

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hypertension is the most important risk factor for a variety of premature cardiovascular diseases (CVDs). Research has indicated that HIV infection increases blood pressure1 and that traditional CVD risk factors, such as hypertension, contributes additional risk, independent of and in addition to that contributed by HIV infection.2 While exposure to antiretroviral treatment (ART) has been reported to increase blood pressure with an odds ratio of 1.68, there is scarce data on whether a specific ART increases the risk.3
Abacavir, a first-line ART agent, has been on the market since 1998. In 2008, the Data Collection on Adverse Events of Anti-HIV Drugs (D:A:D) study reported an association between recent abacavir exposure and an increased rate of myocardial infarction.4 Nevertheless, studies have yet to confirm how and whether or not abacavir elevates CVD risk5678: it is necessary to confirm the long-term safety of abacavir use because, ultimately, people living with HIV (PLWH) will be on ART for decades. While one study has shown that, among several ARTs, only patients using abacavir exhibit a slightly higher risk of hypertension,9 no study has conducted a survival analysis of the hypertension risk associated with abacavir use in initial ART among PLWH over an extended follow-up duration.
In order to evaluate the risk of hypertension with abacavir use in comparison to non-abacavir ART, we analyzed a nationwide cohort of HIV-infected individuals on their initial ART from 2008–2016, considering drug exposure as a time-varying covariate measured on a daily basis.
MATERIALS AND METHODS
Data source
The National Health Insurance System (NHIS) in the Republic of Korea (ROK) began in 1963 and has been the single insurer of the entire population, currently about 52 million, since 2000. This study used data from the Health Insurance Review and Assessment Service (HIRA) database, which includes the claims data of the NHIS and National Medical Aid (NMA), which cover 97% and 3% of the entire population, respectively. The HIRA database includes all information regarding patient diagnosis (using the International Statistical Classification of Diseases and Related Health Problems 10th revision codes), names of procedures, drug prescriptions, health insurance status (NHIS or NMA), types and regions of medical institution visited, and health care costs.10 The HIRA database has been used in other research regarding hypertension1112 and in an ART adherence study.13 This database contains comprehensive data on the use of ART because, since 1989, all healthcare claims, including ART, are fully reimbursed when the condition claimed for their use is relevant to HIV infection.
Study population
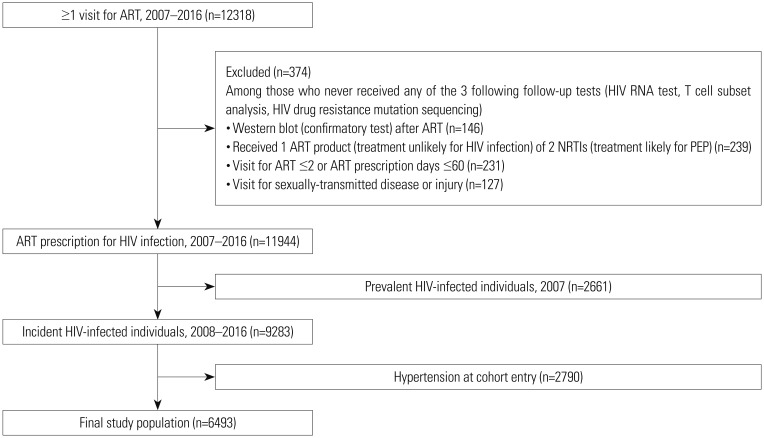
We used the 2007–2016 HIRA databases to establish a cohort of incident HIV-infected individuals on initial ART (Fig. 1). PLWH who received ART treatment at least once were defined as HIV-infected individuals, with an exclusion of those who were likely to have received ART for other preventive care and with a minimum of one year as the window period for defining incident cases. Eventually, 9283 incident HIV-infected individuals with initial ART prescription from 2008–2016 were recruited. After excluding 2790 (30.0%) individuals with prevalent hypertension at cohort entry, 6493 were included as the final study population. A similar method of selecting HIV-infected individuals was used in another study.13
Assessment of exposure and outcome definitions
Drug exposure was categorized into two groups (abacavir and non-abacavir ART), and the switch between the two were applied as a time-varying covariate on a daily basis. That is, the kind of ART (abacavir or non-abacavir ART) a participant received was assessed on a daily basis. When abacavir and nonabacavir ART were both prescribed for the same day, it was counted as abacavir exposure. Hypertension was defined as at least one claim for a visit with the main diagnosis of hypertension or prescriptions of antihypertensive treatment314, and outcomes within 9 months after cohort entry were excluded.15 The cohort entry day was the day of initial ART, and patients were followed until either incident hypertension or the last day of study period (December 31, 2016).
Potential confounders
All comorbidities and co-medications were defined based on information prior to cohort entry. The following confounders related to the probability of prescribing abacavir instead of tenofovir were adjusted for: acute kidney failure, end stage renal disease (ESRD), osteoporosis, and history of switching between abacavir and non-abacavir ART. Acute kidney failure comprised kidney ischemia or infection, as well as temporary proteinuria, while ESRD included chronic kidney disease and dialysis or transplant related status. Factors related to hypertension, such as alcohol drinking, diabetes, dyslipidemia, atherosclerosis, history of medications, such as antidiabetic agent or statins, and prior history of exposure to protein inhibitors (PIs) or nucleoside analogue reverse transcriptase inhibitors (NRTIs) known to increase CVD risk were also adjusted for. An individual with AIDS was defined as one who received at least one diagnosis of an AIDS-defining illness, defined by the Centers for Disease Control and Prevention.16 Requiring prophylactic antibiotics included having been prescribed a prophylactic dose of oral trimethoprim-sulfamethoxazole (80 mg/400 mg: 1 tablet daily, 1 tablet twice daily, or 2 tablets daily) or oral dapsone (100 mg daily or 200 mg weekly). We assumed that individuals requiring prophylactic antibiotics had a CD4+ T-cell count <200 cells/µL, since test results must meet strict indication criteria in order to receive support by the government. PIs with known CVD risk included lopinavir, indinavir, and darunavir (including ritonavir boosted products)17; NRTIs with known CVD risk included didanosine, stavudine, and zidovudine.418 Adherence was examined using the medication possession ratio, calculated as the sum of days of treatment supplied for all ART prescriptions filled, from the first ART fill date (the cohort entry date) until December 31, 2016, divided by the number of days in that same time period. NMA usage was considered a proxy for low socioeconomic status since they are considered to be the financially lowest 3% of the national population. Visiting medical institutions in metropolitan cities reflects better accessibility to healthcare including infectious disease specialists.
Statistical analysis
Our study objective was to evaluate the risk of hypertension with abacavir use in comparison to non-abacavir ART use over the period between 2008 to 2016. Demographic and clinical characteristics of patients with and without abacavir exposure were compared using Pearson's χ2 test for categorical variables. We calculated incidence rates of hypertension for abacavir users and non-abacavir ART users among the overall study population and among subgroups with known hypertension risk. Population attributable fraction (PAF) was calculated using the incidence rates and proportion of population at exposure. PAF reflects the proportion of disease in the population that can be attributed to a particular risk factor that, if eliminated, will potentially prevent the risk.1920 Abacavir risk is presented in hazard ratios (HRs) and 95% confidence interval (CI) using Cox proportional hazards models asdjusted for potential confounders mentioned above. Using the Cox models, we also identified risk factors of hypertension among the entire study population, as well as risk factors particularly critical in clinically important subgroups. An alpha of 0.05 was used for all the statistical hypothesis testing, and all statistical analyses were conducted using SAS Enterprise Guide, version 6.1 (SAS Institute, Inc, Cary, NC, USA). This study was approved by the Institutional Review Board of Seoul National University College of Medicine (IRB No. E-1710-070-893), and the need for informed consent was waived by the board.
Sensitivity analysis
Two kinds of sensitivity analyses were conducted. The first estimated hypertension risk in both abacavir and non-abacavir groups, compared to no ART exposure. In this analysis, intermittent time during the follow-up, either without abacavir or non-abacavir exposure, was defined as time with no ART exposure; drug exposure was applied in a daily base as a time-varying covariate as well. The second analysis estimated hypertension risk without excluding outcomes that occurred within 9 months after cohort entry.
RESULTS
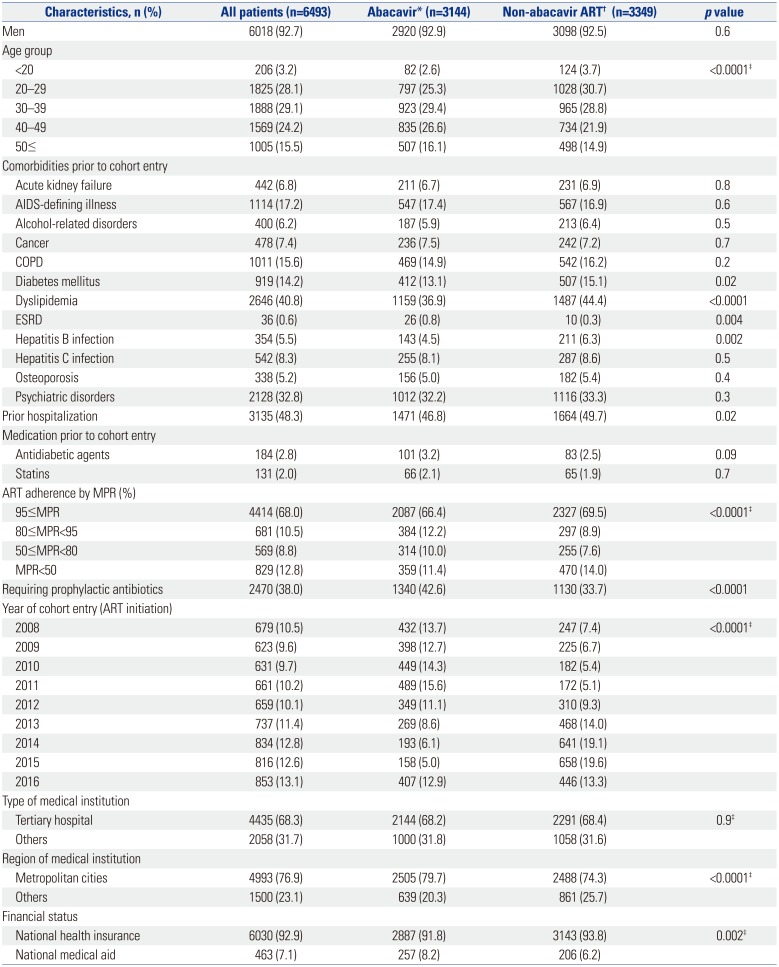
Of the 11944 nationwide HIV-infected individuals from the years 2007–2016, 6493 incident ART users without hypertension before cohort entry (initial ART) from 2008–2016 were selected as the final study participants (Fig. 1). Among them, 3144 (48.4%) had been exposed to abacavir at least once, while 3349 (51.6%) had never received abacavir (Table 1). Among the total study population, 1173 (18.1%) changed at least once from abacavir to non-abacavir and 1593 (24.5%) vice versa.
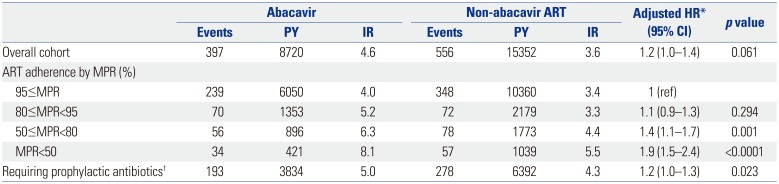
A total of 6493 participants were followed-up for 24072 person-years (PY), while 1599 (24.6%) developed incident hypertension during follow up from 2008 to 2016. However, after exclusion of outcomes within 9 months after the cohort entry from 646 individuals, 953 (14.7%) events occurred, resulting in incidence rates of 4.6, 3.6, and 4.0 per 100 PY among abacavir users, non-abacavir ART users, and the total HIV-infected individuals on ART, respectively (Table 2). PAF of abacavir on hypertension was calculated as 12%. Even though abacavir seemed to increase hypertension risk before adjustment, it lost statistical significance after adjustment (HR 1.2, p=0.061) (Supplementary Table 1, only online). However, poor ART adherence and requiring prophylactic antibiotics were statistically significant factors in the association between abacavir and hypertension (HR ranged from 1.1 to 1.9) (Table 2). In addition, in subgroups of the following characteristics, risk was statistically significant: men, aged ≥40 years, patients visiting tertiary hospitals, and patients visiting medical institutions in urban areas (HR ranged from 1.2 to 1.3) (Table 3). Among patients with history of PIs known to increase CVD risk, prior history of dyslipidemia and antidiabetic treatment were risk factors of hypertension increased by abacavir exposure (Table 4). In sensitivity analysis, defining intermittent non-ART exposure as the comparison group, the risk of hypertension was elevated both for non-abacavir ART (HR 2.8, 95% CI 2.0–3.8) and abacavir (HR 3.1, 95% CI 2.2–4.3) groups with statistical significance after adjustment (data not shown).
DISCUSSION
In this nationwide cohort of incident HIV-infected individuals on initial ART from 2008 to 2016, the incidence rates of hypertension were 4.6 per 100 PY among abacavir users and 3.6 per 100 PY for non-abacavir users. Users of abacavir showed a higher risk of hypertension than non-abacavir ART users only in some subgroups.
The incidence rate of hypertension from this study is comparable with the 4.6 per 100 PY reported among the general population, calculated from a study in the ROK.21 However, the incidence rate of hypertension among ART users from this study may be interpreted as higher than the general population because the cohort of HIV-infected individuals was a much younger group of people; individuals aged ≥50 years made up only 16% of the cohort, compared to 53% among the general population in 2017. The incidence rate in this study was higher than those from North American cohorts: 2.6 per 100 PY overall, 2.2 per 100 PY for non-Blacks, and 3.3 per 100 PY for Blacks among HIV-infected individuals on ART15 and 3.4 per 100 PY among heterogeneous PLWH including about 59% of Blacks and 90% on ART.22 Racial disparities in the occurrence of hypertension among PLWH was shown in other studies,1522 as well as among the general population.23
Abacavir did not elevate the risk of hypertension, compared to non-abacavir ART, and only elevated the risk among men and older adults who visited tertiary hospitals in urban areas. Old age2425 and being male25 were similar risk factors of hypertension among PLWH in other studies. Nevertheless, while financial status or accessibility to healthcare was not considered in the model, this study found that PLWH who visit institutions with specialty doctors in urban areas were more prone to being diagnosed with hypertension. This indicates a gap in the management of HIV-infected individuals, even though the financial barrier to treatment is very low in ROK. Additionally, in order to address concerns for the extent of the role of abacavir in incident hypertension, PAF was calculated in this study and was 12%. This indicates that, among a variety of risk factors affecting hypertension, about 12% occurred as the result of abacavir in HIV-infected individuals on ART. This size of PAF is comparable with the PAFs for CVDs in case of diabetes or high cholesterol (both, 13%) in the USA.26
In a Korean cohort of HIV-infected individuals, PI use was found to be a risk factor for dyslipidemia.272829 Interestingly, the risk of hypertension with abacavir use lacked significance among individuals who had received PIs with known CVD risk. However, prior history of dyslipidemia before cohort entry was a risk factor for developing hypertension among those who had ever received PIs with known CVD risk. This suggests that the hypertension risk associated with abacavir may be mediated through pathways other than dyslipidemia. In a recent meta-analysis, PLWH on ART showed lower heart rate variability, indicating parasympathetic dysfunction with a shift toward sympathetic dominance.30 Autonomic dysfunction was common among PLWH regardless of ART treatment; hence, whether this dysfunction serves as the plausible explanation for the higher risk of hypertension after abacavir use per se remains unclear.31 We propose that CVD risk of abacavir reported in several previous studies may also be mediated through hypertension due to autonomic dysfunction: previous studies mostly suggested vascular dysfunction.414323334
Antidiabetic agent use was a risk factor of hypertension among those who had received PIs with known CVD risk. PI has been shown to inhibit glucose transporter-4 in adipose tissue and muscle,29 and a systematic review has further suggested some detrimental effects of rosiglitazone on lipid profiles among PLWH on ART.35 This emphasizes an additional need to monitor lipid profiles of PLWH on diabetic treatment.
This study has strengths in its study design. First, it used approaches to take into account for immortal time bias36: time-dependent definition for the drug exposure and initial ART use requirement for the study population. This study treated drug exposure as a time-varying covariate measured in a daily unit to precisely reflect exposure, and it included incident HIV-infected individuals who were all starting their initial ART from a nationwide cohort, which provides high homogeneity and decreases survival bias. Second, we decided to evaluate the risk of cumulative exposure of hypertension risk to reflect current situations in the real world. In the case of CVD risk of abacavir, the issue was ‘when’ the risk became maximized. While some studies only reported recent (within 6 months) exposure as being a risk,41437 other studies reported this risk to be high after 3 years,3338 and in another study, the risk peaked after 13–24 months of exposure.32 However, currently, PLWH are not being recommended to change abacavir after a certain period of use. Therefore, PLWH on abacavir for many years were our main interest to ensure that the results can be generalized to those on abacavir for as long as 9 years. It was suggested that the duration of ART treatment may modify the association between ART and hypertension among PLWH.3 In addition, the study period was as long as 9 years and included the era of new combination ART agents in the market. In ROK, tenofovir/emtricitabine/elvitegravir/cobicistat (TDF/FTC/EVG/c) was released in 2014 and abacavir/lamivudine/dolutegravir (ABC/3TC/DTG) in 2015. Third, in seeking causal inference concerning the detrimental effect of abacavir, confounding by indication and channeling bias is particularly important, because switching of drugs is common. For example, the alternate treatment of choice for abacavir, tenofovir, is avoided in patients with poor renal conditions39; after the 2008 D:A:D publication,4 abacavir was avoided in patients with CVD risk.34 During the study period, patients who received abacavir as their initial ART were 897 (13.8%), and 2056 (31.7%) had changed ART between abacavir and non-abacavir ART with a maximum of 21 switching times. Therefore, we included a number of potential confounders that may affect treatment choice or outcomes. Potential confounders were defined based on the information before cohort entry in order to overcome reverse causation. In case of comorbidities, not only the primary diagnosis but all the other reasons for clinical visits were included. Lastly, while studies that excluded early outcomes since cohort entry to reduce detection bias are rare,1522 we excluded outcomes within 9 months after the cohort entry, since the sensitivity analysis showed that the results varied without the exclusion.
Our study has several limitations including the use of administrative database without information on smoking status or glomerular filtration rate (GFR). However, GFR did not seem to influence the association between abacavir exposure and CVD risk in a previous study.14 In addition, we included the history of acute kidney failure and ESRD prior to cohort entry in order to adjust for renal function and chronic obstructive pulmonary disease in order to adjust for smoking status using diagnostic codes that were strictly supervised by the government for reimbursement. Second, in selecting the study population, an arbitrary time of one year was used to identify incident PLWH on initial ART. Therefore, some HIV-infected individuals who never visited any medical institution could have been excluded. However, the number of yearly incident HIV-infected individuals selected in our cohort was similar to the number reported in an official government report.40 Third, in order to evaluate the potential population impact using PAF, there should be a causal relationship between the exposure and the outcome. However, as of yet, the mechanism between abacavir and hypertension remains unclear. Also, abacavir is not such an exposure that could be eliminated. Nevertheless, PAF enabled the evaluation of the quantitative risk of abacavir.
In conclusion, considering a PAF of 12%, abacavir use should be followed by regular monitoring on blood pressure among those with poor ART adherence, those who require prophylactic antibiotics, men, and older adults. Even though this study could not show a concrete result on the risk of hypertension of abacavir due to lack of statistical power, further study should be continued as HIV is now a chronic disease.


 XML Download
XML Download