risk in hypertension with respect to an increase in the estimated cumulative radiation dose (P-trend = 0.01), whereas an increasing risk of hyperlipidemia in the highest tertile of cumulative radiation exposure was found (OR, 2.21; 95% CI, 1.29–3.78). However, other diseases including cancers in females and all diseases in males did not show a significant association with estimated radiation exposure dose (Table 4).
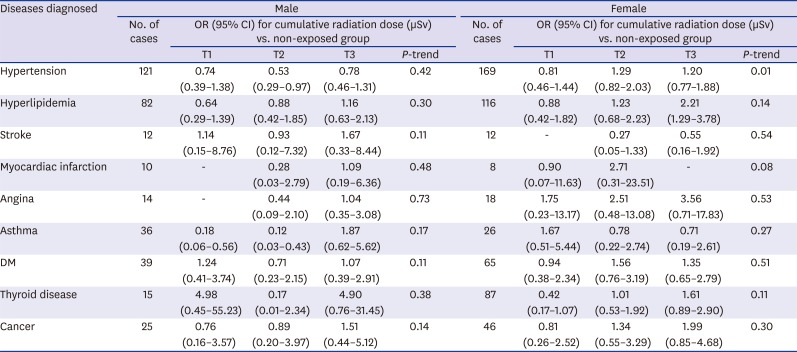
Table 4
Risk of having history of disease diagnosis in 5,566 residents aged 16 or older in association with radiation exposure dose from the 137Cs contaminated roads, 2012, Wolgye-dong, Seoul
OR (95% CI) calculated using survey logistic regression model adjusted for age group, gender, educational level, medical diagnostic radiation exposure, cigarette smoking and alcohol intake. P-trend calculated using the continuous scale of cumulative radiation dose in the corresponding model.
The case includes those who were diagnosed with a disease after the roads were constructed and after starting to live in the target area. In the case of no information of exposure duration (missing start year to live in the area or year of disease diagnosed), considered unknown. T1, T2, and T3 of cumulative radiation dose (µSv); 0.02–26.1, 26.1–87.9, 87.9–35,317.3, respectively.
137Cs = cesium-137, OR = odds ratio, CI = confidence interval, DM = diabetes mellitus.
![]()
Mental health
Anxiety level was not different with respect to gender in all age groups, while psychosocial wellbeing was worse in female adults than in males, showing a 16.3% and 21.7% prevalence of high stress group, respectively. The risk of high anxiety level increased significantly in relation to the increase in cumulative radiation dose in children of 6–12 years (P-trend = 0.001) and residents of > 15 years (P-trend = 0.01). In terms of psychosocial wellbeing, residents aged > 15 years showed significantly increased risk of having psychosocial stress, in relation to an increase in the cumulative radiation dose (P-trend < 0.001) (Table 5).

Table 5
Risk of high risk group of affected mental health in residents, in relation with the radiation exposure dose from the 137Cs contaminated roads, 2012, Wolgye-dong, Seoul
Anxiety measured by the STAI for the group of 16 years or older,78 and the SAIC for groups less than 16 years,910 with cut-off scores of high-risk group were ≥ 57 and ≥ 39, respectively. Psychosocial wellbeing measured by the PWI-SF,11 with a cut-off score for high-risk group was ≥ 27.
OR (95% CI) estimated by the survey logistic regression model adjusted by age group, gender, birth weight, and consulting history due to developmental problem for age group ≤ 12; age group, gender, cigarette smoking and alcohol intake for age group 13–15; and age group, gender, educational level, cigarette smoking, alcohol intake, and medical radiation exposure. P-trend calculated using the continuous scale of radiation dose in the corresponding model. T1, T2, T3 of cumulative radiation dose (µSv); 0.06–26.27, 26.28–87.87, 87.88–1,029.48 for age group ≤ 12, 0.02–26.12, 26.13–88.25, 88.26–773.99 for age group 13–15, and 0.02–26.19, 26.20–88.31, 88.32–35,317.3 for age group 16 or older.
137Cs = cesium-137, OR = odds ratio, CI = confidence interval, STAI = State-Trait Anxiety Inventory, SAIC = State-Trait Anxiety Inventory for Children, PWI-SF = short-form Psychosocial Wellbeing Index.
aPrevalence estimated by the survey analysis.
![]()
Risk perception and needs
Among 14 environmental or behavioral factors, the level of perceived risk of 137Cs contaminated roads was relatively lower than in others, except for mountain climbing, electromagnetic radiation, exposure by mobile phone use, and alcohol consumption (Fig. 2A). Since the order of perceived risk on these factors was different among age groups, we showed the result of 1,338 people aged 40–59 years, the empowered adults, as representative of the opinions of the community. The perceived risk level of the 137Cs contaminated roads was higher in older respondents, females, the less educated, and those who had higher exposure to radiation (Fig. 2B).
In response to the questions regarding the expectations from the government concerning the issue, respondents answered accordingly in the following order: health examination (80.0%), followed by environmental management (58.3%), economic compensation (35.5%), longer-term epidemiologic monitoring (29.5%), education and provision of information (20.7%), and some tasks to improve the community's image of being tagged as a radioactive polluted area (16.0%) in order (data not shown).
DISCUSSION
The study did not find evidence of association between self-reported diseases, including cancers, in residents and the estimated radiation exposure from the 137Cs contaminated roads, while the incidence of all cancers in males in the region where the contaminated roads were located was higher in comparison with those in the neighboring regions. Anxiety and psychosocial stress levels were significantly increased in relation to an increase in the estimated radiation exposure dose. The level of perceived risk concerning the contaminated roads was relatively low, compared to other types of environmental or behavioral factors. Perceived risk was higher in the older participants, in females, the less educated, and in those who had a higher exposure to the radiation.
In a previous study, we reported that an estimated cumulative radiation dose was reported to be more than 10 mSv in approximately 1% of participating residents (n = 61) and the geometric average of cumulative dose of over 12 years after the road was tarred was 0.049 mSv (range, < 0.001 to 35.35 mSv),1 which was far below the legally acceptable level of 1 mSv a year for the general population.15 In the case where construction materials were contaminated with 60Co in Taiwan,16 an estimated cumulative dose among residents of the apartments over a 10-year period was found to be between 47.8–150.7 mSv, which was quite higher than that noted in the present study. An increase in the incidence of leukemia and thyroid cancer was also reported in the Taiwan case.17
There has been much debate regarding the cancer risk of low dose radiation exposure below 100 mSv, because of the scarcity of epidemiological data. Recent studies on occupationally exposed group have provided strong scientific evidence supporting the linear no-threshold model (LNT) of cancer risk, even at low level of external, protracted, or cumulative exposure of ionizing radiation (mean bone marrow dose 1.1 mGy per year; median cumulative colon dose 4.1 mGy).1819 The results of the present study showed no significant association between the self-reported cancers with the estimated cumulative radiation dose. Based on the LNT, the total required for a study regarding an exposure level of less than 10 mSv is more than 107,20 a figure far larger than that used in the present study (about 104).
In the present study, the comparison of cancer incidence among neighboring regions showed an increase of all cancers in men, however, the results should be interpreted cautiously. Due to the ecological design of the comparison, the finding cannot be interpreted as a causal association and is vulnerable to the ecological fallacy. Furthermore, considering the fact that cancer occurrence is followed by at least 2–5 years (for leukemia) or 5–10 years (for solid cancer) after radiation exposure, the ascertainment of cancer occurrence for 2000–2008 in the present study is not sufficient and the follow-up period needs to be extended in the future.
Although currently it has been suggested the threshold level of radiation exposure dose related with cardiovascular disease might be lower than estimated previously,21 non-cancer diseases, the ‘deterministic health effect,’ is known to exist within certain threshold exposure doses.22 Therefore, it is difficult to interpret the significant association between self-reported hypertension and hyperlipidemia in females with estimated radiation dose in the present study. The reason might be due to unknown confounding effects that we could not consider, something with an unknown biological mechanism, reporting bias that could not be assessed in the cross-sectional design, or residual cofounding effect of age in which the higher exposed respondents have a higher age than the lower exposed respondents in the present study (Supplementary Table 2).
In a previous report, the effects of radiation from nuclear power plants are not limited to physical health problems alone, but also mental and societal effects.23 Mental health problems such as depression, anxiety, and post-traumatic stress disorder, particularly in mothers with young children and cleanup workers have been reported, after nuclear power plant explosions, and emotional consequences could occur independently of the actual radiation exposure received.24 The respondents in the present study were parents/guardians, mostly mothers of children aged ≤ 12 years. Results may therefore be reflective of the mothers' fears regarding the health consequences of radiation exposure. In the present study, the levels of anxiety and psychological stress increased concurrently with estimated radiation exposure. The differences observed between the present study and previous studies involving nuclear disasters may be due to the differences in conditions, i.e., the magnitude of the disaster, the degree of fear, and the time of survey as well. This study was conducted immediately after the media reported on the issue, while others were conducted many years after the accidents. Educational and psychosocial interventions might be needed to tackle the issue of the potentially high-risk population with mental health problems.
Understanding people's perception about risk is essential for well-intended policies.25 Risk perceptions were associated with the severity of psychological and medically unexplained physical symptoms in the Chernobyl Nuclear Power Plant accident.26 Risk perceptions depend on the levels of knowledge about the risk, perceived controllability against the risk, and the degree of fear of the risk.27 Socio-political factors such as power, status, alienation, and trust are strong determinants of people's perception and acceptance of risk.28 Fortunately, the degree of fear of the radionuclide-contaminated roads was not very high among residents in the study region. The characteristics of perceived risk were consistent with those of previous studies, i.e., higher perception level was found in the less educated, in older adults, and in females. Health examinations for the highly exposed group, community environmental management, and long-term epidemiological monitoring were indicated in order by the survey participants as the prior governmental tasks for the community. Along with this, the findings on risk perception can provide a scientific basis for efficient risk communication and good policies.
This study had some limitations worth considering, which could have affected the outcome of the results. First, we could not trace workers who participated in the construction of the roads. Although the source of the 137Cs contamination could not be determined, it is possible that the construction workers might have had high internal and external exposure to the radionuclide. Secondly, we could not enroll a sufficient number of young children less than 5 years old who are more susceptible to ionizing radiation exposure. However, the number of children at the elementary schools was 59.5% of the total population of Wolgye 2-dong, which provided us the opportunity to investigate a susceptible group of children. Third, we could not eliminate bias related to a misrepresentation of the previous medical history, as this information was self-reported. It is not possible to disentangle the effects of radiation exposure per se from those due to elevated concern among people living for a long time or close to the road. It is not possible to know whether self-reported information biased differentially between comparison groups in the present study. In addition, we could not use the cancer registry data to identify incident cancer objectively among questionnaire responders in the present study because the privacy protection act prohibited gathering personal identifiable information and no other alternative acts went into effect to allow it for the public benefit at that time. Finally, we did not include information regarding pregnancy in women in the study, therefore, we were not able to assess health risks for the developing fetuses. Instead, we analyzed the health risk in comparison with children born in the study region and in other places and found no difference.
In conclusion, there was no evidence of health problems in residents in association with radiation exposure from the 137Cs contaminated roads whereas increased anxiety level and decreased psychosocial wellbeing was found. As future recommendations, we suggest long-term epidemiological monitoring on cancer occurrence using the data surveillance method. Provision of a selective health examination of residents living close to the contaminated roads as part of a health promotion program would also be beneficial. Most importantly, it is recommended that a governing section for environmental health within the local government and public health center be established, to foster long-term management of the environment and effective communication with residents.
 XML Download
XML Download