

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Patients with prostate cancer (PCa) have extremely heterogeneous clinical courses, ranging from indolent and organ-confined to aggressive, metastatic, lethal diseases.123 Physicians often use risk stratification systems to determine the stage of cancer and design a proper treatment approach.4 At diagnosis, PCa is usually classified into major risk categories (low, intermediate, and high) based on tumor, node, and metastasis (TNM) clinical stage, biopsy Gleason score, and pretreatment prostate-specific antigen (PSA) levels. The most widely used risk classification systems are the D'Amico classification5 and the National Comprehensive Cancer Network (NCCN) risk classification6 that equally assign weights to any combination of these three factors, creating an extremely heterogeneous mix of patients within each of the three categories, particularly for those with intermediate-risk prostate cancer (IRPCa).7 Biochemical recurrence (BCR) rates following definitive primary treatment for IRPCa vary dramatically, with 5-year rates ranging from 2% to 70%.891011 This heterogeneity of clinical courses suggests that there are subsets of IRPCa patients with unfavorable prognoses. Zumsteg and colleagues7 recently proposed substratifying tools to classify patients as having unfavorable or favorable IRPCa using three clinical factors that are not included in the contemporary risk stratification system, such as primary Gleason pattern, percentage of positive biopsy cores, and the number of intermediate-risk factors. Given that different treatment options are recommended according to the risk stratification, there is a great need for reliable risk substratifying tools.
The University of California San Francisco (UCSF) Cancer of the Prostate Risk Assessment (CAPRA) score was developed to facilitate risk stratification.12 The CAPRA score is easily calculated from routinely collected clinical variables: PSA, biopsy Gleason score, age, clinical T stage, and percentage of positive biopsy cores.13 This prediction model has been extensively validated in the assessment of metastasis and mortality across multiple treatment modalities.1415161718 Interestingly, we recognized similarities between the substratifying tools adopted to use established criteria and pretreatment variables in the CAPRA score.719 The primary Gleason pattern, percentage of positive biopsy cores, and numbers of intermediate-risk factors (PSA level > 10 but ≤ 20 ng/mL, a biopsy Gleason score 7, or cT2b-c) were also employed to calculate the CAPRA score. Thus, we hypothesized that because the CAPRA score incorporates additional informative clinical variables it could be used to stratify intermediate-risk patients into different prognostic groups.
The present study aimed to assess the clinical applicability of the CAPRA score to subclassify patients with IRPCa into different prognostic groups. We examined the consistency between CAPRA score and established criteria and compared its ability to predict favorable pathology.
METHODS
Study population and surgery
We retrospectively reviewed the data of 1,086 PCa patients who underwent robot-assisted radical prostatectomy (RARP) performed by a single surgeon at Severance Hospital between January 2007 and December 2012. Among all RARP cases, 19.6% of patients met the criteria of IRPCa according to the D'Amico classification (clinical stage T2b, PSA levels between 10 and 20, or Gleason score of 7).5 After excluding patients who received neo-adjuvant treatment or adjuvant radiotherapy and those with missing variables, 203 subjects met inclusion criteria.
RARP was carried out using our standardized extraperitoneal technique.20 Clinical staging was assigned by the attending urologist according to the 2002 TNM system. Biopsy and pathological grading were performed according to the Gleason grading system, and Gleason scores were assigned by genitourinary pathologists.
Data collection and definition
Preoperative characteristics, including clinical stage, PSA, and prostate biopsy findings were calculated to determine the CAPRA/Cancer of the Prostate Risk Assessment Post-Surgical (CAPRA-S) score. Pathologic favorable IRPCa was defined as a Gleason score ≤ 6 and organ-confined stage at surgical pathology. BCR was defined as two consecutive PSA values ≥ 0.2 ng/mL at any time postoperatively or any additional treatment more than 6 months after RARP. The established criteria for unfavorable IRPCa were defined by criteria 1 (primary Gleason pattern of 4 or ≥ 2 intermediate-risk factors)19 and criteria 2 (criteria 1, and percentage of positive biopsy cores ≥ 50%).7
Statistical analysis
The CAPRA scores were calculated for a continuous sum score model (range, 0–10) and 3-group risk model as low (CAPRA 0 to 2), intermediate (CAPRA 3 to 5), and high (CAPRA 6 to 10). We compared the discriminating performance of CAPRA with established criteria for predicting pathologic outcome with receiver operating curve (ROC) analysis. The Kaplan-Meier method and the log-rank statistic were used to test for BCR free survival differences according to the CAPRA score. Hazard ratios for BCR following RARP were estimated using Cox proportional hazards regression analysis according to the CAPRA scores. Statistical significance was considered at P < 0.05 (two-sided tests). Statistical analysis was performed using SPSS 20.0 software (SPSS Inc., Chicago, IL, USA).
Ethics statement
The study was carried out in agreement with the applicable laws and regulations, good clinical practices, and ethical principles as described in the Declaration of Helsinki. The Institutional Review Board of the Severance Hospital approved the study protocol (Approval number: 4-2014-0619). The board exempted informed consent.
RESULTS
Baseline characteristics
Table 1 lists the baseline characteristics of the 203 IRPCa patients who met the inclusion criteria and underwent extraperitoneal RARP performed by a single surgeon. The median prebiopsy PSA and prostate-specific antigen density (PSAD) were 7.92 ng/mL and 0.27 ng/mL/g, respectively. Overall, 142 (70%) of IRPCa patients had a biopsy Gleason score of 7, and 65 patients had a primary Gleason pattern scored as 4. After RARP, about half of patients were confirmed to have organ-confined disease, and one-fourth of patients had a low-grade cancer (Gleason score ≤ 6). Overall, 38 (18.7%) patients had favorable pathologic features after RARP (Table 2).
Table 1
Baseline clinicopathologic characteristics

Table 2
Pathologic outcomes of RP
Discriminative ability between favorable and non-favorable pathology
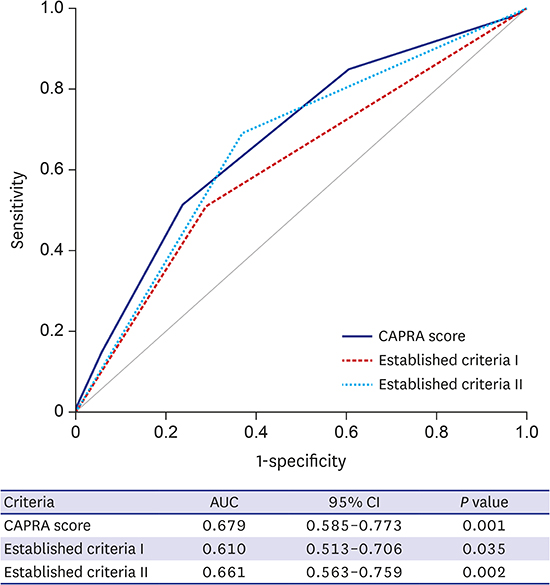
The distribution of the summed CAPRA scores for our cohort is listed in Table 3. The vast majority of patients (97.0%) had a CAPRA score from 2 to 6; only 1.0% had a score greater than 7, and none had a score greater than 8. The CAPRA score was well correlated with established criteria I and II (linear by linear association, P < 0.001). None of the patients who have a summed CAPRA score greater than 5 met the established criteria I and II for favorable IRPCa. The pathologic assessment of the summed CAPRA scores inversely correlated with favorable pathology (linear by linear association, P < 0.001) (Table 4). The areas under the ROC of discriminative ability between favorable and non-favorable pathology were 0.679 for CAPRA score and 0.610 and 0.661 for established criteria I and II, respectively (Fig. 1).
Table 3
Distribution of the data according to the CAPRA scores

Table 4
Relationships between CAPRA score and established classification criteria I and II, and final pathology in patients with IRPCa

Values are presented as number (%). P values were obtained by linear-by-linear association.
CAPRA = Cancer of the Prostate Risk Assessment, IRPCa = intermediate-risk prostate cancer.
Unfavorable disease was defined as aprimary Gleason pattern of 4 or ≥ 2 determinant of intermediate-risk factors at biopsy pathology; bcriteria I or percentage of positive biopsy cores ≥ 50%; cGleason score ≥ 7 or locally advanced disease at surgical pathology.
Fig. 1
Discriminative ability between favorable (Gleason score ≤ 6 and prostate-confined disease at surgical pathology) and non-favorable pathology in patients with IRPCa.
IRPCa = intermediate-risk prostate cancer, CAPRA = Cancer of the Prostate Risk Assessment, AUC = area under the receiver operating characteristics curve, CI = confidence interval.

Prediction of BCR after RARP
During a median follow-up of 37.8 (interquartile range, 24.6–60.2) months, 66 (32.5%) patients experienced BCR. There were significant differences with regard to BCR survival when categorized by 3-group risk model according to the CAPRA score (log-rank P < 0.001) (Fig. 2). In the continuous CAPRA sum score model, the hazard ratio of BCR per 1 group increase was 1.415 (95% confidence interval [CI], 1.185–1.691). The 3-group risk model also showed statistical significance in terms of BCR, the hazard ratios of a BCR within intermediate- and high-risk groups compare to low-risk group were 3.950 (95% CI, 1.210–12.891) and 7.524 (95% CI, 2.291–24.712), respectively (Table 5).
Fig. 2
Kaplan-Meier analysis of BCR-free survival categorized by 3-group risk model according to the CAPRA score in patients with IRPCa.
BCR = biochemical recurrence, IRPCa = intermediate-risk prostate cancer, CAPRA = Cancer of the Prostate Risk Assessment.

Table 5
Cox proportional hazards regression analysis for prediction of BCR after RP in patients with IRPCa

DISCUSSION
In this study, we assessed the clinical applicability of the CAPRA score for risk stratification of patients with contemporary IRPCa. The CAPRA scoring system showed comparable accuracy for pathologic outcomes compared to the established criteria, and was found to be a significant predictor of BCR as a continuous sum score model or 3-group risk model.
Clinical heterogeneity among intermediate- or high-risk patients defined by the traditional three-group risk stratification methods such as D'Amico and the NCCN 2012 classifications has been recognized in several studies.2122 The 5-year BCR rate following definitive primary treatment has been reported to range from 2% to 70% and 49% to 80% in intermediate- and high-risk PCas, respectively.232425 Reese and colleagues1 highlighted heterogeneous pathologic and biochemical outcomes among intermediate- and high-risk groups. Specifically, significant within-group heterogeneity was observed according to the number of intermediate- and high-risk criteria. We also observed heterogeneous pathologic outcomes and BCR rates among IRPCa patients who underwent RARP. Numerous studies have attempted to establish new stratification that can be used to identify subsets of patients with relatively better and worse prognoses. Additional clinical factors such as proportion of positive biopsy cores, pretreatment PSA density, number of intermediate- and high-risk criteria, and primary Gleason pattern have been included in pretreatment prognostic models.7262728
Recently, two valuable prognostic models were described to stratify and identify subsets of patients with IRPCa with relatively better and worse prognoses. Jung and colleagues19 defined the unfavorable intermediate-risk disease as a primary Gleason pattern of 4 or multiple intermediate-risk factors. Another established criterion for unfavorable intermediate-risk disease was developed by Zumsteg and colleagues7; they added a proportion of positive biopsy cores ≥ 50% to a previous criterion to identify patients with unfavorable intermediate-risk disease.
CAPRA is an easy-to-calculate risk score used to predict the preoperative probability of BCR-free survival after radical prostatectomy (RP); it was introduced by Cooperberg et al.1218 in 2005. The sum of the point values for the five variables (preoperative PSA, biopsy Gleason score, clinical TNM stage, percentage of positive biopsy, and age at diagnosis) yields a score from 0 to 10, with a higher value associated with an increased risk of recurrence.13 This prognostic instrument has been extensively validated with regard to biochemical progression, local recurrence, distant metastasis, and prostate-cancer-specific mortality across multiple treatment modalities, but its within-group discrimination power has not been previously investigated. We found that CAPRA scores correlated well with both established criteria. Moreover, the pathologic outcomes of the summed CAPRA scores demonstrated an inverse correlation with favorable pathology.
The present study had a potential limitation. Any retrospective analysis of surgical patients will be fraught with selection bias. It only included cohort from a single tertiary institution and a single surgeon series. Thus, larger multicenter studies are needed to confirm the applicability of the CAPRA score for risk discrimination among contemporary IRPCa patients.
In conclusion, CAPRA score is a simple preoperative tool that can be readily applied in clinical practice to help risk-stratify heterogeneous IRPCa patients into different prognostic groups with regard to therapy planning and counseling.
 XML Download
XML Download