

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
One of the most important issues related to hospital safety is inpatient suicide. In the United States, inpatient suicide is the second most common sentinel event reported to the Joint Commission.1 Because inpatient suicide occurs in close proximity to medical staff, it is often considered a preventable accident. Thus, inpatient suicide can result in litigation, and the legal system tends to be strict about the responsibilities of the hospital in these cases.2 Additionally, inpatient suicide negatively impacts other patients and medical staff. News of suicides may cause other patients to become vulnerable to depression and anxiety.3 Medical staff may feel shock, fear, sadness, and guilt as a consequence of the suicide, and they may even feel that they are incompetent because they could not prevent the event.4 Thus, appropriate assessments and interventions that prevent inpatient suicide are needed for the safety of patients and favorable hospital environments. Although inpatient suicides occur more frequently in psychiatric units, suicides do occur in medical settings.5
These suicides also have devastating effects on patients, families, medical staff, and the hospital environment. Recent studies have suggested that suicides in medical settings and suicides in psychiatric units differ intrinsically. According to a review by Ballard et al.,5 patients who committed suicide in medical settings were typically older, more likely to be married and employed, and more likely to use certain methods of suicide compared with patients who committed suicide in psychiatric units.
The relationship between physical illness and suicide is well established. Several physical illnesses make patients more vulnerable to suicide. Patients with cancer, coronary heart disease,6 and central nervous system dysfunction78 are more likely to attempt or commit suicide. Other factors, such as pain,910 physical limitations,11 older age,12 financial problems, social isolation, and hopelessness1314 are also related to higher risks of suicide. In addition, depression is thought to facilitate the link between physical illness and suicide.6
Because suicides in medical settings have different and unique characteristics compared to suicides in psychiatric units, specific methods that assess suicide risk in medical settings are needed. Although a variety of suicide risk screening tools target patients with mental illnesses, few screening tools that are specialized for medical settings are available.
We aimed to develop a new screening tool that can be used to quickly assess suicide risk in a medical setting. We hypothesized that depression and hopelessness would be related to suicide ideation, and we were able to confirm the reliability and validity of the new screening tool based on the above factors.
METHODS
Gathering literature on suicidality
To develop the Suicide Risk Scale for Medical inpatients (SRSM), we examined existing scales for suicidal risk. Those scales included the modified SAD PERSONS Scale (MSPS),15 the Beck Scale for Suicide Ideation (BSI),16 and the Columbia Suicidality Severity Rating Scale (C-SSRS).17 After analysis of the contents of each scale, three Korean psychiatrists and one psychologist discussed the essential components of an SRSM. These components included factors known to affect suicidality. Based on the review of existing suicide risk scales, researchers included items related to depression, anxiety, hopelessness, previous suicidal idea, impulsivity, and illness perception in the screening questionnaire.
We examined different mental health scales that are known to assess each unique concept — depression/anxiety,18 hopelessness,19 previous suicidal idea,16 impulsivity,20 and illness perceptions,21 and tried to extract one or two representative questions for each factors. These scales are listed as follows.
Hospital Anxiety and Depression Scale (HADS)
The HADS was developed to assess patient's anxiety and depression briefly in primary hospital setting. It consists of 14 items, and each item is rated from 0–3. Seven of 14 items are related with anxiety, and the rest seven items are related with depression. The Korean version of this scale has shown high reliability.22
Beck Hopelessness Scale (BHS)
The BHS was developed to assess patient's hopelessness about the future. It consists of 20 items, and each item can be answered as yes-no statements. Potential final scores of the BHS are ranging from 0–20 and score above 15 is considered as severe state. The Korean version of this scale has shown high reliability.23
BSI
The BSI was developed to assess patient's ideation about suicide. It consists of 5 screening items and 21 self-rated items. All 21 self-rated items are scored on a three-point scale ranging from 0 to 2, but score of last two items is excluded from the total score. There is no specified cut-off score in BSI. Increasing scores reflect increasing suicide risk, and any positive response merits investigation.24 The Korean version of this test has shown high reliability.25
Barratt Impulsiveness Scale (BIS)
The BIS was developed to assess patient's impulsivity. It consists of 30 items that are scored to yield three factors (attentional, motor, and non-planning impulsiveness). Each item is rated from 1–4. The Korean version of this scale has shown high reliability.26
Brief Illness Perception Questionnaire (Brief IPQ)
The Brief IPQ is developed to briefly evaluate cognitive and emotional representations of illness.21 It consists of 9 items. Contents of the scale are concerned with cognitive representation, emotional representation, illness comprehensibility, and perceived cause of illness. Each item is rated from 0–10 except last item which ask patients to list the three most important causal factors of their own illness. This scale is not validated in Korean.
Preliminary survey for the collection of information about suicidality among non-psychiatric inward patients
A preliminary survey of 100 adult patients admitted to the general ward of Korea University Medical Center, Guro Hospital, was performed. Patients under 19 years old or patients admitted for treatment of psychiatric illness were excluded from the survey. All participants provided written informed consent. The survey played an important role in developing the questions that comprise the SRSM. This survey asked inpatients a series of open-ended questions (i.e., Have you thought about suicide in the past three months? If so, please write down what you thought at that time). Based on this survey, we also included pain perception in the SRSM.
Preliminary item selection
Discussions within a research team of three psychiatrists and a clinical psychologist led to selection of 12 questions/items that were included in the preliminary version of SRSM. Each item was representative of a suicide-related factor: depression/anxiety, hopelessness, previous suicidal ideation, impulsivity and illness perceptions. Three reverse-scoring items were included in the preliminary version of SRSM.
Main survey with the preliminary version of SRSM and other related scales
A total of 100 adult patients who were admitted to the general ward of Korea University Medical Center, Guro Hospital, participated in the survey. Patients who were under 19 years old or admitted for treatment of psychiatric illness were excluded from the survey. Patients who had participated in the preliminary survey previously were also excluded from the survey. All participants provided written informed consent. Trained psychologists evaluated participants using the preliminary version of the SRSM, along with questionnaires that are currently used to evaluate depression/anxiety (HADS), hopelessness (BHS), and previous suicidal ideation (BSI). Of the 100 total participants, 20 patients were asked to answer the preliminary version of SRSM again after two weeks.
Reliability and validity
Reliability was measured in terms of internal consistency using Cronbach's alpha coefficient. Exploratory factor analysis was performed to evaluate construct validity. Test-retest reliability was assessed using Pearson's correlation coefficient for 20 patient test and retest scores. Concurrent validity was assessed using Pearson's correlation coefficient of SRSM scores and scales currently used to detect depression/anxiety (HADS), hopelessness (BHS), and previous suicidal ideation (BSI). All statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) 22.0 (SPSS Inc., Chicago, IL, USA).
Comparison of mean score of SRSM according to different groups
We compared mean score of SRSM between two groups according to age, education level, marital status, employment status, and severity of medical illness, using independent sample t-test.
Calculating cut-off score
We calculated the optimal cut-off value of SRSM for screening suicide risk. Receiver operating characteristics (ROC) curve analysis was performed, reflecting sensitivity and 1-specificity of SRSM score, using a score of on the Korean version of BHS as a standard.
BHS was considered as the most appropriate standard in calculating cut-off score among available scales, because there is specific established score of suicide risk in BHS.19 Statistical analysis was performed using MedCalc software version 15.11.4 (MedCalc Software, Mariakerke, Belgium).
RESULTS
Participants
There were 67 men and 33 women included in this study. The mean age of all participants was 58.20 ± 15.04 years old. The number of participants aged 65 or older was 33, and the number of participants under the age of 65 was 67. With regards to education level, 79 participants achieved high school graduation or less, while 21 participants had some form of post-secondary education. Of the participants, 73 were married, and 27 were unmarried, divorced, or widowed. Thirty-nine of the participants were currently employed and 61 were unemployed. With regards to accompanying medical illness, we divided participants into two groups, severe disease group and mild disease group. In Korea, severe disease is classified in National Health Insurance Act (NHIA) which warrants specific financial support. According to NHIA of Korea, cancer, cerebrovascular disease, heart disease, chronic kidney disease, and many other chronic, intractable diseases are classified as severe disease. We used criteria in NHIA of Korea to classify severity of participant's medical illness. According to the criteria, 67 participants belonged to severe disease group and they had either cancer or chronic kidney disease, cerebrovascular disease, Crohn's disease. Other 33 participants were belonged to mild disease group and they had disease other than severe disease such as sinusitis, a non-severe fracture or a ureteral stone. The mean score of the preliminary version of SRSM was 7.34 ± 5.60. The HADS mean score was 15.12 ± 7.97, while the mean score of the anxiety subscale was 6.88 ± 4.24, and the mean score of the depression subscale was 8.24 ± 4.46. The BSI mean score was 1.75 ± 4.96, and the BHS mean score was 3.54 ± 5.24 (Table 1).
Table 1
Demographic data and scores of each scale

Values are presented as number of patients (%) or mean ± standard deviation.
SRSM = Suicide Risk Scale for Medical inpatients, HADS = Hospital Anxiety and Depression Scale, HADS-A = Anxiety subscale of Hospital Anxiety and Depression Scale, HADS-D = Depression subscale of Hospital Anxiety and Depression Scale, BSI = Beck Scale for Suicide Ideation, BHS = Beck Hopelessness Scale.
![]()
Construct validity and reliability
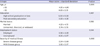
We conducted exploratory factor analyses of the preliminary version of the SRSM to uncover the internal structure of the scale. During exploratory factor analyses, questions about illness perception (item 2: anticipation for the effect of treatment), hopelessness (item 9: things won't be bad all of the time), and impulsivity (item 12: ability to suppress emotion) were found to lower consistency of the scale, and were excluded. Exploratory factor analyses were then performed with remaining nine items. As a result of these analyses, a single factor model was developed. Among the nine items, questions about illness perception (item 1: effect of physical illness on mind), and impulsivity (item 11: acting without contemplation) showed low communalities (< 0.4). These items were also excluded. As a result, the final version of the SRSM consisted of seven items in single factor model, and this model accounted for 65.12% of total variation (Table 2). The Cronbach's alpha of the SRSM was 0.910, suggesting a high degree of internal consistency. The mean score of the SRSM was 4.64 ± 5.04 (Table 1).
Table 2
Factor analysis of SRSM

![]()
Test-retest reliability
The Pearson's correlation coefficient of test and retest scores of the SRSM was r = 0.635 (P < 0.01), suggesting good test-retest reliability.
Concurrent validity
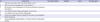
In this study, all 100 participants completed the HADS, BHS, and BSI. The Pearson's correlation coefficient of the SRSM and HADS scores was r = 0.727 (P < 0.001), suggesting strong positive correlation. The Pearson's correlation coefficient of SRSM scores and the scores of the HADS anxiety and depression subscales were r = 0.793 (P < 0.001) and r = 0.551 (P < 0.001), respectively, suggesting the anxiety subscale is more correlated with the SRSM. The Pearson's correlation coefficients of SRSM scores and BHS and BSI scores were r = 0.360 (P < 0.001) and r = 0.584 (P < 0.001), respectively, suggesting significant positive correlation (Table 3).
Table 3
Correlation of scores of each scale with the total score of the SRSM

SRSM = Suicide Risk Scale for Medical inpatients, HADS = Hospital Anxiety and Depression Scale, HADS-A = Anxiety subscale of Hospital Anxiety and Depression Scale, HADS-D = Depression subscale of Hospital Anxiety and Depression Scale, BHS = Beck Hopelessness Scale, BSI = Beck Scale for Suicide Ideation.
aP < 0.01.
![]()
Comparison of SRSM score between different groups
We compared the mean SRSM scores of different groups according to age (participants aged 65 years or older vs. those under 65 years), marital status (married participants vs. unmarried, divorced, or widowed participants), education level (participants who achieved high school graduation or less vs. those with post-secondary education), employment status (employed participants vs. unemployed participants), and illness (participants with severe disease vs. those with mild disease). The SRSM mean score was significantly different only in the illness groups. The SRSM mean score in the severe disease group was 5.54 ± 5.60 and the SRSM mean score in the mild disease group was 2.82 ± 2.97 (P < 0.010) (Table 4).
Table 4
SRSM score according to different groups
Severe disease group: patients in severe disease group are patients who diagnosed with disease which classified as ‘severe disease’ according to NHIA of Korea. Mild disease group: patients in mild disease group are patients who diagnosed with disease other than ‘severe disease’.
SRSM = Suicide Risk Scale for Medical inpatients, NHIA = National Health Insurance Act.
![]()
Diagnostic utility of the scale
ROC analysis was performed to test the diagnostic utility of this scale and to identify the appropriate cut-off score. Area under the curve of the SRSM was estimated as 0.797. We evaluated sensitivity and specificity at each cut-off score to calculate the optimal cut-off score. A score of five was determined as the optimal cut-off, with 71.4% sensitivity and 75.6% specificity (Table 5). In this study, 36% of participants had an SRSM score that was higher than the cut-off score.

DISCUSSION
Inpatient suicide has a negative impact not only on the individual who committed suicide, but also on other patients and medical staff. Thus, careful attention to suicide prevention is important to guarantee a more favorable hospital environment. However, as far as we have found, recent studies have primarily focused suicide in psychiatric unit, and little is known about screening suicide risk in medical setting. The aim of our study was to develop a suicide risk-screening tool that can be applied to medical inpatients.
During the course of development of the SRSM, we considered three conditions as necessary for acceptable screening of suicide risk in inpatients. The first condition was brevity. In a primary clinical setting, it is impossible for mental health professionals to assess the suicide risk of every inpatient. Furthermore, patients have a negative response to being questioned about suicide for a long period of time. Therefore, a screening tool for inpatient suicide risk should be brief enough that can be easily performed by primary physicians or nursing staff. The second condition was capacity to reflect a patient's physical illness appropriately. Physical illness itself is an overwhelming life event which may cause psychiatric impairment to previous healthy individuals.5 Thus, an appropriate screening tool should contain items related to physical illness. For this purpose, we referred to a scale pertaining to illness perception, “Brief IPQ,” during development of the SRSM, though items extracted from the scale have been excluded during exploratory factor analysis. We also performed a preliminary survey with 100 patients and, after analyzing the results, included pain perception in the SRSM. The third condition was verified concurrent validity with previous scales. We selected three scales for verifying concurrent validity: the HADS, BSI, and BHS. The HADS focuses on psychiatric symptoms commonly seen in hospital. The BSI and BHS are well known scales for assessing suicide risk. As there is no current standard instrument to evaluate suicide risk in medical inpatients, verifying concurrent validity with these three scales was the optimal method to test the validity of the SRSM. The SRSM was regarded as meeting the above three conditions.
During the course of exploratory factor analysis, a total of five items were removed from the preliminary version of the SRSM. Three of the items (item 2, item 9, and item 12) were excluded because they were found to lower the consistency of the scale. Interestingly, these were all reverse-scoring items, where a positive response means lower suicide risk, in contrast to other items. This finding suggests that reverse-scoring items may not suitable for this due to the characteristics of the medical inpatients questioned. A number of the patients participating in this study are older, have a lower education level, are socially inactive (unemployed), and have severe medical illnesses. It may be that these inpatients are less able to discriminate the delicate meaning of reverse-scoring items. The remaining survey items tend to be more simple and distinct in description. Two items were excluded owing to low communalities. Those two items were extracted from the Brief IPQ and BIS. The seven items that comprised the final version of the SRSM were items extracted from validated Korean versions of different mental health scales, or items adopted as the result of preliminary survey (Table 6, Supplementary Table 1).
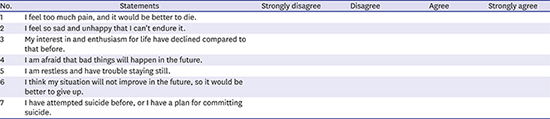
Table 6
Suicide Risk Scale for Medical inpatients
Score each item with the following points: strongly disagree, 0; disagree, 1; agree, 2; strongly agree, 3. The Suicide Risk Scale for Medical inpatients was developed in Korean. An English version of this scale has not yet been validated.
![]()
Although items of SRSM were extracted and modified from various sources, exploratory factor analysis revealed that they consisted of a single factor. This could possibly be attributed to the characteristics of suicidality. Suicide is the result of the interaction of several different factors.27 If a mediator exists, linking those different factors, the factors may actually consist of a single factor. In our study, ‘emotion’ was suggested as the mediator of various factors. The high Cronbach's alpha of the SRSM (0.910) supports the hypothesis that items in the scale are linked by strong mediator.
In our study, severity of illness was the only factor which showed discriminant suicide risk. Our finding suggests that clinician should be alert when treating patients with severe disease, even when he or she seems to be stable in regards to other demographic or socioeconomic aspects.
This study has several limitations. First, this study was designed, and its validity was tested, by showing correlation with previously validated scales, not by correlation with actual suicide attempts, successful or otherwise. Correlation with previously validated scales does not guarantee that SRSM can predict actual commitment of suicide. Second, the calculation of the cut-off score was based on the BHS score, and not on a suicide risk scale or other suicide risk assessment. The BSI has no established specific cut-off score, and any positive score warrants further evaluation.24 In contrast, the relationship between the BHS score and actual suicide are comparatively well established.2829 A BHS score of 15 points indicates a severe level of hopelessness,19 and Cochrane-Brink et al.30 suggested that point as a cut-off score for suicide risk with 100% sensitivity and 71% specificity. As such, we considered the BHS as the best available standard tool for calculating the cut-off score of the SRSM.
To resolve these limitations, additional study is required. In a follow-up study, validity of the SRSM should be verified by its ability to predict actual suicide attempts, successful or otherwise. Similarly, the cut-off score of the SRSM should be reassessed based on suicide risk evaluation by psychiatrist, in both consultation and liaison settings.
 XML Download
XML Download