

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
For many years, the gold standard for the restoration of endodontically treated teeth (ETT) with extensive loss of tooth structure has been the fabrication of metal-ceramic or all ceramic full coverage crowns, with or without the presence of a post [1]. Over the years, the importance of tooth tissue preservation along with the evolution of dental materials has introduced new principles in the restoration of teeth leaving aggressive macromechanical approaches aside [2].
These principles also apply to ETT, with the introduction of the endocrown as an alternative treatment modality. Pissis [3] in 1995 was the first to introduce the heat-pressed ceramic monoblock technique, which utilized the pulp chamber to increase the macromechanical retention of the crown. The development of computer-aided design/computer-aided manufacturing (CAD/CAM) technology has opened new horizons, both in material processing, as well as in the restoration of teeth, providing accuracy, esthetics, and less time consuming restorative procedure. In 1999 Bindl and Mörmann [4] evolved Pissis proposal and used the term ‘endocrown’ to describe a CAD/CAM all ceramic crown, macromechanically anchored to the internal portion of the pulp chamber and adhesively cemented to the remaining tooth structure, gaining micromechanical retention.
Initially, the materials for the fabrication of an endocrown were alumina or spinell reinforced non silica based ceramics and silica based feldspar ceramics [4], using either a heat-pressed technique or later CAD/CAM technology. Later, glass ceramics were the material of choice as they provide the advantage of surface modification, either with the use of hydrofluoric acid or air-abrasion, improving in that way their adhesion to the tooth tissues. According to the literature, glass ceramics reinforced either with leucite or lithium disilicate have been the best option for the fabrication of endocrowns, since they exhibit higher flexural strength than feldspathic glass ceramics and resin composite, and being able to withstand the occlusal forces during mastication [5678]. However, there is a lot of research in hybrid materials that, according to their manufacturers, combine the properties of resin composite and ceramic. As a result, many new CAD/CAM hybrid materials have been introduced in the market. According to recent literature, composite materials are more resilient than ceramics, a condition that may have a positive effect on the stresses transferred to the cavity walls [9].
As with any other restoration, the tooth preparation for an endocrown should follow specific guidelines. An overall reduction of 2 mm in height is necessary. A butt joint margin of 1–1.2 mm is suggested, but not always needed. All cervical margins should be placed as supragingivally as possible. In addition, an occlusal divergence of 5–7° is obligatory, in order for the coronal pulp chamber and the endodontic access cavity to be continuous [710]. However, modifications can be made, due to esthetic, biomechanical, and material-oriented reasons. These deviations include a smaller decrease in the axial height of the cusps especially when resin composite is used [2], the application of the immediate dentin sealing technique for higher bond strength [11], and the presence of a uniform or a non-uniform ferrule in the restoration in order to achieve higher fracture resistance [1213]. Although the increased fracture resistance, due to the addition of ferrule, has been documented scientifically [14], ferrule design is against minimally invasive dentistry. The purpose of this clinical case report was to evaluate the clinical performance of endocrowns and to compare the clinical characteristics of different preparation designs and restorative materials.
CASE REPORT
The following cases describe the restoration of ETT with endocrowns. The fabrication techniques used were either CAD/CAM or conventional laboratory technique. The materials selected were CAD/CAM glass ceramics, resin nano-ceramics, and conventional laboratory resin composite. The cementation procedures included the use of either total etch or self-adhesive dual cure resin luting materials, depending on the location of the margins and consequently the sensitivity of the bonding technique as well as the presence and amount of enamel. The modified United States Public Health Service (USPHS) criteria were used for rating the restorations at recall appointments (Table 1). Every endocrown was rated in a triple scale as followed: A, Alfa (clinically excellent restoration); B, Bravo (clinically acceptable restoration); and C, Charlie (clinically unacceptable restoration).
Table 1
Evaluation of endocrowns in recall appointments according to the modified United States Public Health Service (USPHS) criteria
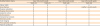
Ratings in USPHS: A, Alfa (clinically excellent restoration); B, Bravo (clinically acceptable restoration); C, Charlie (clinically unacceptable restoration).
![]()
Case 1
A 58-year-old male patient attended the postgraduate clinic of Operative and Aesthetic Dentistry after the completion of endodontic treatment of the upper right maxillary premolars (teeth #14 and #15). He was diagnosed with chronic advanced periodontitis, but his condition was stable after periodontal therapy. The patient was a smoker. Due to the excessive coronal tooth loss and the existence of a crack in the mesial part of tooth #14 as well as the periodontal condition, it was decided to restore these teeth with endocrown restorations made of a resin composite material with similar elastic properties to the tooth. It was also decided not to remove, but to cover the existing crack in order to avoid its expansion. In this case, laboratory fabricated resin composite endocrowns were selected. A butt joint margin of 1 mm was prepared, but no ferrule was created. Since resin composite was chosen, a 1.5 mm reduction of the occlusal surface took place. Undercuts were blocked by the use of conventional resin composite. The selection of shade before any intervention led to an A3 shade restoration (Figure 1). The marginal integrity and shade of the restoration were tested before cementation. A total etch dual cure resin luting cement (Variolink II, Ivoclar Vivadent, Schaan, Liechtenstein) was used due to the presence of adequate enamel on the supragingival margins of the preparation. The patient was reviewed at 6, 10, 12 and 20-month follow up periods. The restorations were characterized as acceptable, without any fractures (Figure 1G). There was no clinical evidence that the existing crack expanded. The color match for both restorations was rated as Bravo. In the endocrown of the first premolar, a marginal discoloration on the palatal side of the tooth was observed (Figure 1G). Interproximal contacts were also rated as Bravo, because of the periodontal mobility of the teeth. The rest of the USPHS criteria and the satisfaction of the patient were rated as Alfa (Table 1).

Case 2
A 55-year-old male patient with moderate periodontitis attended the postgraduate clinic of Operative and Aesthetic Dentistry seeking treatment of the first and second right mandibular molars (teeth #46 and #47), which were endodontically treated. On examination, extensive loss of tooth structure and very thin remaining walls were detected, especially on the first molar. After discussing the treatment options, it was decided to restore the first molar with an endocrown and the second molar with an onlay to replace the missing mesiolingual cusp. In this case, a ceramic material was chosen due to its superior aesthetics and fracture resistance, and a polychromatic feldspathic CAD/CAM material was used (CEREC Block PC, Sirona Dental Systems, Bensheim, Germany). The endocrown preparation margins were located on the gingival level of both enamel and dentin. The root canal sealing material was protected by a glass ionomer cement liner and the cavity was prepared according to the guidelines. A non-uniform ferrule of 1.2 mm was created on the buccal side of the tooth. A retraction cord was used and a precise digital impression was acquired using the Cerec system (CEREC 3D, Sirona Dental Systems). Staining and glazing followed. The intaglio surfaces of the restorations were treated with 5% hydrofluoric acid and a silane agent was applied. Since the margins were located at the gingival level, a less technique-sensitive resin luting cement was applied (Rely-X Unicem, 3M ESPE, St. Paul, MN, USA) (Figure 2). After the 6 and the 10-month follow up period, no alterations were observed (Figure 2F; Table 1).

Case 3
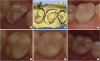
A 34-year-old female patient attended the postgraduate clinic of Operative and Aesthetic Dentistry with a severely fractured upper right first molar (tooth #16). A fracture of the mesio-palatal cusp associated with negative response to pulp vitality tests and sensitivity on percussion and palpation led to an endodontic treatment. Gingivectomy was performed in order to relocate the margins of the cavity as supragingivally as possible. The endocrown preparation followed four weeks after gingivectomy. Glass ionomer cement was used as a liner to cover the obturated orifices. A central inner cavity was formed for retention. A 1–1.2 mm reduction of both distopalatal and buccal cusps was made since a hybrid resin composite-ceramic material was going to be used (Shofu Block HC, Shofu Inc., Kyoto, Japan) [2]. A 1.2 mm non-uniform ferrule was created on the distobuccal part of the tooth. Retraction cord was placed in the mesial area and digital impression was followed. The adhesive material used was self-adhesive resin luting cement (Rely-X Unicem, 3M ESPE), since it is less technique sensitive. Before the 6-month recall appointment (at 5th month), a fracture of the material without any tooth interlocking was revealed (Figure 3D). Subsequently, the gross fracture was rated as Bravo, since the restoration was partially fractured with more than half of the restoration still intact and only a small part of the distopalatal cusp missing. The underlying tooth structure was cleaned and polished, and a bevel was formed at the margins of the remaining CAD/CAM resin nanoceramic crown which was later mechanically processed by the use of air-abrasion. In order to repair the fractured part of the restoration, acid etching was applied on both restoration margins and tooth structure, followed by placement of a silane agent and adhesive system on both tooth and restoration surfaces. Resin composite was placed (Figure 3E). In the 12-month recall appointment, the restoration was still functional and all the other evaluated criteria were rated as Alfa (Table 1).
DISCUSSION
The results of this clinical report indicated a successful short-term survival of this relatively new minimal invasive approach.
One of the findings was that the endocrowns fabricated with the CAD/CAM technique demonstrates superior anatomic contour and surface textures. This observation is in agreement with studies supporting that the morphology of CAD/CAM generated restorations are more compatible with the natural morphology of an intact tooth, compared to those fabricated by dental technicians using wax up technique [15]. Besides the superior anatomic properties provided by the CAD/CAM unit, a one-appointment and less time consuming treatment is counted as an advantage.
Another clinical observation was a slight color difference between sound tooth structure and the resin composite endocrown restorations of the maxillary premolars as well as a small area of marginal discoloration of the restoration in the first upper right maxillary premolar in the first clinical case, which possibly could be attributed to the patient's smoking habits and stain absorption [16]. No marginal discoloration was detected in the rest of the endocrown cases.
For the fabrication of endocrowns, specific preparation guidelines are suggested. An alteration on the design of the endocrown is possible to increase esthetics and physiomechanical properties of the final restoration. Among other factors, the restorative material influences the preparation design, regarding the overall reduction in the height of the occlusal surface. Fages et al. [10] recommended at least 2 mm reduction in the axial direction when a monoblock ceramic material is used, whereas Rocca et al. [2] suggested an overall reduction of 1 to 1.5 mm from the occlusal plane when resin composite is used, taking advantage of the material's elastic modulus and stress-absorbing properties similar to those of dentin [3]. In the first clinical case where resin composite was used, a reduction of 1.5 mm in height took place. After almost 2 years, no failures or debonding have been occurred. Contrarily, in the 3rd clinical case where a hybrid resin nanoceramic material was used and a reduction of 1–1.2 mm of the distopalatal cusp was applied, partial fracture of the restoration was observed after 5 months. A possible explanation to this could be that the 1–1.2 mm thickness of the resin nanoceramic CAD/CAM material used was not able to withstand occlusal and non–axial forces (masticatory forces) in the region of the distopalatal cusp, which is a functional cusp and receives extensive loadings.
The best clinical outcome was observed in the second clinical case where a feldspathic CAD/CAM glass-ceramic was used. After almost a year, every clinical characteristic was rated as Alfa. This finding strengthens the beliefs, presented in several clinical reports that recommend glass ceramic materials, that feldspathic, leucite reinforced, or lithium disilicate may be the most preferable materials for the fabrication of an endocrown due to the creation of a superior bond between resin cement and tooth tissues [1718]. However, the establishment of the ‘material of choice’ cannot be achieved since new generation materials are constantly being introduced. Ramírez-Sebastià et al. [9] in 2013 concluded that Cerec fabricated endocrowns made by millable resin composite blocks (MZ100 blocks, Paradigm, 3M ESPE) presented better marginal adaptation than leucite reinforced CAD/CAM glass ceramics (IPS Empress CAD, Ivoclar Vivadent). The new resin nanoceramic restorative materials present advantages related to their superior properties that resemble those of dentin, such as modulus of elasticity, less crack propagations, higher fracture resistance as opposed to ceramics that are more prone to fracture due to their brittle nature [8192021]. However, resin composite materials appear to have higher microleakage during time [22] and are weaker than lithium disilicate glass ceramics under non-axial loadings [23].
Regarding the preparation design used, the incorporation of a ferrule did not seem to have any great influence on the clinical outcome of an endocrown. In the first clinical case, butt joint margins were created with no ferrule design, whereas in the other 2 cases a ferrule was prepared only on one side of the tooth, while a flat preparation was prepared on the other side of it. Although the preparation of a ferrule is opposed to minimal invasive principles, it has the ability to simultaneously increase the dentin surface available for adhesion in cases of severely damaged teeth, as crown lengthening is usually required. According to Einhorn, the ferrule design in an endocrown may increase the failure load resistance. However, this was an in vitro study and catastrophic failures occured only at forces above those of the normal masticatory function. No differences in the fracture resistance were observed if the endocrown was prepared with or without ferrule [12]. However, caution is recommended concerning the complexity of the preparation. The addition of a ferrule or the increase of the cavity depth and the intraradicular extension are the causes that can increase the discrepancies and lower the adaptation of the restoration in the prepared cavity [122024].
The type of tooth accepting an endocrown is another area of concern regarding the success of these restorations. Bindl et al. [7] reported in 2005 that endocrowns are inadequate for premolars, having a failure incidence of 31%, which showed a strong correlation with the surface available for adhesion. Likewise, many researchers support that endocrowns must be limited to molars [2325]. As opposed to the aforementioned statement, Lin et al. [26] in 2010 confirmed that according to 3 dimensional finite element analysis (FEA), the use of endocrowns in maxillary premolars is possible. Although, it should be taken into account that FEA is a computerized in vitro study in which clinical condition may not be completely replicated [27]. However, Belleflamme et al. [11] in 2017 endorsed clinically and concluded that the fabrication of endocrowns is a reliable approach for restoring both molars and premolars, even in the presence of extensive loss of tooth structure or occlusal risk factors. In our 2 clinical cases of maxillary premolar endocrowns, no failure was observed after 20 months even though a smaller surface for adhesion was available. Non axial forces because of the location of the tooth in the arch and the participation of premolars in lateral occlusal guide did not have major influence on the clinical outcome of the restoration. This may be explained by the fact that composite resins show a lower elastic modulus and may present higher long term survival rates for endocrown-restored maxillary premolars compared to leucite reinforced glass ceramics [8]. This is in accordance with Magne's statement that “composite resin presents better fatigue resistance compared to ceramics” [2829].
All in all, the few clinical trials available today show clinical success rate of endocrowns that varies from 94%–100% in a 36-month period [30], while their 10-year survival rate was set to 98.8% [11]. Otto et al. [31] in 2015 concluded that the survival rate of Cerec fabricated feldspathic endocrowns in molars and premolars was set to 90.5% and 75% respectively, in a 12-year follow up period.
CONCLUSIONS
The findings of this clinical report indicate that the clinical survival of endocrowns up to a 20-month follow up period is more than satisfactory, leading to the conclusion that this type of restoration is a possible viable alternative and a more minimal invasive therapeutic regimen for ETT. However, scarce clinical evidence and short follow up periods available in the literature do not help us draw clear conclusions about the clinical performance of such restorations. Four main factors account for the success and longevity of endocrowns: correct preparation of the tooth, precise selection of restorative and bonding materials, and careful selection of cases including tooth category, margin locations, and remaining sound tissue. Nevertheless, long term clinical trials to evaluate the performance of these restorations are of paramount importance in order to establish this restorative modality as a viable option.
 XML Download
XML Download