

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Systemic anticancer chemotherapy is known to damage various organs, including the bone marrow, gastrointestinal (GI) tract, liver, kidney, and heart. However, ocular toxicity of chemotherapeutic agents is relatively uncommon. Because of the frequency of other life-threatening adverse effects and the priority assigned to them, ophthalmologic complications associated with chemotherapeutic agents are often underestimated and neglected.12 Nevertheless, vision deterioration can significantly affect the quality of life. Moreover, recent developments in chemotherapy have enabled prolonged survival; hence, chronic toxicities with long latency periods may become more evident.
Anterior segment abnormalities such as subconjunctival hemorrhage can be diagnosed by simple physical examination. However, the diagnosis of retinal damage requires special ophthalmologic examination owing to the location of the retina. Although the retina is protected from systemic drugs by the inner and outer blood-retinal barriers, the association between several retinal diseases and anticancer agents has been identified.34 Tamoxifen retinopathy is a type of retinal toxicity that exhibits unique clinical features.5 Paclitaxel and docetaxel therapy could induce cystoid macular edema (CME).6 New systemic anticancer treatments, including targeted biological agents, may not only offer promising antitumor activity but also produce novel adverse effects in the retina. McCannel et al.7 reported a series of bilateral serous retinal detachments (RDs) associated with the mitogen-activated protein kinase kinase (MEK) inhibitor treatment. Wolf et al.8 also reported a case of vemurafenib-induced severe uveitis. Hence, recent clinical trials of biological agents have also included a screening program in the ophthalmologic department.
Despite these concerns, only few studies have assessed the uveoretinal adverse effects of systemic chemotherapy. Most of the information from systemic reviews of the ocular effects of anticancer agents has been limited to the listing of rare presentations from case reports.1234 Considering the increasing number of cancer patients and the widespread use of chemotherapy, integrated data, including the frequency and severity of retinal toxicities, are essential. In the present study, we aimed to assess the incidence, clinical features, and outcomes of a series of uveoretinal adverse effects of anticancer chemotherapeutic agents, including traditional cytotoxic drugs and advanced targeted agents. We also investigated the changing patterns of uveoretinal toxicities based on the type of chemotherapy administered with time.
METHODS
In the present study, we selected patients who received systemic chemotherapy and presented to the ophthalmologic department of Asan Medical Center between July 2005 and June 2015. Patients diagnosed with uveoretinal diseases such as uveitis, macular disease, and retinal vascular disease were identified by analyzing the diagnosis code. The following International Statistical Classification of Diseases and Related Health Problems 10th revision (ICD-10) codes were used: scleritis H15.0, H15.9, and H19.0; uveitis H20.x; other disorders of the iris and ciliary body H21.x and H22.x; chorioretinal disorders H30.x to H32.x; RD H33.x; Retinal vascular occlusions H34.x; other retinal disorders H35.x to H36.x; and vitreous hemorrhage or opacity H43.1, H43.3, H43.8, H43.9, and H45.0.
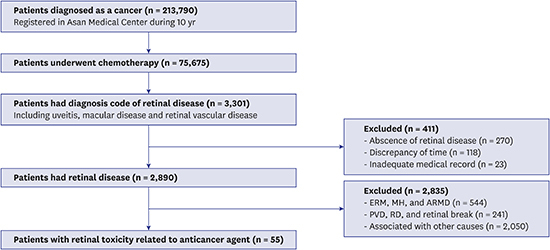
We excluded cases of retinal disease that may have been affected by other factors such as metastases to the eye or central nervous system, retinal issues related to thrombocytopenia, or ocular infection because of immunosuppression. Cases of diabetic, hypertensive, or radiation retinopathies and cancer-related retinopathies were also excluded for the same reasons. In addition, we excluded patients with typical risk factors, such as central serous chorioretinopathy during corticosteroid therapy, noninfectious uveitis in autoimmune disease, and retinal vascular occlusions associated with hypertension, diabetes, or old age (≥ 70 years).9 Cases of epiretinal membrane (ERM), macular holes (MHs), and age-related macular degeneration (ARMD) were excluded from this study because of the uncertain onset of these chronic diseases. Cases of posterior vitreous detachment (PVD), RD, and peripheral retinal degeneration including retinal break also excluded because the mechanical properties of these disease (Fig. 1).
 | Fig. 1Flow diagram of the patient selection process and inclusion and exclusion criteria.
ERM = epiretinal membrane, MH = macular hole, ARMD = age-related macular degeneration, PVD = posterior vitreous detachment, RD = retinal detachment.
|
Data, including age, sex, cancer type, distant metastasis, chemotherapeutic agents, route of first visit to the ophthalmologic department, ophthalmologic symptoms, duration between the first use of anticancer agents and ophthalmic presentation, ophthalmologic diagnosis, bilaterality, ophthalmologic feature, and prognosis, were collected. We assumed that all chemotherapeutic agents were administered in accordance with an acceptable dosing regimen. In general, the patients had been treated using multiple chemotherapeutic agents according to the schedule of their own combination therapy regimens. However, we strictly assessed only those agents that were administered at the time of ophthalmologic diagnosis, because past medicine could reduce the validity of a possible causal relationship between chemotherapy and ophthalmic disease.
We sorted the patients into 2 groups based on the chemotherapeutic agent exposure time and final visual outcome, respectively. First, we categorized the patients into 2 groups based on the median date of first exposure to the chemotherapeutic agent, because novel anticancer treatments could produce new uveoretinal toxicities that are different from those associated with traditional anticancer drugs. Second, we categorized the patients according to the final visual outcome (visual acuity [VA] < 20/40 Snellen or 0.5 Decimal at the last visit). These data were analyzed to determine the possible correlations between the final visual outcome and several factors such as age, sex, combination therapy, and metastasis. The Mann-Whitney U test or χ2 test was performed to evaluate the mean or proportional difference, and P values < 0.05 were considered statistically significant. Finally, we also examined the incidence of each cancer type and the frequency of use of each chemotherapeutic agent at our center over 10 years.
RESULTS
A total of 213,790 patients were diagnosed with malignant cancer during the 10-year study period at our center of which 75,675 patients underwent systemic chemotherapy including hormonal therapy. Among these patients, 35,149 (46.4%) were females. Breast cancer was the most common type of cancer (13,116 patients; 17.3%), followed by colorectal cancer (9,784 patients; 12.9%), gastric cancer (8,801 patients; 11.6%), hepatocellular carcinoma (8,124 patients; 10.7%), lung cancer (5,929 patients; 7.8%), and others. Cisplatin (27,935 patients; 36.9%) was the most frequently prescribed chemotherapeutic agent over the 10-year period. We enrolled and thoroughly reviewed 3,301 patients who were diagnosed with uveoretinal disease, including uveitis, macular disease, and retinal vascular disease during chemotherapy using ICD-10 diagnosis codes. Of these patients, 270 did not have any uveoretinal disease (miscoded); 118 had uveoretinal disease before chemotherapy (discrepancy of time); 23 had inadequate medical record; 544 had ERM, MHs, and ARMD; and 241 had PVD, peripheral degeneration, retinal tear, and rhegmatogenous RD. We excluded 2,050 patients because they had retinal diseases related to certain systemic conditions, such as diabetic retinopathy (n = 986), hemorrhage in coagulopathy (n = 149), vascular occlusion in hypertensive patients (n = 106), uveitis with autoimmune disease (n = 53), hypertensive retinopathy (n = 51), infectious uveitis (n = 48), ocular metastasis (n = 44), central serous chorioretinopathy associated with systemic steroids (n = 38), and others (Fig. 1).
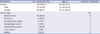
Finally, 55 eligible patients were enrolled over the study period including 38 (69.1%) females and 17 (30.9%) males. The age of the patients was 24–69 years (median, 58 years): 21–40 years for 7 (12.7%) patients, 41–50 years for 16 (29.1%) patients, 51–60 years for 22 (40.0%), and ≥ 61 years in 10 (18.2%). Breast cancer was the most common type of cancer (36.4%), followed by hepatocellular carcinoma (18.2%), GI cancer (14.5%), and hematologic malignancy (10.9%). Systemic metastases were observed in 20 patients (36.4%; Table 1).
Table 1
Patient demographics and oncologic characteristics
![]()
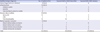
Bilateral involvement was noted in 16 (29.1%) patients. The most common uveoretinal adverse effects were noninfectious anterior uveitis (21.8%), followed by serous RD (18.2%), tamoxifen retinopathy (18.2%), retinal vascular occlusion (16.4%), and retinal or vitreous hemorrhage (16.4%). Among patients exposed to anticancer agents before 2009, tamoxifen retinopathy (35.7%) was the most common finding. In contrast, among patients exposed after 2010, retinal vascular occlusions (25.9%) and uveitis (25.9%) were the most common complications, followed by retinal hemorrhage (22.2%; Table 2). A total of 44 patients (80.0%) had ophthalmologic symptoms, such as blurred vision (50.9%), red eye (14.5%), floaters (9.1%), and metamorphopsia (5.5%). Other patients (20.0%) were identified by an adventitious retinal exam, such as tamoxifen retinopathy screening (Fig. 2). Thirty-seven (67.3%) patients presented to the outpatient department, 16 (29.1%) patients underwent an ophthalmologic consultation during hospitalization for systemic chemotherapy, and 2 (3.6%) patients with branch retinal artery occlusion and posterior uveitis presented to the emergency department (Fig. 2).
Table 2
Retinal adverse effects according to the time of first exposure
![]()

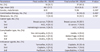
Monotherapy was administered to 36 (65.5%) patients and combination therapy using ≥ 2 agents was administered to 19 (34.5%) patients. Cisplatin (21.8%) was the most frequently used drug, followed by tamoxifen (16.7%) and paclitaxel (7.7%; Table 3). Tamoxifen (38.2%) and cisplatin (26.5%) were the most common chemotherapeutic agents associated with uveoretinal complication before 2009. Cisplatin (18.2%) was the most common agent after 2010, followed by paclitaxel (11.4%; Supplementary Table 1). Daunorubicin, cytarabine, tamoxifen, toremifene, and imatinib were found to be associated with uveoretinal complications more frequently than other agents (Table 3 and Supplementary Table 2). The median duration between the first use of anticancer agents and ophthalmologic presentation was 208.5 days (6.8 months; range, 19–5,945 days). Intraocular hemorrhage, vascular obstruction, and serous RD generally occurred within the initial 6 months of chemotherapy, whereas CME and tamoxifen retinopathy occurred later. Inflammatory disease generally developed within 12 months. Most patients with tamoxifen retinopathy presented after 24 months (Fig. 3). Final snellen VA < 20/40 (decimal 0.5) was observed in 18 (32.7%) patients (Table 4). The relationship between low final VA and systemic complications of chemotherapy, age, sex, combination therapy, and metastasis was not significant. Tamoxifen retinopathy (33.3%) and retinal vascular occlusion (27.8%) were more common in the group with final VA < 20/40.
Table 3
Anticancer agents used in patients who presented with retinal adverse effects

Only agents that had ≥ 2 related cases are displayed (Supplementary Table 2).
Vas occlusion = vascular occlusion, RD = retinal detachment, Tmx retinopathy = tamoxifen retinopathy, CME = cystoid macular edema.
![]()
 | Fig. 3Duration between the first use of anticancer agents and ophthalmologic diagnosis.
Vas = vascular, CME = cystoid macular edema, RD = retinal detachment, Tmx retinopathy = tamoxifen retinopathy.
|
Table 4
Comparison of clinical characteristics according to final VA
VA = visual acuity, SD = standard deviation, HCC = hepatocellular carcinoma, GI = gastrointestinal, Tmx retinopathy = tamoxifen retinopathy, Vas = vascular, RD = retinal detachment.
aP value was obtained by Mann-Whitney U test; bχ2 test.
![]()
All 3 patients who had been treated with cytarabine and daunorubicin developed anterior uveitis. Two patients treated with letrozole manifested minor retinal hemorrhage (Supplementary Fig. 1). The 3 patients diagnosed with retinal artery occlusion had been treated with cisplatin (Supplementary Fig. 2), and the 2 patients with branch retinal vein occlusion had been treated with hormonal agents. The 3 patients with idiopathic central macular edema had been treated with mitotic agents (Supplementary Fig. 3). Among the patients with serous RD, 2 had been treated with tamoxifen and 2 with imatinib. All 10 patients with tamoxifen maculopathy showed various degrees of pseudo-cystic cavitation in the fovea, which was proved using optical coherence tomography scans (Supplementary Fig. 4). Two of these patients required vitrectomy because retinal disruption had progressed to a full-thickness MH. The median duration from initiation of tamoxifen to the diagnosis of retinopathy was 62.5 months (5.2 years). Among the 10 patients treated with biological targeting agents, noninfectious anterior uveitis was the most common adverse event (40.0%; Supplementary Fig. 5), followed by serous RD (30.0%).
DISCUSSION
In the present study, we described our 10-year experience with uveoretinal adverse effects of systemic anticancer chemotherapy at a single center, which is the largest referral hospital in Korea. We found that uveoretinal damage was the most common adverse effect of chemotherapeutic agents. Patients were predominately female. Toxicity was averagely developed in sixth decade of life. One thirds of patients had breast cancer. These epidemiological features of complicated patients differed from those of all patients who underwent chemotherapy at our hospital for 10 years. These discrepancies may be associated with the high incidence of tamoxifen retinopathy among retinal adverse effects.
The most common adverse effects noted in the present study include noninfectious uveitis. Anterior uveitis was predominantly noted, which usually be resolved using conservative treatment such as corticosteroid eye drops. However, a severe case may produce a structural damage including posterior synechiae, and may necessitate the cessation of the causative agent. We observed 3 cases of uveitis during cytarabine and daunorubicin treatment for acute myeloid leukemia. Although leukemia could manifest as uveitis, the absence of posterior segment involvement and lagging onset of uveitis (after the primary disease is controlled) decreases the probability of malignant intraocular involvement in these cases. Although keratoconjunctivitis is relatively common in patients undergoing cytarabine treatment,3 anterior uveitis has also been reported in several cases.1011 This emphasizes the importance of careful monitoring of patients who develop red eye or complain about reduced vision during cytarabine chemotherapy.
Posterior uveitis is rare, but it may lead to serious visual impairment and remnant sequelae. In the present, both the patients with posterior uveitis were treated with biological targeted agents. Vemurafenib is a BRAF kinase inhibitor, whereas sorafenib is a tyrosine kinase inhibitor that targets RAF and other receptor kinases. Although most cases of uveitis induced by vemurafenib have been managed when chemotherapy was ongoing,12 severe panuveitis has also been reported.8 The authors speculated that uveitis may involve an immunological cross-reaction of antigens in the uvea. To our knowledge, there have been no reports on the association of posterior uveitis with sorafenib. However, cutaneous vasculitis has described in several reports of sorafenib treatment with a hypothesis which states that apoptosis may be induced in endothelial cells because of direct antivascular endothelial growth factor receptor or anti-platelet-derived growth factor receptor effects.1314
Retinal vascular occlusion related to alkylating agents, particularly cisplatin and oxaliplatin, is most likely to occur via a vaso-occlusive mechanism.1516 Cisplatin is known to increase platelet reactivity.17 However, in the present study, we found that vascular occlusion also increased in the next 5-year-group despite the lack of change in the cisplatin prescription. This was partially attributed to the development of hormonal agents, which could increase the risk of the thrombosis. The occurrence of retinal vein occlusion after long-term tamoxifen use has also been reported.1819 Because retinal or vitreous hemorrhage may be caused by the release of blood cells from the vascular cavity due to occlusion of the small arteriole, venule, or capillary, it may fit into the huge category of vascular occlusion conditions in a broad sense. Eisner et al.20 observed patients who received aromatase inhibitor developed retinal hemorrhage at the posterior pole.
In the present study, we found that 2 patients receiving tamoxifen therapy had serous RD and pigment epithelial detachment. A recent study also reported a case of central serous RD associated with tamoxifen.21 Since tamoxifen has toxic effects on human retinal pigment epithelium and photoreceptor cells,2223 fluids can leak though the broken blood-retinal barrier and accumulate in the subretinal area.24 Multiple serous RDs related to binimetinib, which is an inhibitor of MEK, is another emerging complication in melanoma patients.25 However, we did not observe similar cases at our hospital owing to the low incidence of melanoma in non-Caucasian populations.
Although crystalline retinopathy is the best known ocular complication, tamoxifen toxicity can present as a diverse set of conditions, including macular edema, pseudo-cystic cavitation, MH, serous detachment, and vascular occlusion.518262728 In the present study, tamoxifen maculopathy, which manifested as a retinal cavitation in the fovea, was a common adverse effect, as a single condition caused by a single agent. Following recent marked developments in high-resolution optical coherence tomography scans, this maculopathy induced by low-dose tamoxifen could be visualized.282930 The dysfunction of Müller cells, which are glial cells that extend vertically throughout the retina, is believed to play a significant role in structural disruption of the retina.28
There were several limitations in the present study. Because the use of combination chemotherapy regimens make it difficult to attribute ocular toxicity to a particular drug, we only listed a single chemotherapeutic agent as the inciting agent despite the patient being treated with multidrug therapy. However, it is likely that other drugs may have caused sensitization of the retina to the reported side effect. Moreover, patients receiving chemotherapy for malignancies might also develop ocular problems for totally unrelated reasons. Although analysis of change relative to anticancer agent may be more meaningful than final VA, it was not available since most patients presented to ophthalmologic department after their symptom onset including visual impairment. However, uveoretinal complications might lead irreversible visual damage due to its low regenerative ability; thus, final visual outcome could reflect the visual effect of anticancer agents. As we excluded all patients with other suspected underlying diseases at the start of the study, the actual incidence of uveoretinal toxicity may be higher than that which is reported. Previous studies have indicated that decreased estrogen levels may be associated with the occurrence of ARMD and that some medications could aggravate diabetic macular edema.313233 Hence, further assessments should focus on chronic diseases, such as ARMD, or on the exacerbation of the underlying retinal problem.
Since ophthalmologic symptoms are often overlooked by physicians or patients themselves, we described the ocular toxicities of chemotherapeutic agents in order to assist oncologists who care for such patients. Although the present study had insufficient data to completely determine the frequency of uveoretinal complications, we demonstrated the relative incidence of each adverse effect and subsequently identified the agents that have higher potential for retinal toxicity. Thus, careful ophthalmologic examination by retinal specialists is recommended in patients who are or have been treated with multiple chemotherapeutic agents including cytarabine, daunorubicin, imatinib, toremifene, tamoxifen, and taxanes.
In conclusion, uveoretinal complications were mostly mild to moderate and exhibited a favorable response to conservative therapy. Nevertheless, a considerable number of patients exhibited significant loss of vision that was irreversible despite cessation of the causative chemotherapeutic agent. Oncologists and ophthalmologists should always consider the possibility of uveoretinal problems being associated with chemotherapeutic agents. Since there is no consensus or recommendation regarding routine ophthalmologic monitoring, prompt consultation with an ophthalmologist can lead to early detection, proper diagnosis, and appropriate treatment. Dose reduction or discontinuation of incriminated drugs may help to reduce the severity and duration of uveoretinal adverse effects.
 XML Download
XML Download