

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hemophilia A is an X-linked recessive inherited bleeding disorder caused by a deficiency in coagulation factor VIII (FVIII), which causes acute bleeding episodes. The common morbidity associated with hemophilia is recurrent bleeding into joints, which can lead to long-term complications such as chronic arthropathy. The mainstay of treatment is prophylactic or on-demand replacement therapy with plasma-derived (pd) or recombinant (r) FVIII concentrates. Treatment has progressed from the use of blood transfusions to pdFVIII concentrates and, more recently, the use of rFVIII concentrates.123
Common treatment switches are from pdFVIII to rFVIII products and between different recombinant products. When choosing between FVIII products, the physician must consider various factors, including safety, efficacy, cost, and supply/availability.4
GreenGene F™ (beroctocog alfa; Green Cross Corporation, Yongin, Korea) is a new third generation rFVIII developed to treat hemophilia A patients. By applying various improvements to enhance quality, GreenGene F™ has significantly reduced the potential risk of viral pathogen transmission and can be considered to be of higher technical quality than other available products. GreenGene F™ was launched in 2010 using advanced state-of-the-art technology and processes, without the use of human or animal-derived albumin or other plasma proteins, including viral inactivation (solvent/detergent treatment) and viral removal (nanofiltration) steps.56 GreenGene F™ attains high purity and high homogeneity through its cultivation technology and the purification process. A continuous cell culture technology and a unique purification process have been adopted to make high quality FVIII protein homogeneously, and a 20 nm nanofiltration is applied in the manufacturing process to significantly improve product safety.6
Changing the type of factor concentrate may be beneficial to promote improved safety of new products, lower cost, provide more convenient product administration or storage, reduce injection frequency due to a longer half-life, improve national contracting, offer wider patient/family options, and foster greater participation in clinical research.7 However, the development of anti-FVIII inhibitors is the most serious adverse event (SAE) of hemophilia treatment. Neutralizing allo-antibodies to FVIII occur in approximately 30% of previously untreated patients (PUPs) with severe hemophilia A.89 Although such anti-FVIII antibodies occur far less frequently in previously treated patients (PTPs),1011 there is some concern that switching treatments may increase the risk of inhibitor development. Because of the detrimental complication of FVIII inhibitors, new FVIII products must be carefully screened for any increased propensity to induce inhibitor formation, with continuous monitoring for inhibitor development.
We performed post-marketing surveillance (PMS) of GreenGene F™ to assess its safety and efficacy in patients with hemophilia A.
METHODS
Patients
Patients of any age with hemophilia A who were either naive to FVIII products or who had been treated previously with any of the FVIII products other than GreenGene F™ were eligible. PUPs were defined as those with ≤ 3 exposure days (EDs) in the month before screening and no other FVIII concentrate use. PTPs were defined as having > 50 EDs to FVIII products. FVIII inhibitors were measured by the Nijmegen-Bethesda method. Patients with an FVIII inhibitor titer of ≥ 0.6 Bethesda unit (BU) at enrollment, as determined by the local laboratory or by patient records, were excluded.
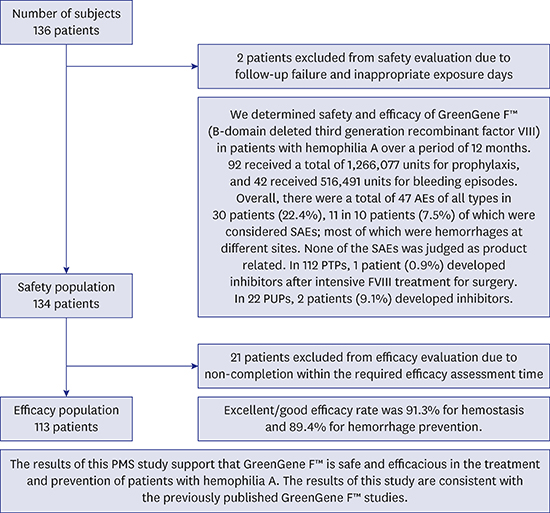
From July 2010 to July 2014, a total of 162 case report forms (CRFs) from Korean hemophilia A patients were collected from 12 hospitals (Korea Hemophilia Foundation clinics, university hospitals, and general hospitals) in the PMS study and were analyzed for drug safety and efficacy. Twenty-six CRFs were duplicated and 1 patient was not available for a follow-up survey, and a 43-year-old patient with FVIII 3% who had received on-demand FVIII agent was excluded because he had received pdFVIII less than 50, and more than 3 EDs. Among the 134 patients, a total of 113 patients were analyzed for drug efficacy, and 21 patients were excluded for non-completion within the required efficacy assessment time (Fig. 1).

Patients with differing hemophilia A severities and medical histories were monitored during 12 months of prophylactic and/or on-demand therapy. The monitoring schedule, including the frequency of inhibitor testing, was determined by the treating physician. Laboratory tests for FVIII:C and FVIII inhibitor were performed at the source clinic attended by the patient. Based on the correlation between factor concentration and clinical manifestation, hemophilia A was classified as follows: severe (FVIII:C < 1.0 IU/dL), moderate (FVIII:C 1–5 IU/dL), and mild (FVIII:C > 5–40 IU/dL). Inhibitors to FVIII with an assay value of 0.6–5 BU were defined as low titer, and those with values > 5 BU were defined as high titer. A positive inhibitor result was defined as ≥ 0.6 BU. Hemophilic arthropathy was defined as stage II or more by the Arnold-Hilgartner classification or as having existing joint deformity or a limited joint range of motion in the limbs. Hepatitis C was defined as hepatitis C virus (HCV) polymerase chain reaction (PCR) positive, with positive anti-HCV antibodies and a serum alanine aminotransferase (ALT) > 50 IU/L.
Of the 134 patients, 22 were PUPs and 112 were PTPs. Following enrollment, information in relation to demography data, family history, past history of replacement therapy and history of concomitant diseases was collected. The scheduled doses of GreenGene F™ for bleeding episodes or prophylaxis followed the generally accepted guidelines for the treatment of hemophilia A-related bleeding. After each infusion of GreenGene F™, patients were monitored for significant changes in vital signs, other adverse signs or symptoms, and the clinical response to treatment. The study was approved at each hospital by the local Institutional Review Board. Informed consent was obtained from each individual (or guardian) prior to enrollment.
Safety and efficacy
Adverse events (AEs) were defined as any unfavorable and unintended signs, symptoms or changes from baseline, with the use of GreenGene F™, deemed related or unrelated to GreenGene F™. SAEs were defined as AEs resulting in death, a life-threatening adverse drug experience, inpatient hospitalization or prolongation of an existing hospitalization, a persistent or significant disability/incapacity, a congenital anomaly/birth defect, or other occurrences that could jeopardize the patient and require medical or surgical intervention to prevent one of the outcomes listed in this definition. The development of FVIII inhibitors was also considered an SAE. All AEs following drug administration within the PMS study were recorded and assessed for seriousness, the relationship to GreenGene F™ (unrelated, possibly related, or probably related), and severity (mild, moderate, or severe). Safety evaluation included all changes in relation to undesirable medical findings. When the administration of GreenGene F™ ended, monitoring continued (involving a phone call or a request for a home visit for discharged patients) for more than 1 day to assess safety concerns regarding any delayed potential AEs.
Efficacy was rated by the patients' doctors, using a 4-point scale that included excellent, good, moderate, or no effect. The efficacy evaluation scale, assessing the hemostatic effect post-GreenGene F™ administration, was recorded as follows: excellent, when bleeding had completely stopped; good, when bleeding had almost stopped, that is, hemostasis was as good as expected for the type of procedure performed; moderate, when hemostasis was less than optimal, but was maintained without a change in therapeutic regimen; or none, when a hemostatic effect was not attained, that is, there was a lack of hemostatic control in the face of proper dosing, necessitating a change in the therapeutic regimen.
The hemorrhage prevention effects were evaluated using the following criteria: excellent, when hemorrhage was completely prevented; good, when hemorrhage was almost prevented; moderate, when not sufficient to prevent hemorrhage, but some prevention effect was attained; none, when a hemorrhage prevention effect was not attained.
Statistical analysis
Descriptive statistics were used to describe the demographic and clinical characteristics of the study population and follow-up time in the study. Total follow-up time was calculated as either the time from the first infusion of GreenGene F™ to the development of an inhibitor or to the end of the study/last follow-up. Data analysis was performed with IBM SPSS Statistics 19 software (SPSS Inc., Chicago, IL, USA). The patient age was based on the age at first exposure to the study product. Patients enrolled in multiple studies were considered only once. Descriptive data are presented as means and standard deviations, medians and ranges, or frequencies and percentages. Comparisons between groups were made using an independent two-sample t-test or the Wilcoxon rank sum test and χ2 test or the Fisher's exact test.
RESULTS
Patient characteristics and dispositions
Of a total of 136 male patients receiving at least one infusion of GreenGene F™, 134 were included in the safety analysis set after two patients were excluded due to follow-up failure or inappropriate EDs (Fig. 1). The demographics of the 134 treated patients, 112 of whom were PTPs according to our definition, are shown in Table 1. The median age for the safety analysis set was 24 years (0 to 73 years). All patients were Korean males and included adults, children, and adolescents. Among the 134 patients, 85 (63.4%) had severe hemophilia, 34 (25.4%) had moderate hemophilia, and 15 (11.2%) had mild hemophilia. Table 2 summarizes the demographic and baseline characteristics based on a prophylaxis or on-demand initial treatment regimen. Of these 134 patients, 92 received a total of 1,266,077 units for prophylaxis and 42 received 516,491 units for bleeding episodes. Previously used treatment products included pdFVIII (Green Mono™ in 96, Greeneight™ in 71, Monoclate-P® in 5), rFVIII (Advate® in 26, Recombinate® in 19, GreenGene™ in 2). Because 114 of 134 (85.1%) patients were treated for a long period of time, various kinds of FVIII products were injected. Right before PMS study used treatment products were pdFVIII (84 of 114 patients), and rFVIII (30 of 114 patients).
Table 1
Demographic and baseline characteristics based on initial treatment regimen
Data are shown as number (%).
PTP = previously treated patient, PUP = previously untreated patient, SD = standard deviation, ICH = intracranial hemorrhage.
aEpilepsy and nephropathy in 2 cases, one case each of anxiety disorder, attention deficit hyperkinetic disorder, chorioretinitis, cystitis, diabetes mellitus, disorder of vestibular function, gastritis, hemorrhoid, hypertension, hypercholesterolemia, other arthritis, otolithiasis, sleep disorder, splenomegaly, and urticaria; bOne case each of hypercholesterolemia and hemorrhoids.
![]()
Table 2
Demographic and baseline characteristics based on prophylaxis or on-demand initial treatment regimen
Data are shown as number (%).
SD = standard deviation, FVIII = factor VIII.
aFVIII product which was injected to patients right before post-marketing surveillance study.
![]()
Safety
The patients were followed for 12 months. There were no deaths in this study. None of the 134 patients developed hypersensitivity, anaphylaxis, or anaphylactoid reactions. Thirty-three patients (24.6%) developed 50 AEs.
Development of inhibitors
In 112 PTPs, one patient (0.9%) developed inhibitor after intensive FVIII treatment. A 42-year-old patient with an FVIII of 0.5% showed low titer inhibitor at 90 EDs, post-surgical removal of a pseudotumor. Inhibitors were reported in one PUP with severe disease (low titer) and one PUP with moderate disease (high titer). The overall incidence of inhibitor was 9.1% (2/22) in PUPs (Table 3).

Other AEs
Table 4 shows the frequency of AEs (other than inhibitors) according to product relatedness. Overall, there were a total of 47 AEs of all types in 30 patients (22.4%), 11 in 10 patients (7.5%) of which were considered SAEs; most of which were hemorrhages at different sites. None of the SAEs were judged as product related.
Table 4
Other AEsa

AEs = adverse events.
aOnly AEs different from inhibitors are included; bOnly one case each was found, which included muscle hemorrhage, musculoskeletal pain, pain in extremity, localized edema, mass, pyrexia, abdominal wall hematoma, diarrhea, vomiting, hemorrhoids, device-related infection, dizziness, somnolence, hemorrhage, intra-abdominal hematoma, contusion, post-traumatic pain, road traffic accident, subcutaneous hematoma, eczema, urticaria, nephrolithiasis, food allergy, and synovectomy.
![]()
Nine non-serious AEs in eight patients (6.0%) were related to GreenGene F™. The most frequent product-related AEs were in relation to gastrointestinal, nervous system, vascular, and general symptoms, which were well tolerated and recovery occurred without special management. One patient showed syncope but otherwise demonstrated normal vital signs, and recovered in 1–2 minutes with no further issues.
Efficacy
Of the 134 patients, 113 were assessed for efficacy (Table 5). In the efficacy assessment of the hemostatic effect, ‘excellent’ was most commonly observed (53.3%), followed by ‘good’ (38.0%), ‘moderate’ (8.7%), and ‘none’ (0%). In the efficacy assessment of the bleeding prevention effect, ‘good’ was most commonly observed (61.7%), followed by ‘excellent’ (27.7%), ‘moderate’ (10.6%), and ‘none’ (0%). Therefore, the ‘excellent/good’ efficacy rate was 91.3% for hemostatic effects and 89.4% for bleeding prevention effects. The concentrate amounts by EDs showed no differences in efficacy.
Table 5
Efficacy of hemostasis response and hemorrhage prevention effect of GreenGene F™ treatment
![]()
DISCUSSION
GreenGene F™ (beroctocog alfa) is a third generation rFVIII concentrate. This product is an upgraded version of a second generation rFVIII GreenGene™ (beroctocog alfa), developed for higher safety using an advanced manufacturing process, which was shown to be safe and efficacious in patients with hemophilia A.12 The upgraded GreenGene F™ added further improvements, such as a viral inactivation (solvent/detergent treatment) and a viral removal process (20 nm nanofiltration) and a final formulation with stabilizers replacing human serum albumin with amino acids. These improvements aimed essentially to eliminate the potential contamination of viruses and significantly enhance the safety of GreenGene F™ product use.6
GreenGene F™ is homogenously expressed and purified as a heavy chain (A1 and A2 domains) and a light chain (A3, C1, and C2 domains), which is unique among the other FVIII products with their many different heterogenous forms observable on SDS-PAGE. This homogeneity of rFVIII allows for better quality control and safety in following good manufacturing practice (GMP) product quality regulations.6
There were no deaths during this study. No hypersensitivity, anaphylaxis, or anaphylactoid reactions were observed in any patient. A 42-year-old patient showed syncope but demonstrated no distinctive clinical features of allergy such as pruritus, flat skin erythema, and hives. His vital signs were normal, and recovered in 1–2 minutes with no further issues. No more syncope occurred to him despite continued treatment with GreenGene F™, so we concluded that it was not hypersensitivity due to GreenGene F™. Ten patients experienced 11 SAEs other than inhibitors; most of which were hemorrhages at different sites.
In this study, the inhibitor incidence in PTPs was 0.9% (1/112). One middle-aged man developed inhibitor at 90 EDs after intensive GreenGene F™ use following the surgical removal of a pseudotumor. Surgery accompanied by intensive FVIII administration is highly related to antibody formation, with direct effects on an increased rate of antibody formation.131415 Therefore, it is suggested that patients scheduled for surgery remain on their current product without switching in the intraoperative period.
Previously reported inhibitor incidence has been reported as approximately 0.13%–6.7% in PTPs.16171819 Given that switching from full-length FVIII to B-domain-deleted FVIII (Refacto-AF) was not associated with an increased inhibitor development,1920 there may be an ethnic component to varying inhibitor development because the rate of inhibitor development in African-American hemophilia A patients appears to be twice that of Caucasians.2122 The evaluation of more recent data does not support previous studies suggesting that switching products (e.g., recombinant vs. plasma-derived and full-length vs. B-domain modified) significantly influences inhibitor development.451923
In PUPs with hemophilia A, the development of a neutralizing antibody may be result of an intricate interplay of both genetic and environmental factors.24 Although the type of rFVIII product used in PUPs has been implicated as a risk factor for inhibitor development in three clinical studies,152526 other studies show no difference between rFVIII products.9192728 In this study, among 22 PUPs, inhibitors were observed in two infants (9.1%).
Although the numbers involved are relatively small, this PMS data supports the hypothesis that switching patients from another rFVIII therapy onto GreenGene F™ does not seem to carry a significant risk of inhibitor development. However, the risk of inhibitor development for PTPs following a change in rFVIII product use should be evaluated within a larger Korean cohort to identify which treatment practices are associated with a greater likelihood of inhibitor development.29 Because anti-FVIII antibodies occur far less frequently in PTPs, multi-national collaboration is suggested to evaluate the relative immunogenicity of different FVIII concentrates, including post-marketing safety surveillance through large registries.30
This PMS study shows that GreenGene F™ is efficacious for preventing bleeding and treating bleeding episodes. Overall, the ‘excellent/good’ efficacy rate was 91.3% for hemostatic effects and 89.4% for bleeding prevention effects.
A limitation of our study is that it is a surveillance study. Surveillance studies may need very large sample sizes for rare outcomes, such as inhibitor development in PTPs. The monitoring schedule, including the frequency of inhibitor testing, was not on a regular basis, but determined by the treating physician.
In conclusion, the results of this PMS study support the use of GreenGene F™ (beroctocog alfa) as safe and efficacious in patients with hemophilia A for both on-demand treatment of bleeding episodes and for prophylactic treatment. This new rFVIII treatment will allow those involved with hemophilia care and treatment to collect more data prospectively to better address the challenges of hemophilia.
 XML Download
XML Download