

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Sleep disturbance, which is one of the most common non-motor symptoms of Parkinson's disease (PD), increases in frequency with advancing disease.1 A community-based study reported that 60% of patients with PD (144 of 239 patients) had sleep problems, compared with 33% of healthy age- and sex-matched controls (33 of 100 healthy participants).2 A study on prevalence, using a non-motor symptoms questionnaire, demonstrated daytime sleepiness (DS) in 31% of patients with PD, insomnia in 46%, restless legs in 42%, vivid dreams in 34%, and acting out during dreams in 36%.3 Sleep problems have a significant negative impact on the quality of life of patients and their caregivers.45 Therefore, recognition and appropriate management of sleep problems are vitally important in PD treatment.
The Scales for Outcomes in Parkinson's Disease-Sleep (SCOPA-S) evaluates sleep problems using a self-administered questionnaire.6 The nighttime sleep (NS) section, which addresses sleep problems during the night in the prior month, consists of five items with four response options (i.e., 0 [not at all] to 3 [a lot]), with a maximum score of 15. The DS section evaluates sleepiness during the daytime in the prior month, and includes six items with four response options (i.e., 0 [never] to 3 [often]), with a maximum score of 18. Additionally, overall sleep quality (SQ) is also assessed with seven response options (i.e., 0 [slept very well] to 6 [slept very badly]).
In the present study, we translated SCOPA-S into Korean and evaluated its reliability and validity for use in Korean patients with PD.
METHODS
Study design and setting
Study participants
We recruited patients with PD, aged above 39 years, from 27 movement disorder centres of university-affiliated hospitals in Korea. The diagnosis of PD was made according to the clinical diagnostic criteria of the United Kingdom Parkinson's Disease Society Brain Bank.7
The exclusion criteria were as follows; diagnosis of secondary Parkinsonism or symptoms suggesting Parkinson plus syndrome, history of psychiatric illness, and current or past use of antidepressants or medication that can cause drug-induced Parkinsonism.
Translation
The following steps were taken to translate the original English version of SCOPA-S6 (Appendix 1) into Korean: forward translation and backward translation, expert committee review, pretest of the pre-final version, and development of the final Korean version.
First, two independent bilingual translators translated the English version of SCOPA-S into Korean, literally. A panel consisting of five authors (Ahn TB, Cheon SM, Kim JS, Kim SJ, and Koh SB) reviewed the translations to form a single forward translation. Another bilingual translator translated the Korean version draft of SCOPA-S back into English. The panel then evaluated discrepancies between the original English form and the first draft of the Korean translation. Interview with four patients was performed to test the interpretation of the translation. Thereafter, we generated the final Korean version of SCOPA-S (K-SCOPA-S) (Appendix 2).
Assessment
Clinical assessment was conducted using the following tools: modified Hoehn and Yahr Scale (HYS),8 Unified Parkinson's Disease Rating Scales part I, II, and III (UPDRS I, II, and III),9 the Korean version of the SCOPA-cognition, autonomic, and psychosocial, the Korean version of the Mini-Mental Status Examination (K-MMSE),10 the Korean version of the Montreal Cognitive Assessment (MoCA-K),11 the Korean version of the Montgomery-Asberg Depression Scale (K-MADS),12 the Parkinson's Disease Sleep Scale 2nd version (PDSS-2),13 the Korean version of the 39-item Parkinson's Disease Questionnaire (K-PDQ39),14 the Korean version of the Non-motor Symptoms Scale (K-NMSS),15 the Rapid Eye Movement Sleep Behavior Disorders Screening Questionnaire (RBDQ),16 and the Neurogenic Orthostatic Hypotension Questionnaire (NOHQ).17
For the test-retest reliability, K-SCOPA-S assessments were repeated twice, with an interval of 10–14 days, allowing sufficient time to minimize learning effect.
Statistical analysis
The quality of data was considered satisfactory if more than 95% of the scale data were fully computable. Reliability was tested for internal consistency and stability of measures. Internal consistency was analyzed using the Cronbach's α-coefficient (criterion value for α: ≥ 0.70). The item homogeneity (mean of the inter-item correlation coefficients, criterion value: ≥ 0.30) and corrected item-total correlations (without contribution of the tested item, criterion value: ≥ 0.40) were determined to ascertain the internal consistency of K-SCOPA-S.
The test-retest reliability was assessed using intraclass correlation coefficient (ICC). Correlation values of 0.70 or greater were considered satisfactory. Comparison of baseline and follow-up scores was performed using a Wilcoxon's test. In addition to identifying the association between variables, the Spearman's rank correlation coefficients (rS) were used to analyze the construct validity with other scales. All statistical analyses were performed using SPSS 17.0 (SPSS, Inc., Chicago, IL, USA).
RESULTS
Demographic features
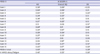
Among the 136 patients who were enrolled in this study, 133 patients completed the retest step. The study cohort comprised 65 men and 71 women, with a mean age of 66.8 ± 9.0 years. The median HYS was 2 (19 patients at stage 1, 7 at stage 1.5, 55 at stage 2, 32 at stage 2.5, 21 at stage 3, 1 at stage 4, and 1 at stage 5). The demographic and clinical characteristics are summarized in Table 1.
Table 1
Demographics and clinical characteristics
SD = standard deviation, HYS = Hoehn and Yahr Scale, UPDRS = Unified Parkinson's Disease Rating Scale, K-MMSE = Korean version of the Mini-Mental Status Examination, MoCA-K = Korean version of the Montreal Cognitive Assessment, K-MADS = Korean version of the Montgomery-Asberg Depression Scale, K-NMSS = Korean version of the Non-motor Symptoms Scale, K-PDQ39 SI = Korean version of the 39-item Parkinson's Disease Questionnaire summary index, K-SCOPA = Korean version of Scales for Outcomes in Parkinson's Disease, RBDQ = Rapid Eye Movement Sleep Behavior Disorders Screening Questionnaire, NOHQ = Neurogenic Orthostatic Hypotension Questionnaire.
![]()
Validation results
The mean sub-scores of K-SCOPA-S were 3.8 for NS and 2.6 for DS. The median score of K-SCOPA-S SQ was 2. Descriptive data and acceptability parameters of K-SCOPA-S are shown in Table 2.
Table 2
Descriptive statistics, and acceptability parameters of the K-SCOPA-S
K-SCOPA-S = Korean version of Scales for Outcomes in Parkinson's Disease-Sleep, SD = standard deviation, NS = nighttime sleep, SQ = sleep quality, DS = daytime sleepiness.
![]()
Internal consistency
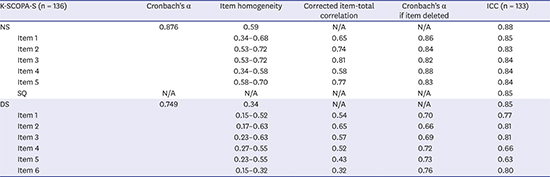
Table 3 displays data on internal consistency of K-SCOPA-S. The Cronbach's α-coefficients were 0.88 and 0.75 for the NS and DS subscales, respectively. The corrected item-total correlations ranged from 0.58 to 0.81 for the NS subscale and from 0.32 to 0.65 for the DS subscale. The corrected item-total correlations for all items, except K-SCOPA DS item 6, were ≥ 0.40. The inter-item correlation coefficient was 0.59 and ranged from 0.34 (items 1 and 4) to 0.72 (items 2 and 3) for the NS subscale, and was 0.34 and ranged from 0.15 (items 1 and 6) to 0.63 (items 2 and 3) for the DS subscale.
Table 3
Internal consistency and test-retest reliability of the K-SCOPA-S for PD
K-SCOPA-S = Korean version of Scales for Outcomes in Parkinson's Disease-Sleep, PD = Parkinson's disease, ICC = intraclass correlation coefficient (using mixed model, type consistency, averaged measures), NS = nighttime sleep, N/A = not applicable, SQ = sleep quality, DS = daytime sleepiness.
![]()
Test-retest reliability
There was no significant difference between initial and follow-up scores (P > 0.05, Wilcoxon's test). Test-retest reliability of K-SCOPA-S, which was determined in 133 patients who performed the test twice, was 0.88 (ranged from 0.83 to 0.85) for the NS subscale, 0.85 for single-item on SQ, and 0.85 (ranged from 0.63 to 0.81) for DS (Table 3). The ICCs for all the items, except DS items 4 (0.66) and 5 (0.63) were ≥ 0.70.
Construct validity
The correlation coefficient between K-SCOPA-S SQ and NS section was 0.66 (P < 0.001), whereas there was no significant correlation between K-SCOPA-S SQ and DS section. The SQ and NS sub-scores of K-SCOPA-S were significantly correlated with PDSS-2 item 1 (the overall quality of your night's sleep is), PDSS-2 total score, and sleep/fatigue sub-score of the K-NMSS (Table 4). Among the PDSS-2 items, item 2 (difficulty falling asleep) had the highest correlation (rS = 0.64; P < 0.001) with K-SCOPA-S NS subscale (Table 4). There was a significant, but weak correlation between the DS sub-score, and the PDSS-2 total score (rS = 0.29; P < 0.001) and sleep/fatigue sub-score of K-NMSS (rS = 0.26; P < 0.001).
Table 4
Convergent validity of the K-SCOPA-S for PD
K-SCOPA-S = Korean version of Scales for Outcomes in Parkinson's Disease-Sleep, PD = Parkinson's disease, NS = nighttime sleep, SQ = sleep quality, DS = daytime sleepiness, PDSS-2, Parkinson's Disease Sleep Scale 2nd version, K-NMSS = Korean version of the Non-motor Symptoms Scale.
aP < 0.01 by Spearman correlation; bP < 0.05 by Spearman correlation.
![]()
Correlation between K-SCOPA-S and other clinical variables
Correlation coefficients of K-SCOPA-S sub-scores with the PD-related scales are shown in Table 5. The correlations of K-SCOPA-S DS and NS sub-scores with HYS, UPDRS I, and UPDRS II were significant. The DS sub-score of K-SCOPA-S was significantly correlated with UPDRS III, while SQ and the NS sub-scores of K-SCOPA-S were not. K-MMSE and MoCA-K scores were not correlated with K-SCOPA-S scores.
Table 5
Correlation of the K-SCOPA-S for PD with clinical variables
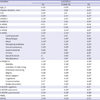
K-SCOPA-S = Korean version of Scales for Outcomes in Parkinson's Disease-Sleep, PD = Parkinson's disease, NS = nighttime sleep, SQ = sleep quality, DS = daytime sleepiness, HYS = Hoehn and Yahr Scale, UPDRS = Unified Parkinson's Disease Rating Scale, K-MMSE = Korean version of the Mini-Mental Status Examination, MoCA-K = Korean version of the Montreal Cognitive Assessment, K-MADS = Korean version of the Montgomery-Asberg Depression Scale, K-NMSS = Korean version of the Non-motor Symptoms Scale, K-PDQ39 SI = Korean version of the 39-item Parkinson's Disease Questionnaire summary index, K-SCOPA = Korean version of Scales for Outcomes in Parkinson's Disease, RBDQ = Rapid Eye Movement Sleep Behavior Disorders Screening Questionnaire, NOHQ = Neurogenic Orthostatic Hypotension Questionnaire.
aP < 0.01 by Spearman correlation; bP < 0.05 by Spearman correlation.
![]()
The K-SCOPA-S DS sub-score had a moderate correlation with the cognitions sub-score of K-PDQ39 (rS = 0.48). The SQ sub-score was moderately correlated with K-MADS score (rS = 0.44), while the NS and DS sub-scores were weakly correlated (rS = 0.32 and 0.27, respectively). All the sub-scores of K-SCOPA-S had a significant correlation with the K-NMSS total, the K-PDQ39, the K-SCOPA autonomic and psychosocial, and the NOHQ scores. The DS sub-score of K-SCOPA-S was significantly correlated with RBDQ, while SQ and the NS sub-score of K-SCOPA-S was not.
DISCUSSION
We translated the SCOPA-S into Korean using a standard method to overcome the language barrier. We found K-SCOPA-S to be a reliable and valid instrument applicable to a Korean-speaking PD population. The assessment was done in 27 different movement-disorder clinics by different investigators, which strengthened the impact of our study and the usefulness of K-SCOPA-S in clinical practice.
The mean NS and DS sub-scores of the K-SCOPA-S were lower in comparison to the results found using the Dutch and Thai versions of SCOPA-S.618 This discrepancy could be attributed to the milder severity and earlier stages of PD in patients in the current study cohort, compared to those in the original Netherlands study, or to the effect of weather (e.g., tropical night phenomenon) on SQ in Thailand. The mean NS and sub-scores of the current study were, however, similar to those reported using the Swedish version of K-SCOPA-S.19 The disease duration and severity in the Swedish patients with PD in that previous study was similar to those in the Korean patients with PD included in the current study.
Since a cut-off above 0.7 for Cronbach's α-coefficients is acceptable for internal consistency and reliability, the internal consistency of K-SCOPA-S was satisfactory, as Cronbach's α-coefficient was 0.876 and 0.749 for NS and DS, respectively. Test-retest reliability, which was 0.88 and 0.85 for NS and DS, respectively, when assessed by ICC, was also adequate. These results suggested that the K-SCOPA-S is a valid and reliable instrument to assess SQ in Korean patients with PD.
The SQ and NS sub-scores of K-SCOPA-S were significantly correlated with PDSS-2 item 1, PDSS-2 total score, and the sleep/fatigue sub-score of K-NMSS. However, the DS sub-score of K-SCOPA-S was only significantly correlated with the PDSS-2 total score and K-NMSS sub-score. This discrepancy may be related to the fact that PDSS-2 mainly evaluated NS (only 1 item assesses DS), whereas K-SCOPA-S evaluated both NS and DS in a more balanced way (5 and 6 items, respectively). The strength of SCOPA-S in the assessment of both nocturnal and daytime sleep problems was similarly addressed in a previous study comparing SCOPA-S and PDSS.20
K-SCOPA-S was significantly correlated with scales for non-motor symptoms (namely, UPDRS I, K-NMSS, K-MADS, K-SCOPA autonomic, and K-SCOPA psychosocial), activities of daily living (UPDRS II), quality of life (K-PDQ39), neurogenic hypotension (NOHQ), and RBDQ (Table 5). The close correlations between sleep and mood/depression or quality of life in PD have been previously highlighted in other studies.2021222324252627 This study showed that sleep problems measured by K-SCOPA-S were correlated with specific non-motor symptoms such as dysautonomia (K-SCOPA-autonomic and NOHQ) in addition to a general measure (K-NMSS) or psychosocial measure (K-SCOPA psychosocial). In line with these findings, it was reported that dysautonomia was more severe in those with sleep problems in PD.28 Interestingly, the DS sub-score rather than the NS sub-score was significantly correlated with RBDQ. The importance of DS in rapid eye movement sleep behavior disorder (RBD) was previously reported. DS was higher in those with RBD than without RBD in PD and an important predictor for the conversion into neurodegenerative disorders in idiopathic RBD, suggesting that DS could be related to more severe pathologies in the brain including arousal system.2930 Our study showed that K-SCOPA-S was useful in detecting sleep problems in PD and its clinical significance was substantiated by the close association with other non-motor scales, which was consistent with previous studies.
In the current study, specialized scales for cognition, such as K-MMSE, MoCA-K, and K-SCOPA cognition showed poor correlation with K-SCOPA-S, whereas sub-scores of K-NMSS (attention/memory) and K-PDQ39 (cognition) showed significant correlations. Previous studies showed that sleep disturbance exerted an adverse effect on cognitive function in patients with PD.31 According to a recent meta-analysis, sleep disorders in patients with PD were associated with memory and executive function.32 Patients with PD and RBD reported more cognitive dysfunction.33 Thus, it is plausible that sleep problems have a significant effect on the cognition of patients with PD. Rather than directly measuring cognitive function, the questions on cognition of patients with PD, in the K-NMSS and K-PDQ39, are actually designed to identify practical problems related to cognitive dysfunction. Therefore, the significant correlation between K-SCOPA-S and the cognitive items in K-NMSS/K-PDQ39 may support the usefulness of these scales in the practical management of patients with PD.
The subscales of K-SCOPA-S, except SQ, were partly correlated with motor scales of PD (HYS and UPDRS III), although the correlation was not strong. A preliminary study of PDSS reported a significant difference between advanced and early PD,34 which was not confirmed by others.3536 In other studies, sleep problems were associated with disease severity.3738 Thus, sleep deteriorates with disease progression. Interestingly, an 8-year follow-up study showed a significant fluctuation of the severity of insomnia in a cohort of patients with PD.39 Thus, sleep disorder in PD was not homogeneous along the course of the disease and its manifestation may not be determined by a simple factor (disease severity).373839
A few limitations in our study must be noted. The majority of patients in the current cohort had a HYS score of 2.5 or less (81.8%), which could be a limitation. Since this study required two consecutive visits at an interval of 2 weeks, it was challenging to recruit patients with advanced PD. Nonetheless, the correlation between disease severity and K-SCOPA-S was only partial and weak, suggesting that disease severity was not a strong confounder. The second potential limitation of this study is the use of a self-questionnaire for data acquisition. However, the test-retest reliability of K-SCOPA-S was excellent enough to argue against the uncertainties associated with the subjective assessment of sleep problems.
In conclusion, the results of the current study demonstrated that K-SCOPA-S exhibited good reliability and validity to assess sleep problems in Korean patients with PD. Moreover, its clinical usefulness was substantiated by its significant correlation with other measures of clinical assessment.
 XML Download
XML Download