

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Melanomas are malignant tumors that arise from melanocytes or pigment cells. Most are cutaneous tumors; however, they can be extracutaneous depending upon the location of melanocytes. Extracutaneous melanomas can be ocular, leptomeningeal, or mucosal [1]. Primary malignant vaginal mucosal melanoma is very rare and has an aggressive clinical course. It arises from melanocytes found in the basal portion of vaginal epidermis as embryological remnants of neural crest cells found in around 3% of healthy women, and constitutes 0.3% to 0.8% of melanomas in women and fewer than 3% of vaginal malignant tumors [2]. Among these, amelanotic melanoma is a unique variant due to the absence of melanin pigmentation and accounts for only 2% of all vaginal melanomas [3]. The diagnosis is difficult without immunohistochemistry. We present a rare case of primary amelanotic malignant vagina melanoma, confirmed on immunohistochemistry based on the presence of human melanoma black 45 (HMB45) and S-100.
Case report
A 53-year-old woman who was menopausal for 10 years presented with postmenopausal bleeding for 4–5 months. On examination, her abdomen was unremarkable, but vaginal examination revealed a friable growth of the posterior wall extending up to the fornices, whereas the anterior wall and cervix appeared normal. The growth was white in color with areas of hemorrhage, soft in consistency, and bled easily on touch. A biopsy was taken. Microscopic examination (Fig. 1) showed soft tissue fragments lined by acanthotic stratified squamous epithelium with extensive areas of ulceration. A malignant tumor was seen in the subepithelium, arranged in nests, alveoli, trabeculae, and as singly scattered cells, separated by thin fibrous septa. A radial pattern of growth with junctional activity was present. Tumor cells were markedly pleomorphic, round to polygonal or spindle-shaped, and had eccentrically placed nuclei with conspicuous nucleoli along with scant to moderate cytoplasm. Focal intranuclear inclusions, eosinophilic macronuclei, nuclear grooving, intracellular/extracellular, hyaline globules and few binucleated/multinucleated giant cells were seen as well. Numerous atypical and bizarre mitotic figures were noted. There was a lymphocytic infiltrate and large areas of necrosis. Lymphovascular emboli were seen. Immunohistochemistry (Fig. 2) was used to confirm the diagnosis. Tumor cell cytoplasm was strongly-positive for HMB45 and vimentin, and both nucleus and cytoplasm were positive for S-100. Cells were negative for cytokeratin. The final diagnosis was primary vaginal amelanotic melanoma based on final cutaneous and ocular examination. Chest computed tomography was suggestive of metastatic nodules in bilateral lungs. Multi-agent chemotherapy (cisplatin and adriamycin) and hypofractionated radiotherapy were initiated.
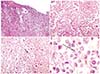
Fig. 1
Hematoxylin and eosin stained sections show (A) a tumor in the subepithelium with junctional activity and surface ulceration. (B) Tumor cells arranged in cords with intervening thin fibrous septa. Cells are plasmacytoid with eccentrically-placed nuclei and abundant cytoplasm. (C) Numerous mitotic figures (arrow). (D) Tumor cells have prominent eosinophilic nuclei and few hyaline globules (arrow).

Discussion
Malignant melanomas are cutaneous and extracutaneous tumors arising from melanocytes, which are embryological remnants of neural crest cells. Most melanocytes are located in the epidermis and dermis, but are also found in many other locations including the eye, leptomeninges, oral mucous membranes, esophagus, rectum, anal canal, nasal cavity, paranasal sinuses, larynx, vagina, and cervix [1]. Primary vaginal malignant melanomas are rare and aggressive tumors. Only 500 cases have been reported [2], principally affecting postmenopausal women, with a mean age of 57 years [4]. Mucosal melanomas are more often associated with KIT gene mutations rather than BRAF mutations, which are more often found in cutaneous melanomas [5]. Primary malignant vaginal melanoma usually occurs in the anterior wall, typically in the lower one-third. Common clinical presentations are abnormal vaginal bleeding, an easily palpable vaginal mass, pain, and discharge from the vagina [36]. On visual inspection, these tumors appear as nodular and polypoidal masses that are easily palpable and usually ulcerated, and bleed on touch. They are often pigmented masses, however amelanotic tumors lead to misdiagnosis and delayed treatment [1]. Amelanotic appearance is not rare among mucosal lesions, but makes diagnosis even more difficult. When pigment is absent, even microscopic diagnosis is difficult. Immunohistochemical staining positive for protein S-100, HMB45, Melan-A, Mart-1, and tyrosinase support a diagnosis of melanoma. Therefore, biopsies and immunohistochemical analysis are mandatory in such cases. When diagnosing primary mucosal melanoma, especially in uncommon locations, it is of crucial importance to exclude metastatic lesion from primary cutaneous or ocular melanoma. Whole-body skin examination and ophthalmic examination are crucial. The presence of in situ melanoma/junctional components or a radial growth phase is important for distinguishing primary lesions from metastases or intact epithelium overlaying invasive melanoma. However, because of hidden locations and lack of early symptoms, diagnosis of mucosal melanomas is usually delayed and many lesions are ulcerated at diagnosis; therefore, this criterion is not easy to assess. Hence, the absence of junctional change in an ulcerated lesion does not preclude the possibility of a primary melanoma [78]. As these cases are uncommon and rarely reported, definitive treatment guidelines are lacking. The Food and Drug Administration (FDA) previously approved interleukin-2 and dacarbazine for distant metastasis; in clinical trials, each had response rates of 10–20% without improving overall survival benefit. Presently, ipilimumab, a fully-humanized antibody that binds to cytotoxic T-lymphocyte-associated antigen 4, has been approved by the FDA for use in metastatic disease [9].
In conclusion, amelanotic vaginal melanomas are rare tumors and can be easily misdiagnosed on clinical examination as well as on imaging. Therefore, biopsy, histopathological examination, and immunohistochemistry are mandatory for a conclusive diagnosis.
 XML Download
XML Download