

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pediatric deaths can be attributed to several causes, such as congenital or genetic defects, malignant neoplasm, injury, and acute diseases.1 Furthermore, pediatric deaths in different age groups, such as infancy (below 1 year of age), childhood (1–9 years of age), and adolescence (10–19 years of age), can be attributed to different diseases and disorders.1 As medical technology evolves, the trend of causes of pediatric deaths is shifting from acute illnesses or injuries to chronic conditions.23 There are several serious or non-curable fatal pediatric chronic conditions, such as advanced cancer, complex cardiac malformations, cystic fibrosis, and neurodegenerative diseases. These are classified as complex chronic conditions (CCCs), and are defined as “any medical condition that can be reasonably expected to last at least 12 months (unless death intervenes) and to involve either several different organ systems or 1 organ system severely enough to require specialty pediatric care, and probably some period of hospitalization in a tertiary care center.”3
Children dying because of CCCs need special supportive healthcare services, including aggressive pain control and effective symptom relief, sensitive emotional and spiritual care for grief management, and respite and bereavement services for the family. These services together are called pediatric palliative care (PPC).45 Since the establishment of the first PPC service in the United Kingdom in the 1980s, PPC has developed rapidly and has been introduced in developing countries, as well as developed countries, to improve the quality of life of children with serious illnesses.678 There are several obstacles faced (i.e., shortage of healthcare personnel and healthcare organizations providing palliative or hospice care, inadequate funding, and financial burden due to lack of insurance coverage) in establishing comprehensive healthcare services for children with CCCs.91011 Healthcare authorities should have a complete understanding of the trends of pediatric deaths while considering the implementation of a new system and tackle these obstacles. However, to the best of our knowledge, the nation-wide population data of pediatric CCCs have never been examined in Korea.
The present study aimed to comprehensively examine the available information on pediatric deaths due to CCCs in Korea. The study examines the following pieces of information: number of pediatric deaths, major causes of pediatric deaths (disease composition of CCCs and non-CCCs), changes in the trend of causes of pediatric death over time, prevalence of certain types of CCCs, the locations where the majority of deaths occur, locations in which patients are living across the country, and whether healthcare institutions which take care of these patients are providing comprehensive palliative care.
Go to : 
METHODS
Data source
We analyzed the Cause of Death Statistics during 2005–2014 in Korea. These data were obtained from the Korean Statistical Information Service of Statistics Korea (accessible at: http://kosis.kr/eng/). The cause of death statistics contains the following information: the date of death notification, address of the decedent, age of the decedent, gender of the decedent, time of death, place of death, marital status, level of education, cause of death, and nationality of decedent. The cause of death is reviewed and classified according to the Korean standard classification system (Korean Standard Classification of Diseases [KCD]-4,5,6). The underlying cause of death is determined by an automated coding system based on the recommendation of the World Health Organization.12
Operational definition of pediatric deaths and selecting CCCs
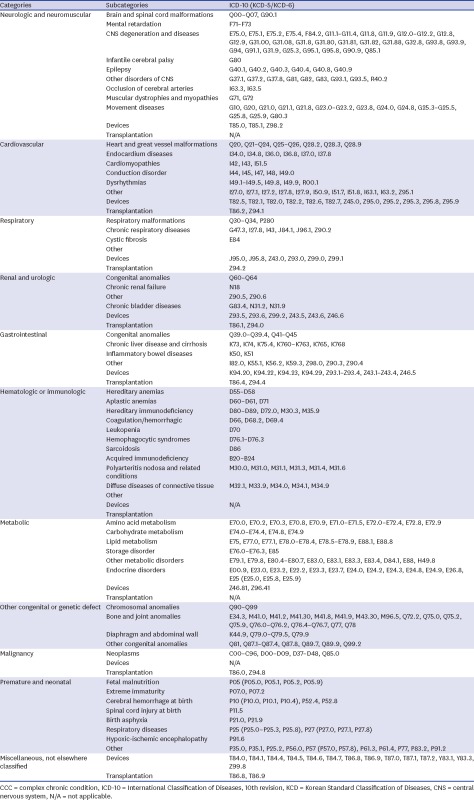
The term “Pediatric deaths” refers to the deaths of people below the age of 20 years. In this study, pediatric deaths were categorized into the following groups: the death of infants (below 1 year of age), children (between 1–9 years of age), and adolescents (10–19 years of age). To identify the population of pediatric patients who need PPC in Korea, we adopted and modified the “Pediatric complex chronic conditions classification system version 2” developed by Feudtner et al.13 According to this classification system, using International Statistical Classification of Diseases, 10th revision (ICD-10) codes, CCCs are divided into 10 disease categories that include neurologic and neuromuscular diseases, cardiovascular diseases, respiratory diseases, renal and urologic diseases, gastrointestinal diseases, hematologic or immunologic diseases, metabolic diseases, other congenital or genetic defects, malignancies, and premature and neonatal disorders (Appendix 1). We modified the classification made up of the ICD-10 codes to use the KCD codes.
Evaluating the level of special PPC in Korea
For children with CCCs, and particularly for children reaching the end-of-life point due to CCCs, special PPC is essential. Although there is no golden standard of PPC across the world, we defined the minimum standard as follows: “comprehensive palliative care for children should be provided as a 24/7 service and the PPC team should consist of multidisciplinary healthcare personnel, including at least 1 physician, 1 registered nurse, and 1 social worker, who have professional knowledge and skills in taking care of children with serious illnesses.” Using this evaluation standard, we examined whether there are hospitals or medical institutions providing adequate PPC in Korea.
Statistical analysis
Descriptive statistics of the study population are presented as number (%) for dichotomous variables. Multivariate logistic regression analysis was performed to investigate the factors that contribute to choosing home as the place of death. All analyses were performed using IBM SPSS Statistics (version 19; IBM Company, Chicago, IL, USA), and the level of significance was set at P < 0.05.
Ethics statement
The present study was exempted from approval from the Institutional Review Board (IRB No. 07-2017-8/052) because it deals with anonymous public data, the Cause of Death Statistics, provided by Statistics Korea. Therefore, we could not locate the subjects of the study, and there was no need for obtaining informed consent from the patients in the present study.
Go to :
RESULTS
Total scale and trends in pediatric deaths from 2005 to 2014
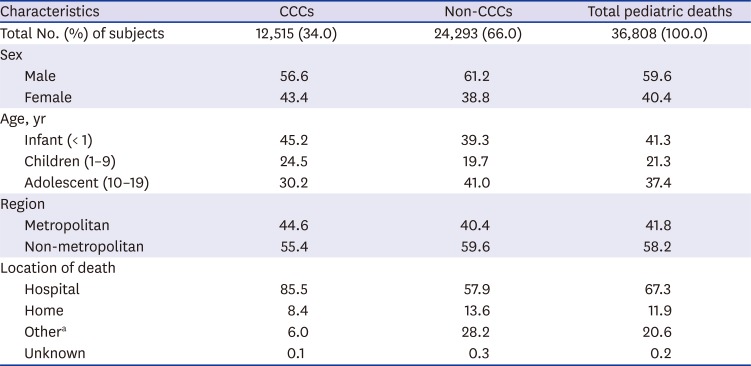
The total cumulative number of pediatric deaths from 2005 to 2014 was 36,808, of which 12,515 (34.0%) were due to CCCs and 24,293 (66.0%) were caused by non-CCCs. Approximately two-thirds of the decedents (67.3%) died in hospitals. In case of CCCs, 85.5% of decedents died in hospitals (Table 1). Fig. 1 shows the distribution of the number of cases of pediatric deaths over the examined 10-year period by age (infancy, childhood, and adolescence) and cause of death (CCCs, non-CCCs, sudden infant death syndrome and injuries). In 2014, the total number of pediatric deaths was 2,914 and CCCs accounted for 1,044 (35.8%) of those deaths. Among the deaths due to CCCs, 641 occurred in infants, 113 in children, and 127 in adolescents. The prevalence of infant, child, and adolescent deaths has declined over 10 years, regardless of the cause of death or the age group. Total pediatric deaths attributed to CCCs per 100,000 children have decreased from 12.2 in 2005 to 9.8 in 2014, but the prevalence of these deaths in infants remains unchanged (Fig. 2).
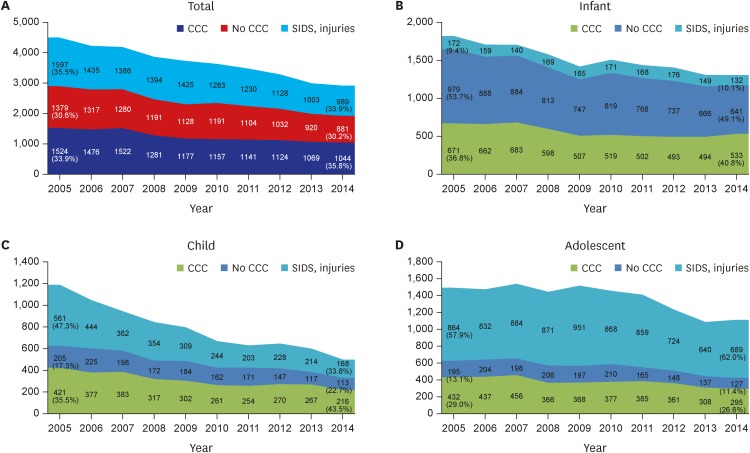 | Fig. 1Trends in pediatric deaths from 2005 to 2014 in Korea by age categories. (A) Total, (B) infant, (C) child, and (D) adolescent (crude number).
CCC = complex chronic condition, SIDS = sudden infant death syndrome.
|
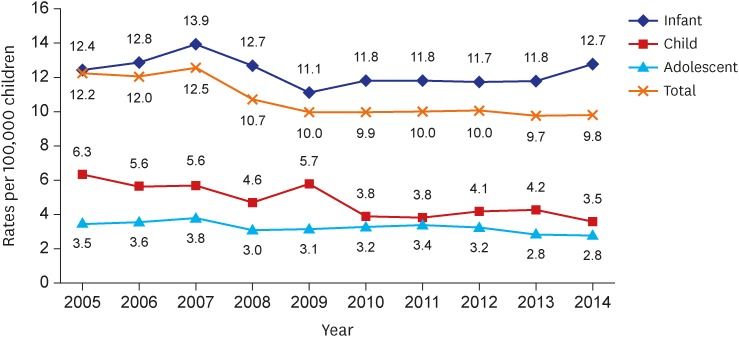 | Fig. 2Trends of age-specific pediatric CCC death rates per 100,000 children over 10 years in Korea.
CCC = complex chronic condition.
|
Table 1
Total scale of pediatric deaths from 2005 to 2014 according to demographic factors
Values are presented as number of patients (%) or percentage.
CCC = complex chronic condition.
aWelfare facilities, on the way to hospital, road, etc.
![]()
Major diseases contributing to pediatric deaths caused by CCCs in different age groups
There were 12,515 pediatric deaths due to CCCs from 2005 to 2014. Overall, malignancy (29.0%) was the leading cause of death, followed by cardiovascular disease (18.9%), and neurologic and neuromuscular diseases (17.9%). However, the proportion of the causes of death differed among different age groups. In infants, neonatal disorders were the most common cause of death (35.6%), followed by cardiovascular diseases (29.8%), and other congenital or genetic defects. In children, malignancies were the most common (43.0%) cause of death, followed by neurologic and neuromuscular diseases (28.9%), and cardiovascular diseases (11.7%). In adolescents, malignancies were the most common (56.2%) cause of death, followed by neurologic and neuromuscular diseases (25.9%), and cardiovascular diseases (8.6%) (Table 2).
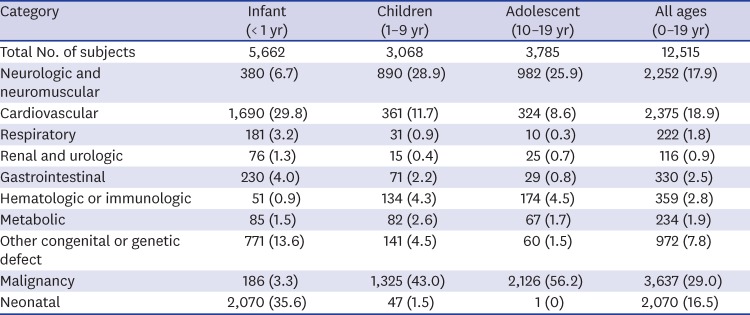
Table 2
Proportion of CCC-attributed pediatric deaths by disease category and age group, 2005–2014
![]()
Factors affecting the choice of place of death among children with CCCs
We examined the locations where the death of the children occurred and the factors affecting the choice of place of death for children with CCCs (Table 3). The frequency of death occurring at home was 1.67 and 2.0 times greater in children and adolescents, respectively, than in infants (P < 0.001). In particular, children living in non-metropolitan areas were 1.21 times more likely to die at home than those in metropolitan areas (P = 0.005). Children with conditions other than hematologic and immunologic diseases were more likely to die at home (P < 0.001) than children with malignancy. Children with hematologic and immunologic disease were less likely to die at home, but this result was not significant (P = 0.154).
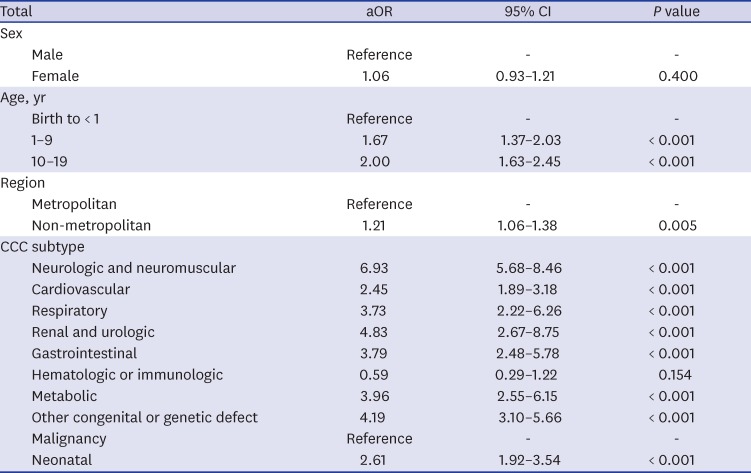
Table 3
Factors associated with home as a place of pediatric death with CCCs
![]()
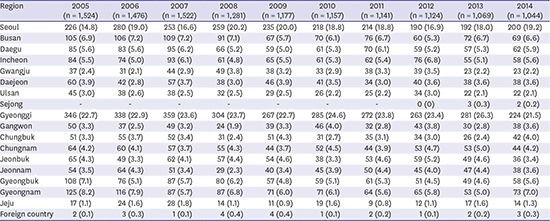
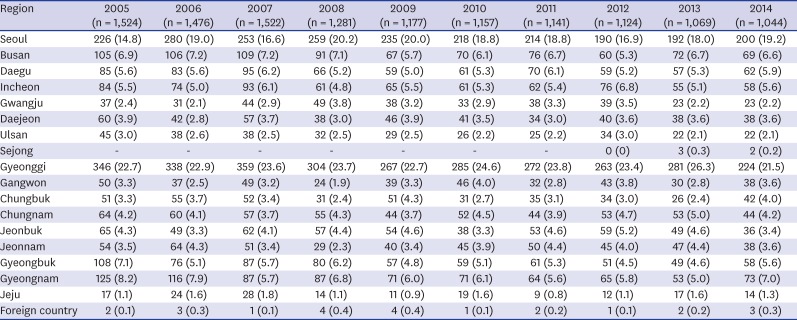
Regional distribution of pediatric deaths due to CCCs and special PPC provisions
In 2014, there were 1,044 pediatric deaths caused by CCCs. Table 4 and Fig. 3 show the regional or geographical distribution of pediatric deaths due to CCCs. The distribution of residential areas in which children died from CCCs was similar to the general population of metropolitan areas and provinces. Based on government reports and media, there was no medical institution or agency that provides PPC services.14 Among 43 tertiary teaching hospitals in Korea, none provided services meeting the minimum standard for special PPC. Two hospitals, both located in Seoul, had in-hospital services called PPC, but they neither had trained healthcare professionals working in a multidisciplinary team, nor provided 24/7 service.
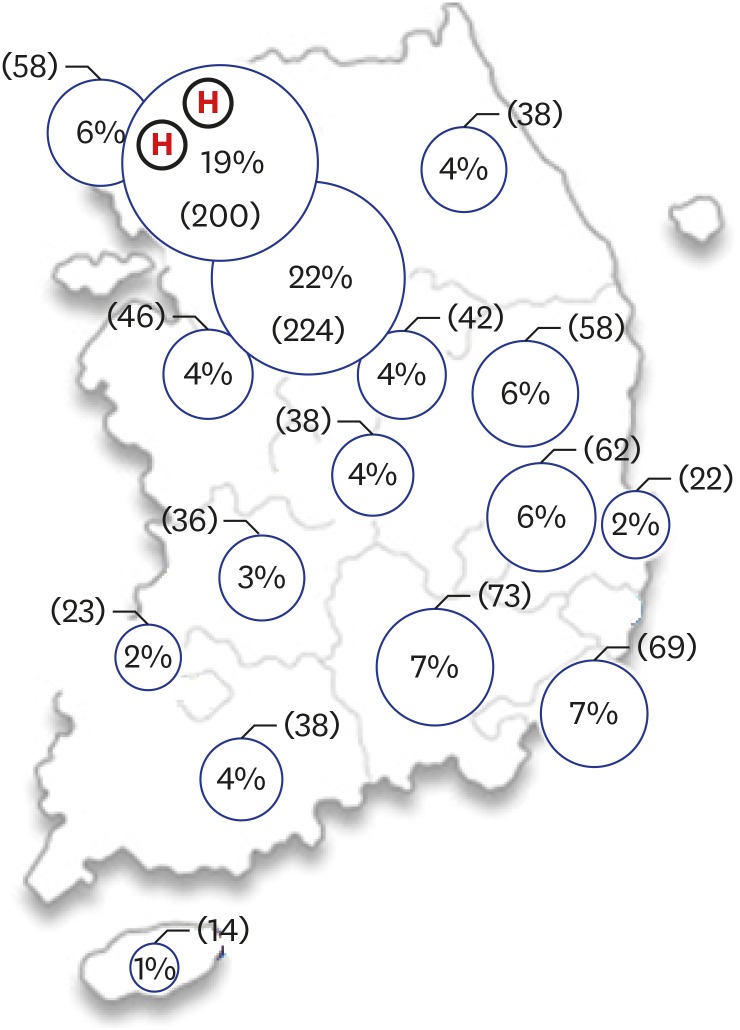 | Fig. 3Regional distribution (proportion and number) of pediatric deaths in 2014 and PPC service in Korea. ‘H’ designates hospitals which runs in-hospital PPC services.
PPC = pediatric palliative care.
|
Table 4
Regional distribution of pediatric deaths attributed to CCCs from 2005 to 2014
![]()
Go to :
DISCUSSION
Children with CCCs need special palliative care services because of the high likelihood of continued suffering owing to physical and psychological symptoms, frequent re-admission, sudden intensive care involvement, and several subspecialty interventions.15
Over the past few decades, significant advances in pediatric healthcare, including disease prevention, diagnosis, treatment, and rehabilitation, have resulted in a reduction in childhood morbidity and mortality rates.1 Even though technological advancement has increased the lifespan of patients suffering from diseases previously considered lethal and improved the quality of long-term care for the pediatric population, the requirement of palliative care services has not yet been addressed in Korea.11617181920212223 To the best of our knowledge, the present study is the first study on childhood mortality due to serious illnesses in Korea, and it revealed that there were 36,808 cases of pediatric deaths during a 10-year period, one-third (12,515 cases, 34.0%) of which were observed in patients with CCCs who would have benefited from PPC. In 2014, 1,044 deaths in children aged 0–19 years were observed, representing a death rate of 9.8 per 100,000. This is a significant decrease from the rate of 12.2 deaths per 100,000 individuals observed in 2005. The rate of pediatric death due to CCCs has declined in children and adolescents, whereas the infant mortality rate remains unchanged. A similar declining trend was previously observed in the United States. Feudtner et al.3 reported that the annual rate of death due to CCCs declined from 1979 to 1997 in almost all age groups, but the rate of medical deaths due to CCCs increased in infants. Neonatal and cardiovascular diseases were the main cause of death in infants, and cancer and neurologic diseases were the main cause of death in children and adolescents. Palliative care is often considered necessary only for cancer patients, but a large proportion of pediatric deaths can be attributed to non-cancer diseases. A study analyzed the data of patients who received hospital-based PPC in the United States and reported that the leading causes of pediatric deaths were genetic/congenital conditions (40.8%), neuromuscular conditions (39.2%), and cancer (19.8%).24 It is imperative to identify the distribution of pediatric deaths by age and disease because the illness trajectory and the type of palliative care services required vary according to these factors.25 Diversity of the age of the patients and type of disease have made it difficult to create a comprehensive plan for implementing PPC services nation-wide. The present study attempts to provide more refined information on the fundamental characteristics of the population potentially in need of PPC.
The chosen place of death of these children depended on the disease category, age of the patient, and whether they lived in metropolitan or non-metropolitan areas. Considering that there are currently no home-based end-of-life care services for children in Korea, we interpret this finding cautiously because we could not find the healthcare services used near the end-of-life point. It is possible that death occurred suddenly, or that patients chose to breathe their last at home. PPC has developed with home care as one of the core services because children and families tend to prefer to be at home during end-of-life care.26 As home palliative care gradually evolves, the frequency of pediatric deaths due to CCCs occurring at home is increasing in the United States.27 Further research is needed to investigate the other factors that affect how patients suffering from CCCs and their families choose the place of death. Moreover, resources to conduct proper services in accordance with Korean culture need to be made available.
Why should PPC be provided? Wolfe et al.28 interviewed bereaved parents of cancer patients and showed that because of PPC, fewer children suffered from pain and dyspnea, and parents were more prepared during the last month of the child's life. Another report showed that the severity of the physical and psychological symptoms of the child was associated with higher levels of long-term parental grief, which implies that the effect of PPC extends after end-of-life.29 Although palliative care for children is applicable throughout the illness and may be congruent with maximal treatment for sustaining life, the role of palliative care for children is becomes more apparent at the end-of-life point when patients and their families experience extensive suffering. However, currently, no hospital or medical institution in Korea provides PPC by an adequate multidisciplinary team, and only 2 tertiary hospitals have attempted to set up special palliative care for children. These hospitals might plan to expand their program and equip themselves with better resources, but they can only provide specialized palliative services for children dying with CCCs living in Seoul, Incheon, and the Gyeonggi province. Therefore, more than half of the children dying because of CCCs cannot access palliative care services at a location within two hours of their residential location. To meet these regional needs, the health authorities must consider supporting the establishment of specialized palliative pediatric care centers in regional tertiary teaching hospitals, where most children with serious illnesses are treated. In addition, it is necessary to conduct research in order to develop an appropriate system of PPC for Korean pediatric patients and their families, and to educate medical personnel based on their needs.
The importance of providing quality care for patients at the end of life has recently been highlighted in Korea by legislation such as “the law on the hospice and palliative care and the determination of life-sustaining treatment for terminally ill patients,” which has come into force in 2017.30 It is anticipated that the implementation of this law would improve the development of palliative care services for a wide range of patients with life-threatening diseases and not just terminally-ill adult cancer patients. Despite a burgeoning concern for preserving human dignity at the end of life, far less attention has been focused on the trends of childhood mortality and the implied need for PPC implementation. Although longitudinal studies in cancer patients31 informed us of the trends of cancer specific incidence and deaths, no study, to the best of our knowledge, has analyzed comprehensive data on the pediatric mortality of life-threatening diseases in Korea. For these reasons, we examined all deaths among children aged 0 days to 19 years from 2005 to 2014 in Korea. To provide detailed information for the planning of PPC, we used the concept of CCCs for the analysis of population attributes. CCC classification was primarily developed by Feudtner and colleagues in 2000.3413 Classifying the causes of death due to CCC can help aggregate diverse pediatric health conditions into several distinct groups to provide more refined information on the evolving patterns and the changing needs of the pediatric patient population.
The present study has some limitations. First, we used the cause of death data from Statistics Korea. However, the variables of socioeconomic positions (SEPs), such as family income and level of education of parents, are not included in these databases, and therefore, we could not investigate the association between pediatric deaths and SEPs. Second, this was a cross-sectional study of annual pediatric deaths which would help us in understanding the need for end-of-life and bereavement care for children with CCCs and their families. The benefits of early implementation of PPC for children with CCCs have been emphasized in the present study, and it is important to understand the unmet needs of pediatric CCC patients living in Korea. Future research should seek to identify the prevalence, incidence, and healthcare utilization, as well as the PPC service needs, of patients with CCCs and their families.
Go to :
 XML Download
XML Download