

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic thromboembolic pulmonary hypertension (CTEPH) is a rare disease thought to be caused by an unresolved pulmonary embolism and its subsequent transformation into fibrous tissue, resulting in chronic occlusion of pulmonary arteries and pulmonary hypertension.12 Traditionally, the treatment of choice for CTEPH is pulmonary endarterectomy (PEA).34 However, not all patients are eligible for PEA — in fact, it has been reported that no more than 60% of patients with CTEPH can undergo PEA due to the location of lesions and comorbid conditions.5 Furthermore, of those who have undergone the surgery, 17%–31% experience recurrence or persistence of pulmonary hypertension.6 Recently, balloon pulmonary angioplasty (BPA) has arisen as a promising alternative treatment strategy for CTEPH patients with inoperability or recurrence of pulmonary hypertension after PEA, and previous studies from Japan and Europe showed favorable results with regard to hemodynamics,78 right ventricular function and exercise capacity,91011 quality of life,12 and respiratory function13 in CTEPH patients after BPA. However, there have been no prior studies on the efficacy and safety of BPA in CTEPH patients from Korea. Therefore, we sought to compare clinical and hemodynamic parameters at the baseline and last BPA session in CTEPH patients who were inoperable or who experienced recurrence or persistent pulmonary hypertension after PEA.
METHODS
Study population
The present study was single center, observational study of CTEPH patients who received BPA between December 2015 and April 2017 at Samsung Medical Center. We screened patients with suspected CTEPH based on a detailed medical history, a chest computed tomography scan, transthoracic echocardiography, lung ventilation-perfusion scintigraphy and right heart catheterization, and confirmed CTEPH by angiographic demonstration of multiple stenosis and obstruction of bilateral pulmonary arteries. A total of 15 CTEPH patients who received 52 sessions of BPA were finally eligible for this study. The following information was collected retrospectively through medical record review: age, gender, underlying comorbidities, laboratory findings, medications, hemodynamics, echocardiographic parameters, and BPA-related data. The time from the onset of symptoms to the first session of BPA and, if the patient had PEA before, from the time of PEA to the first BPA session, was calculated.
Clinical assessment
All patients underwent pre-specified examinations at baseline, 4 weeks, 24 weeks, and annually after the first BPA session according to the CTEPH prospective registry at the Samsung Medical Center. Assessment included the World Health Organization (WHO) functional class, N-terminal-pro-brain natriuretic peptide (NT-proBNP) levels, 6-minute walk distance (6MWD), pulmonary function testing, including the lung diffusion capacity for carbon monoxide, chest computed tomography scan, transthoracic echocardiography, lung ventilation-perfusion scintigraphy, and right heart catheterization. Hemodynamic parameters by right heart catheterization included pulmonary arterial wedge pressure, mean pulmonary arterial pressure (PAP), right atrial pressure, cardiac output, cardiac index (CI), pulmonary vascular resistance (PVR), and mixed-venous oxygen saturation. Transthoracic echocardiography included right ventricular systolic pressure, tricuspid annular plane systolic excursion (TAPSE), peak systolic annular velocity, right ventricular basal diameter, and right ventricular fractional area change. Every disease-related and hemodynamic parameter which was recorded at the last BPA session were defined as “post-BPA” data and used for further comparison.
BPA
Results of every BPA session were recorded according to our routine report form, including the number of BPA sessions for each patient, the number of vessels dilated in each session, and the amount of contrast and radiation used. All patients undergoing BPA received written information regarding the procedure and provided informed consent. The BPA procedure was carried out by two interventional cardiologists. Oral anticoagulation was maintained throughout the duration of the hospital stay. Firstly, we placed a 9F indwelling sheath (Radifocus® Introducer; Terumo, Tokyo, Japan) into a mainly femoral vein and a 7F long sheath (Flexor® Check-Flo Introducer; Cook Medical, Bloomington, IN, USA) was brought into the main pulmonary artery via a 9F sheath. We selected a branch of the pulmonary artery using an appropriate 6F guiding catheter and performed angiography. Unfractionated heparin was additionally infused after introduction of the guiding catheter according to the activated clotting time. A 0.014-inch wire (Runthrough NS Extra Floppy Coronary Guidewire; Terumo) was crossed to the targeted lesion, and then the lesion was dilated using balloon catheters of the appropriate size (Coyote 1.5 to 4.0 × 20 mm; Boston Scientific, Marlborough, MA, USA). The balloon was inflated by hand until the indentation disappeared or until the balloon was fully expanded. If the vessel was to be dilated for the first time, a small-sized balloon was used regardless of reference diameter of the segmental artery to prevent procedure related complications such as reperfusion edema, vascular rupture or vascular dissection, and a slightly bigger balloon was used in the subsequent session. After inflation, angiography was performed to confirm sufficient dilation and the presence of ruptured vessels (Fig. 1). Dilatation was repeated if it was deemed insufficient. A second session of BPA was done within seven days of the first BPA session. We performed two additional sessions of BPA if patients were symptomatic or had a mean pulmonary artery pressure greater than 30 mmHg at 4th week follow-up. At the 24th week follow-up, patients also underwent two additional sessions of BPA if mean pulmonary artery pressure was over 30 mmHg or if they complained of dyspnea, New York Heart Association (NYHA) functional class II or greater. After BPA, each patient was transferred to the cardiac intensive care unit to monitor vital signs and potential complications for at least 24 hours.
 | Fig. 1Selective pulmonary angiography before and after BPA. (A) Subtotal occlusion seen in the lateral basal segmental artery of the left lower lobe before BPA (arrow), (B) after ballooning, selective angiography shows good blood flow to the peripheral arteries, and (C) an improvement in parenchymal perfusion with excellent run-off in the venous phase (arrowheads).
BPA = balloon pulmonary angioplasty.
|
Statistical analysis
Results are presented as the mean ± standard deviation or median with interquartile range. Baseline characteristics between patients with history of PEA and those without PEA history were compared using Fisher's exact test or Mann-Whitney U test. Comparisons between baseline and post-BPA data were conducted with paired t-tests or Wilcoxon signed-rank tests. Statistical analyses were performed using PASW Statistics version 18 (IBM Co., Armonk, NY, USA). All tests were two-tailed, and P < 0.05 was considered statistically significant.
RESULTS
Study population
Baseline characteristics are presented in Table 1. Seven patients (46.7%) were female and the mean age of patients at the time of diagnosis was 53 years old. The severity of dyspnea was somewhat evenly distributed at the time of diagnosis, with class II being the most common (40.0%). Thrombophilic conditions were diagnosed in 3 patients (20.0%); these diagnoses included antiphospholipid syndrome, protein S deficiency, and antithrombin III deficiency. Six patients (40.0%) had a history of PEA. The other nine patients did not undergo this surgery due to distal inaccessible lesions (n = 5), poor general condition (n = 2), and refusal (n = 1). One patient initially presented with a cardiac arrest due to acute pulmonary thromboembolism with underlying CTEPH, and went through embolectomy rather than PEA. Reviewing the medications, 9 patients (60.0%) were prescribed sildenafil or macitentan. All patients were on anticoagulants, with warfarin being most common prescription (n = 9, 60.0%), and rivaroxaban being second most common (n = 4, 26.7%). The other medications included edoxaban and apixaban. Comparison between the group of patients with history of PEA and the group without history of PEA showed that the former group had significantly higher percentage of older patients, with significantly less estimated glomerular filtration rate, albeit within normal range.
Table 1
Baseline characteristics of patients with or without PEA history

Values are presented as mean ± standard deviation, number (%), or median (interquartile range).
PEA = pulmonary endarterectomy, NYHA = New York Heart Association, BPA = balloon pulmonary angioplasty, eGFR = estimated glomerular filtration rate.
aAt the initial diagnosis.
![]()
Hemodynamic and clinical outcomes
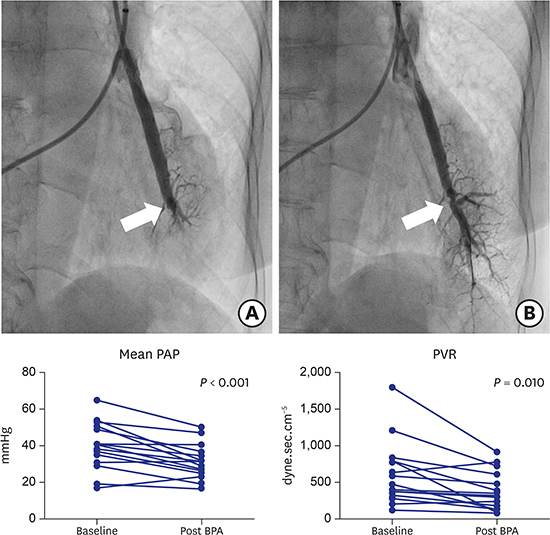
Each patient went through an average of 3.47 sessions of BPA, with 5.27 vessels dilated for each session on average. The mean number of segments treated was 11.07 (5.13 in the left lung and 5.93 in the right lung). Treatment goal was reached within the study period for seven patients. The other patients have been scheduled for additional BPAs in the near future except for three patients (one patient refused further invasive treatment due to complete resolution of subjective symptoms, and two patients were lost to follow-up). Comparisons between baseline and post-BPA data showed improvements in several disease-related and hemodynamic parameters (Table 2). Dyspnea severity and NT-proBNP levels significantly improved; all but three patients reported their dyspnea symptoms as having lessened, reflected in a definitive decrease in NYHA functional class. 6MWD was also significantly improved. Among the hemodynamic parameters, mean PAP, PVR, and right atrial pressure showed significant improvement, while CI did not (Fig. 2). Other parameters with significant changes included the right ventricular systolic pressure, TAPSE, mixed venous saturation, and arterial oxygen saturation. The overall rate of BPA-related complications was low; there were six sessions (11.5%) after which complications were recorded. Complications included vascular dissection (n = 3), hemoptysis (n = 1), and reperfusion injury (n = 2). Both patients with reperfusion injury were infused with a three-day course of high-dose methylprednisolone, after which their condition normalized. None of the patients required a mechanical ventilator or extracorporeal membrane oxygenation.
Table 2
Clinical and hemodynamic data before and after BPA

Values are presented as mean ± standard deviation.
BPA = balloon pulmonary angioplasty, NYHA = New York Heart Association, 6MWD = 6-minute walk distance, NT-proBNP = N-terminal-pro-brain natriuretic peptide, PAP = pulmonary arterial pressure, CI = cardiac index, PVR = pulmonary vascular resistance, BPM = beats per minute, TAPSE = tricuspid annular plane systolic excursion.
![]()
 | Fig. 2Hemodynamic parameters before and after BPA. Significant improvement of mean (A) PAP, (B) PVR, and (C) 6MWD seen after BPA, but not in (D) CI.
BPA = balloon pulmonary angioplasty, PAP = pulmonary arterial pressure, PVR = pulmonary vascular resistance, 6MWD = 6-minute walk distance, CI = cardiac index.
|
DISCUSSION
This study is, to our knowledge, the first study regarding the efficacy and safety of BPA for CTEPH patients in Korea. Our findings showed that BPA resulted in improvements in clinical and hemodynamic outcomes, and procedure-related complication rates were acceptable. Therefore, BPA might be a safe and effective strategy for both inoperable CTEPH patients and patients with residual pulmonary hypertension after PEA.
Current guidelines state that PEA is the treatment of choice for CTEPH, which is a disease caused by incomplete thrombolysis of a pulmonary thromboembolism and subsequent fibrotic vascular obstruction, culminating in pulmonary hypertension and/or right ventricular dysfunction.3 If the patient is deemed technically inoperable, carries an unfavorable risk-benefit ratio for PEA, or suffers from persistent symptomatic pulmonary hypertension after PEA, interventional BPA may be considered (class IIb).3 Our study also abided by this guideline, and BPA resulted in improvements in several symptomatic parameters evaluated by NYHA functional class, 6MWD, and hemodynamic and echocardiographic assessment. Most of these data were concordant with the findings of previous studies on the efficacy of BPA in CTEPH patients conducted in Japan and Europe.891011121415 A significant increase in arterial and mixed venous oxygen saturation was also recorded in this study, which is consistent with a report by Tatebe et al.,16 who suggested it to be the result of decreased intrapulmonary shunt. Interestingly, although mean PAP, PVR, and right atrial pressure were significantly reduced, indicating decreased pressure overload on the right sided heart, CI did not show any significant change after BPA, in contrast to most previous studies reporting significant improvement in CI. There are several possible explanations for this discrepancy, although it remains unclear why there was no significant difference in CI between baseline and post-BPA in our patient population. In contrast to a median CI of 2.2 L/min/m2 at baseline and a follow-up duration of 2.2 ± 1.4 years after the final BPA session in a previous representative study by Mizoguchi et al.,17 our subjects' CI were mostly in a normal range, with a median CI of 2.94 L/min/m2 and a median follow-up of 9 months. The relatively short duration of our study might not be enough time to reflect the impact of BPA on CI. Another possible explanation is reduced sympathetic activity: the respiratory distress and emotional tension associated with the procedure may have been relieved after repeated BPA sessions, which might have reduced the heart rate, thus reducing CI. In fact, the heart rate at the last BPA session was decreased compared with that at baseline, although there was no statistically significant difference. Considering that sildenafil was stopped in six out of ten patients who were prescribed sildenafil, a change in medication might have negated the beneficial effect of BPA on CI. However, in our study, there was no significant difference in change of CI after BPA between the group of patients who discontinued sildenafil and the group of patients whose medication did not change (whether sildenafil was continued or no medication was prescribed from the beginning). Finally, ethnic differences between Asian and Western populations might be able to explain this phenomenon. Indeed, two reports from Japan did not show a significant reduction in CI after BPA.1116
In six sessions (11.5% of total sessions), we experienced complications during BPA and post-BPA management. Vascular dissection occurred during three sessions, all of which were asymptomatic and spontaneously resolved. Hemoptysis that cannot be attributed to reperfusion injury was found in one session, and was resolved with supportive care alone. Two sessions were complicated by reperfusion edema, both of which were successfully treated by a three-day course of methylprednisolone. This complication rate is lower than those of previous reports, particularly when considering that of reperfusion edema.171819 As most of the complications reported in previous studies originated from vascular injury caused by wires or balloons, we focused on refining the BPA techniques, such as using wires with a tip load of < 1 g, using undersized balloons, and limiting the number of dilated segments. We suspect that this practice strategy will result in low complication rates.
Our study has several limitations. First, the number of study subjects was small, mainly owing to the short experience of BPA in our center. The number of enrolled patients was not sufficient to infer definite conclusions from this study, but it may help in generating hypotheses on which further research may be based. Second, our study was conducted in a single-arm setting at a single institution. This fact may also limit the generalizability of our findings, which should be interpreted with caution. Finally, the effects of BPA on respiratory function and glycemic control, which has been examined in recent published studies,1316 cannot be identified because we did not involve pre-specified examinations in the CTEPH registry.
In conclusion, BPA might be a safe and effective method for both inoperable CTEPH patients and CTEPH patients with residual pulmonary hypertension after PEA. Further large-scale studies will be needed to confirm these findings.
 XML Download
XML Download