

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Human listeriosis is a foodborne infection mostly caused by Listeria monocytogenes, a gram-positive non-spore-forming rod-shaped bacterium that can survive a wide range of temperature, acidity, and salinity. It is ubiquitously present in the soil, decaying matter, and the feces of various animal species, and it contaminates raw products and processed foods [1]. The burden of listeriosis is increasing globally. It is the most common cause of food-related deaths in the United Kingdom, and maternal-neonatal listeriosis commonly causes early neonatal infection with high fatality [234].
Listeriosis is rare with an annual incidence of 0.3 per 100,000 in the general population [5]. It poses the greatest risk to the elderly, immunocompromised patients, pregnant women, and fetuses/neonates, with increased susceptibility and severe invasiveness. Pregnancy-associated listeriosis, defined as listeriosis in the pregnant women, fetus, and neonates, is estimated to be 12–20 times more prevalent than listeriosis in the general population, accounting for up to 35% of all cases [6]. Clinical features of pregnant mothers with listeriosis are often mild or asymptomatic, while the effects on the fetus or neonate are fatal, leading to miscarriage, stillbirth, preterm birth, and systemic infection of neonates with mortality rates of 20–30% [67].
Several guidelines for the management of pregnancy-associated listeriosis have been suggested but remain controversial [78]. Furthermore, the management of listeriosis is clinically challenging because it is rare with nonspecific maternal features, but commonly results in severe neonatal outcomes. Herein, we report our experience of maternal bacteremia with chorioamnionitis due to listeriosis with the related literatures.
Case report
1. Case 1
A 25-year-old Korean singleton nullipara presented with fever (38.7°C), nausea, loose stool, nasal stiffness, and myalgia at 36 weeks and 5 days gestation. She had no notable events during the antenatal care of the current pregnancy. Her medical history included a miscarriage and gastroesophageal reflux disorder treated intermittently with antacid. Her vital signs were normal except for the fever. Fetal ultrasound and electronic fetal monitoring were unremarkable. A workup for fever was performed to test for gastroenteritis, upper respiratory infection, and chorioamnionitis. Cervicovaginal examination with a speculum was unremarkable with no evidence of membrane rupture. After the patient's urine and vaginal swab revealed absence of pathogens, a blood culture was performed. Initially, leukocytosis (11.5×106 mg/L) with a C-reactive protein (CRP) level of 2.97 mg/L was observed. There was no evidence of influenza infection in the related test results. Considering the effects of maternal fever on the fetus, empirical antimicrobials were started with intravenous cefazolin at 3 g/day. On day 3, the fever persisted, with a higher CRP level of 5.9 mg/L, and the antimicrobial was changed to intravenous ampicillin/sulbactam at 6 g/day. On day 5, the fever was partially controlled, but she felt reduced fetal movement. A 3.2-kg boy was born via emergent cesarean section at 37 weeks and 2 days gestation, and he appeared grossly normal with 1-minutes and 5-minutes Apgar scores of 7 and 9, respectively. The amniotic fluid was meconium-stained, and the pathological examination of the placenta was performed. After delivery, gentamicin was added for the prophylaxis of puerperal infection and was continued until discharge. Her fever resolved on postoperative day 3. Laboratory tests were performed for the neonate concerning the maternal condition and were negative for all parameters except for an elevated CRP level of 0.9 mg/L. He was administered intravenous ampicillin and was discharged with his mother on the 5th day of life. Maternal blood cultures, however, revealed the growth of L. monocytogenes, and re-examination of the placenta for listeriosis, which was initially reported as chorioamnionitis, revealed multiple microabscesses with focal necrosis and hemorrhage (Fig. 1A-C). With Brown & Brenn staining, gram-positive bacteria were confirmed (Fig. 1D). The neonate was hospitalized for further invasive evaluation for listeriosis and treatment with ampicillin for another 10 days; all tests were negative. Maternal oral amoxicillin therapy was continued for another 10 days, and the subsequent blood culture was negative for L. monocytogenes. The neonatal condition was unremarkable during the regular check-up for late-onset disease until 6 months of age.
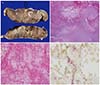
Fig. 1
(A) Multiple abscess formation in the placental sections. The histological examination results show a necrotic area (B, original magnification ×12), the villus destroyed by the inflammation, and fibrinogen (C, original magnification ×200). The Brown & Brenn staining shows multiple bacilli. This confirms the presence of Listeria monocytogenes (D, original magnification ×1,000).
2. Case 2
A 34-year-old primigravida without medical history presented with decreased fetal movement at 29 weeks and 6 days gestation. Her initial vital signs were normal except for mild fever (37.9°C). Fetal assessment revealed fetal tachycardia of around 180 bpm with minimal variability and no end-diastolic flow on the umbilical artery Doppler ultrasonography. Emergency cesarean delivery was performed, and a 1.8-kg dead female neonate with an Apgar score of 0/0 at 1/5 minutes was delivered. One week prior, she had shared sandwiches with her husband and brother, who were subsequently treated with enteritis for severe diarrhea and fever. She had no symptoms other than loose stool and febrile sense; therefore, she was not treated. L. monocytogenes was confirmed in the maternal blood culture on day 3 and identified in the placental tissue and swabs of the neonate's skin. She was treated with ampicillin and gentamicin and discharged uneventfully.
Discussion
Listeriosis is more prevalent and severe in pregnant women than in the general population, which can be attributed to pregnancy-induced maternal T-cell suppression and the ability of Listeria, with its various virulence factors, to facilitate entry into host cells and escape intracellular degradation by the host immune system. The placenta plays a role in protecting the fetus from external stimulation, but once bacteria have invaded the intervillous space, it may become a nidus for the repeated shedding of the bacteria to the mother and fetus, leading to recurrent infections [19].
Unfortunately, there is no standard diagnostic test for listeriosis. The culture of sterile samples, such as the blood and cerebrospinal fluid, but not of the stool due to its low sensitivity, is effective only for febrile and symptomatic patients because the infected dosage determines the positive predictive rate and duration of the culture result [910]. Microbiological diagnosis may lead to disparity in the detection rate, due to the unavailability of Listeria-specific agar in most clinical laboratories and the difficulty of the Listeria culture, which requires microaerophilic conditions or a relatively low temperature for proliferation [91011]. A prospective study reported that the placental culture was the most sensitive among the various sample cultures and other tests for maternal-neonatal listeriosis [11]. Amniocentesis has been proposed as a fast alternative for detecting gram-positive rods in the amniotic fluid [12]. The maternal blood culture took about 48 hours to show changes in case 2 and longer than 1 week in case 1. The infected amount was larger in case 2 than in case 1, which might have affected the neonatal outcomes.
The placenta affected by listeriosis shows characteristic pathologic findings, including macroabscesses or microabscesses with focal necrosis and hemorrhage [9]. However, the relevant investigation and early treatment are not performed due to nonspecific maternal symptoms, including flu-like symptoms, preterm labor, and reduced fetal movement. In neonatal listeriosis, 90% of all cases and 50% of fatal cases occur in the context of nonspecific maternal symptoms [13]. Retrospective placental examination has also led to the detection of more cases of listeriosis, although only half of the neonatal cases undergo placental examination [3]. In case 1, placental listeriosis was confirmed by re-examination with additional special staining, after maternal bacteremia was revealed.
The transmission of Listeria to neonates occurs mostly via congenital infection through transplacental transfection, an ascending infection from the colonized vagina, and, rarely, via horizontal infection from the mother or a nosocomial infection [6910]. It manifests as preterm birth, dyspnea, pneumonia, bacteremia, and meningitis in neonates, as well as neonatal death. The onset of listeriosis can occur at any time from 3–70 days after exposure, and the typical incubation period for the invasive disease is longer in pregnant women (2–4 weeks) than in non-pregnant persons (1–10 days) [6913]. Therefore, the neonates of affected mothers should be followed-up for another 2–3 months after birth.
The recommended antimicrobials for listeriosis treatment are high-dose intravenous ampicillin (6–12 g/day) or oral amoxicillin 100 mg/kg/day for at least 14 days [78]. When there is allergy to penicillin, the alternatives are erythromycin, trimethoprim/sulfamethoxazole, vancomycin, and fluoroquinolones [7]. The use of gentamicin with ampicillin/amoxicillin improves the survival rate in invasive listeriosis [1114], although it has no efficacy against intracellular Listeria in macrophages. As in previous reports and case 1, the appropriate type and dosage of antimicrobials should be emphasized [36811], especially since cephalosporin is most commonly administered for maternal inflammatory conditions to treat more common conditions, such as group B Streptococcus and Escherichia coli infections but is not effective for Listeria infection. According to the recent guideline for the intrapartum management of intra-amniotic infection, the combination of ampicillin and gentamicin is suggested as the primary empirical treatment [15].
The current published guidelines provide strategies and indications for the testing and treatment of febrile or symptomatic women exposed to Listeria but do not provide treatment strategies for asymptomatic women suspiciously exposed to Listeria [89]. The French guidelines, however, recommend a workup for fever and the commencement of amoxicillin treatment for every febrile pregnant woman, even without establishing Listeria exposure [8]. Most pregnant women with listeriosis have no history of immunocompromising disease or the ingestion of potentially contaminated foods, and they also have a low level of awareness concerning the risk of foodborne infections [4810].
In conclusion, early identification of listeriosis in pregnancy is challenging owing to the rarity of the infection and typically nonspecific maternal features. Moreover, the disease is not reported in South Korea. However, considering the high mortality rates and severe morbidity in neonates, which require further follow-up, clinicians should consider the possibility of listeriosis when investigating and administrating empirical antimicrobials for unexplained maternal inflammation.
 XML Download
XML Download