

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Kidney transplantation (KT) is the gold standard therapy for patients with end-stage renal disease (ESRD).1 However, there is continuous imbalance between the number of recipients on waiting list and the number of donors regardless of living or deceased. To overcome the organ shortage, ABO incompatible KT, KT across donor specific antibody (DSA) and kidney paired donation (KPD) have been tried.
ABO blood group incompatibility and the presence of pre-existing human leukocyte antigen (HLA)-DSA are major immunological barriers to living donor KT.23 Technical advances in both measure and removal antibodies have given chances to overcome these immunologic barriers. Moreover, there are currently several modalities with clinical efficacy and efficiency.456
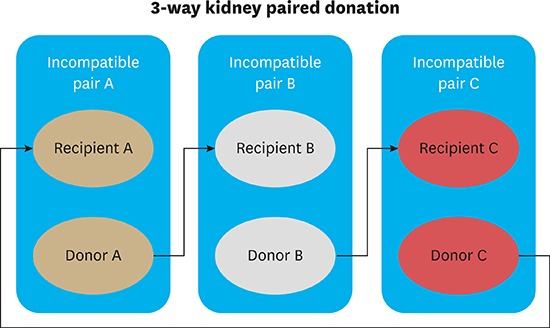
The concept of KPD was introduced by Rapaport in 19867 and was performed in 1991 for the first time in Korea.8 KPD enables incompatible living donor-recipient pairs to be matched with other pairs, leading to acceptable KTs for each recipient. KPD and desensitization are complementary methods to maximize the likelihood of living donor KT.291011
Here, we report our first successful 3-way KPD transplantation in a single center resulting in transplantation of highly sensitized recipients and ABO incompatible recipients.
Go to : 
CASE DESCRIPTION
Recipient 1 (R1) was a 44-year-old woman with ESRD secondary to biopsy proven IgA nephropathy. R1 had an ABO compatible willing living donor 1 (D1), her husband. She was difficult to match with broad HLA sensitization and hard to desensitize due to a high immunologic risk with positive anti-human globulin enhanced complement dependent cytotoxicity (AHG-CDC) cross-matches with the willing living donor and showed repeated positive AHG-CDC cross-matches with other donors. In addition, she showed multiple and high titer DSAs. Her waiting time for KT was 20 months.
Recipient 2 (R2) was a 59-year-old woman with ESRD due to unknown cause. R2 had blood type O and was ABO incompatible with her willing living donor 2 (D2) of blood type B, her husband. Moreover, she showed multiple and high titer DSAs. Her waiting time for KT was 48 months.
Recipient 3 (R3) was a 51-year-old man with ESRD secondary to biopsy proven diabetes mellitus nephropathy. R3 was difficult to match due to the blood type combination with willing living donor 3 (D3), his wife. He had an anti-tuberculosis medication 1 year ago for active tuberculosis so desensitization treatment was not considered. After 13 months of waiting, he underwent KT.
KPD matching rules in Samsung Medical Center
The matching rules for KPD were made according to the consensus of the transplantation surgeons, nephrologists, clinical pathologists, and the coordinators of Samsung Medical Center.
KPD rules and its priorities are as followings, so called three avoidings and three maximizings.
1. Avoiding matches with HLA positive cross-match
2. Avoiding matches with presences of HLA DSA
3. Avoiding matches with blood type incompatibility
4. Maximizing matches for recipients with low match probabilities (high panel reactive antibody [PRA])
5. Maximizing matches for the similar age group
6. Maximizing matches for recipients with lesser HLA mismatch
The 3-way KPD was performed on R1 with D3, R2 with D1, and R3 with D2 under our matching rules. Table 1 describes the pre-transplant characteristics of recipients and donors and Table 2 shows matching conditions of KPD transplantation.
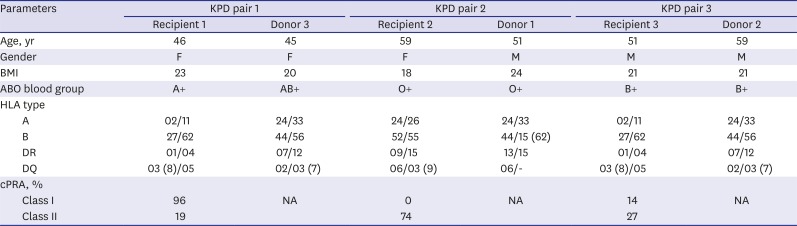
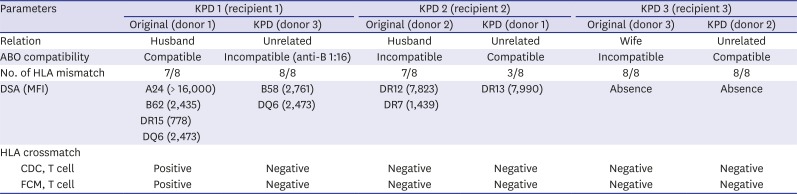
Table 1
The characteristics of KPD recipients and donors
KPD = kidney paired donation, BMI = body mass index, HLA = human leukocyte antigen, cPRA = calculated panel reactive antibody, NA = not available.
![]()
Table 2
Matching conditions of KPD transplantation for original and KPD pairs
KPD = kidney paired donation, DSA = donor specific antibody, MFI = median fluorescence intensity, HLA = human leukocyte antigen, CDC = complement-dependent cytotoxicity, FCM = flow cytometry.
![]()
R1 received KT from D3 in June 2014. She was ABO incompatible with KPD donor but her AHG-CDC and flow cytometry-crossmatches (FC-XM) against the donor in the exchange were negative. The number and strength of DSAs were decreased in compared with original condition. She began desensitization therapy with rituximab and plasmapheresis two weeks before transplantation. Initially her isohemagglutination titer for anti-B IgG was 1:32, and after taking 4 cycles of plasmapheresis, IgG titer of 1:2 was accomplished. R2 received ABO compatible KT from D1. Nevertheless, she still had a high strength DSA to DR13. She underwent desensitization therapy with rituximab 2 days prior to transplantation. R3 received an ABO compatible KT from D2. He did not have a DSA to D2; therefore, she did not need any desensitization therapy.
One transplantation team carried out three transplantations for two days.
All recipients showed immediately good graft function and normalization of serum creatinine (sCr) within days, and had stable graft function on discharge at 1 month after transplantation. Table 3 describes the laboratory findings of three KPD recipients.

Table 3
The outcome of KPD
KPD = kidney paired donation, KT = kidney transplantation, BUN = blood urea nitrogen, eGFR = estimated glomerular filtration rate.
![]()
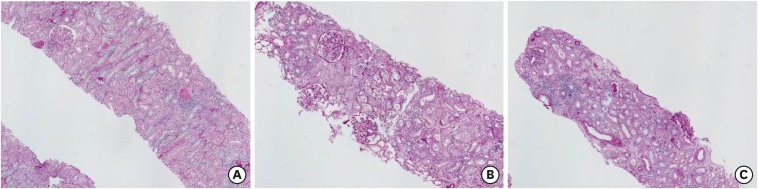
All recipients underwent protocol biopsy at two weeks after transplantation (Fig. 1). Pathologic findings for R1 and R2 showed normal appearances. However, biopsy for R3 revealed a finding of borderline acute cellular rejection. He was treated with methylprednisone-pulsed therapy. During the follow up period, R1 produced de novo DSA, anti-DR13 (median fluorescence intensity [MFI] 2,677) to D2 at 7 days after transplantation. Although the strength of preformed DSA, anti-B58 was slightly decreased from MFI 2,638 to 1,119. Eventually, both DSAs were not detected at 4 months after transplantation. R2 had a preformed DSA, anti-DR13 (MFI 7,990) to D3 and it has persisted at low level between MFI 2,000–3,000 until 10 months after transplantation.
After 1 year of follow up, R2 and R3 were tolerated with excellent graft function. However, R1 was presented with 3 times episodes of rejection managed with methylprednisone-pulsed therapy at 2 months, 4 months, and 6 months after transplantation. Eight months after transplantation, R1 was revealed to have BK nephritis on biopsy. The maintenance immune-suppression was changed to Sirolimus. During the follow up, sCr for R1 was slightly elevated between 2 and 3 mg/dL and estimated glomerular filtration rate (eGFR) was decreased between 20 to 30 mL/min. After 18 months of follow up, she was well with stable graft function.
Go to :
DISCUSSION
Currently there are three options available to patients who have an immunologically incompatible living donor: KPD, desensitization and a combination of the two options. KPD enables to match a potential kidney recipient who has a willing but incompatible donor to another incompatible pair.13
Desensitization could overcome the immunologic incompatibilities of donor-recipient pairs with ABO incompatibilities, DSAs, and even positive cross matches. Although it is still demanding technically and costly, some centers have provided comparable results to living donor KT.1014
Despite desensitization protocols or inclusion in a KPD registry, highly sensitized patients with multiple DSAs and high PRA remain difficult to undergo living KT. It is obvious that for these patients either strategy alone will not be able to find a suitable donor with no immunologic risk.
We describe the first experience of 3-way KPD with desensitization in Korea. The recipients were highly sensitized or ABO incompatible with their donors. With KPD and desensitization, they successfully underwent KTs. In this study, R1 suffered from 3 times episodes of rejection and BK nephritis after KPD with desensitization, however eventually she became to have stable graft function. Without combination of KPD and desensitization, she might not have a chance to live free from dialysis due to high immunologic risk with highly broad sensitization. With thorough analyzing immunologic condition of donor and recipient, this combination strategy of desensitization and KPD could enhance successful transplantation in highly sensitized patients.11
The success of KPD is greatly dependent on the size of pool and composition. Many studies reported potential matches could be increased with pool size.1516 However, there are several barriers to be overcome. There should be consensus between participating transplant centers on the allocation requirements and criteria. The participating centers may have different interests on KPD and they may cause not enough cooperation. Nowadays, national KPD programs have introduced rapidly including the United States, Canada, Australia, and the United Kingdom, and so on.17181920 Considering these factors, nationwide registry program is favored than multiple independent center based registries to enlarge the size of donor pool, especially in country with small population, like Korea. Decisions about the best transplantation option for the highly sensitized patient could now be made rationally using KPD and desensitization as complimentary options by more thoroughly identifying the immunologic risks and better understanding of the limitations of both KPD and desensitization. When determining which option is best for a matching, there are three important considerations. The first is the proper matching by selecting the best KPD rules based on the degree of sensitization, recipient blood type, donor blood type and the size of the KPD pool. The second is to facilitate the various desensitizing modalities available nowadays based on the immunologic risks of recipient and donor. The third is the full participation of kidney transplant centers. These considerations will estimate the likelihood of success of KPD for the matched pairs. The primary goal of KPD should be focused on not only facilitating immunologically compatible kidney transplants, but also comprising highly sensitized patients with least incompatible donors.
In this 3-way KPD with desensitization transplantation, we have showed that combination of desensitization and KPD has the potential that can increase living donor KTs with lower immunological risks and reasonable graft survivals.
Go to :
 XML Download
XML Download